Why is cancer called cancer? We need to go back to Greco-Roman times for the answer
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
One of the earliest descriptions of someone with cancer comes from the fourth century BC. Satyrus, tyrant of the city of Heracleia on the Black Sea, developed a cancer between his groin and scrotum. As the cancer spread, Satyrus had ever greater pains. He was unable to sleep and had convulsions.
Advanced cancers in that part of the body were regarded as inoperable, and there were no drugs strong enough to alleviate the agony. So doctors could do nothing. Eventually, the cancer took Satyrus’ life at the age of 65.
Cancer was already well known in this period. A text written in the late fifth or early fourth century BC, called Diseases of Women, described how breast cancer develops:
hard growths form […] out of them hidden cancers develop […] pains shoot up from the patients’ breasts to their throats, and around their shoulder blades […] such patients become thin through their whole body […] breathing decreases, the sense of smell is lost […]
Other medical works of this period describe different sorts of cancers. A woman from the Greek city of Abdera died from a cancer of the chest; a man with throat cancer survived after his doctor burned away the tumour.
Where does the word ‘cancer’ come from?

The word cancer comes from the same era. In the late fifth and early fourth century BC, doctors were using the word karkinos – the ancient Greek word for crab – to describe malignant tumours. Later, when Latin-speaking doctors described the same disease, they used the Latin word for crab: cancer. So, the name stuck.
Even in ancient times, people wondered why doctors named the disease after an animal. One explanation was the crab is an aggressive animal, just as cancer can be an aggressive disease; another explanation was the crab can grip one part of a person’s body with its claws and be difficult to remove, just as cancer can be difficult to remove once it has developed. Others thought it was because of the appearance of the tumour.
The physician Galen (129-216 AD) described breast cancer in his work A Method of Medicine to Glaucon, and compared the form of the tumour to the form of a crab:
We have often seen in the breasts a tumour exactly like a crab. Just as that animal has feet on either side of its body, so too in this disease the veins of the unnatural swelling are stretched out on either side, creating a form similar to a crab.
Not everyone agreed what caused cancer

In the Greco-Roman period, there were different opinions about the cause of cancer.
According to a widespread ancient medical theory, the body has four humours: blood, yellow bile, phlegm and black bile. These four humours need to be kept in a state of balance, otherwise a person becomes sick. If a person suffered from an excess of black bile, it was thought this would eventually lead to cancer.
The physician Erasistratus, who lived from around 315 to 240 BC, disagreed. However, so far as we know, he did not offer an alternative explanation.
How was cancer treated?
Cancer was treated in a range of different ways. It was thought that cancers in their early stages could be cured using medications.
These included drugs derived from plants (such as cucumber, narcissus bulb, castor bean, bitter vetch, cabbage); animals (such as the ash of a crab); and metals (such as arsenic).
Galen claimed that by using this sort of medication, and repeatedly purging his patients with emetics or enemas, he was sometimes successful at making emerging cancers disappear. He said the same treatment sometimes prevented more advanced cancers from continuing to grow. However, he also said surgery is necessary if these medications do not work.
Surgery was usually avoided as patients tended to die from blood loss. The most successful operations were on cancers of the tip of the breast. Leonidas, a physician who lived in the second and third century AD, described his method, which involved cauterising (burning):
I usually operate in cases where the tumours do not extend into the chest […] When the patient has been placed on her back, I incise the healthy area of the breast above the tumour and then cauterize the incision until scabs form and the bleeding is stanched. Then I incise again, marking out the area as I cut deeply into the breast, and again I cauterize. I do this [incising and cauterizing] quite often […] This way the bleeding is not dangerous. After the excision is complete I again cauterize the entire area until it is dessicated.
Cancer was generally regarded as an incurable disease, and so it was feared. Some people with cancer, such as the poet Silius Italicus (26-102 AD), died by suicide to end the torment.
Patients would also pray to the gods for hope of a cure. An example of this is Innocentia, an aristocratic lady who lived in Carthage (in modern-day Tunisia) in the fifth century AD. She told her doctor divine intervention had cured her breast cancer, though her doctor did not believe her.

From the past into the future
We began with Satyrus, a tyrant in the fourth century BC. In the 2,400 years or so since then, much has changed in our knowledge of what causes cancer, how to prevent it and how to treat it. We also know there are more than 200 different types of cancer. Some people’s cancers are so successfully managed, they go on to live long lives.
But there is still no general “cure for cancer”, a disease that about one in five people develop in their lifetime. In 2022 alone, there were about 20 million new cancer cases and 9.7 million cancer deaths globally. We clearly have a long way to go.
Konstantine Panegyres, McKenzie Postdoctoral Fellow, Historical and Philosophical Studies, The University of Melbourne
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Astrology, Mental health and the Economics of Well Being

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Ultimately can the mental health system single-handedly address the concerns of inequality and economic access in society?
Around 75 per cent of the Indian population lives in rural areas, but their access to quality mental health care is limited and traditional approaches continue to be in use. The shortage is to such a large extent that there are only 0.7 physicians per 1000 population and only one psychiatrist for every 343,000 Indians. While over the years the mental health sector has seen major developments, like the 2017 mental health care act. This act establishes equal access for all citizens, to avail government-run or funded mental health services in the country. However, it does not bridge the gap in society as the majority of the population remains deeply unaware or unable to access these services.
While the uncertainties of the pandemic brought mental wellbeing to the forefront, the national budget for the sector dropped, making this an issue of human rights. This accessibility to services is further corroborated by the recurring financial expenses of medications and frequent visits to government clinics. The cost of sessions is steep and a single session is not ideal. Spending exorbitant amounts on healthcare is a burden most families can’t afford leading to debt. In the absence of insurance and healthcare schemes and provisions, therapy remains a luxury to many Indians.
Economic struggles are only one of the causes of this discerning gap in the mental health sector. Barriers caused by sexuality, gender, caste and religion also play a major role in mediating people’s perception and access to therapeutic services. The persistent stigma surrounding mental health, especially in India continues to be a hindrance to seeking help. The supernatural inhibitions and disparity in knowledge across communities only create more confusion. The notion that mental well being is an optional expense is popular, even though the country’s population is in a dire state. Data collected in a WHO report found that nearly 15 per cent of Indian adults need active intervention for one or more mental health issues.
The population disregards the very prevalence of such mental disorders and more than often finds it fruitless to receive treatment. Some who are open-minded fail to afford the hiked fees that therapists in urban settings charge, leaving them with no option. While for years Indians attributed the systemic weakness of the mental health system to the people’s attitudes, a 2016 survey showed more than 42% of people have positive attitudes toward mental wellbeing and treatment. While the skeptics remain, these underprivileged sections of society too struggle to gain the accessibility they deserve.
This is where astrology, tarot card reading and other spiritual practices, have created a market for themselves in the well-being industry. The sceptics, and those from poor socio-economic backgrounds resort to these local and easily accessible ways of coping, to instil the faith they so desperately need. Astrology is a layman’s substitute for therapy, or for some even a supplement when they cannot afford extended periods of treatment. Visiting a local astrologer in many ways breeds the self-awareness one would expect from a session in therapy. These practices even hold certain similarities to actual psychotherapy settings, in the way they define, and alleviate aspects of one’s personality and behaviour.
Very often one simply needs an explanation, or an answer to the ‘why’ no matter how scientifically rooted that response truly is. Astrologers impart a level of faith, that things will get better. For those in rural areas, struggling to provide the bare necessities to their family affording therapy is impossible, so their local psychic, astrologer or pandit becomes their anchor during emotional duress. Tarot cards and other practices primarily focus on the future and act as a guide point for how to deal with the things ahead. For a farmer coping with anxiety, access to anti-anxiety medication is strained, and so is therapy. His best bet remains to consult his next-door jyotish about his burdens.
A famous clinician Caroline Hexdall in an interview said that “ Part of the popularity of astrology and tarot today has to do with their universal nature”. With growing technology and the pervasiveness of social media, people can gain easy access to self-care and astrology resources. Apps and web pages provide daily tarot cards, zodiac signs readings and astrological predictions for people, and almost serve the purpose of a therapist. Is reading the lines on our palm, and checking the alignment of the stars enough to cure the mental illness they undergo? Is it a solution or a quick fix as a consequence of an ignorant healthcare system?
Several studies have also shown the deteriorating effects of depending on astrology. Cases of worsening and onset of depression, anxiety and personality disorders are common for those who use astrology as more than just a temporary coping mechanism. It also becomes a source of losing control, as every feeling is attributed to fate and destiny, instilling a sense of helplessness. Ultimately can the mental health system single-handedly address the concerns of inequality and economic access in society?
Maahira Jain is a third-year student at Ashoka University studying Psychology and Media studies. She is a movie buff and is extremely passionate about writing and traveling.
This article is republished from OpenAxis under a Creative Commons license. Read the original article.
Share This Post
-

The Brain-Gut Highway: A Two-Way Street
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The Brain-Gut Two-Way Highway

This is Dr. Emeran Mayer. He has the rather niche dual specialty of being a gastroenterologist and a neurologist. He has published over 353 peer reviewed scientific articles, and he’s a professor in the Departments of Medicine, Physiology, and Psychiatry at UCLA. Much of his work has been pioneering medical research into gut-brain interactions.
We know the brain and gut are connected. What else does he want us to know?
First, that it is a two-way interaction. It’s about 90% “gut tells the brain things”, but it’s also 10% “brain tells the gut things”, and that 10% can make more like a 20% difference, if for example we look at the swing between “brain using that 10% communication to tell gut to do things worse” or “brain using that 10% communication to tell gut to do things better”, vs the midpoint null hypothesis of “what the gut would be doing with no direction from the brain”.
For example, if we are experiencing unmanaged chronic stress, that is going to tell our gut to do things that had an evolutionary advantage 20,000–200,000 years ago. Those things will not help us now. We do not need cortisol highs and adrenal dumping because we ate a piece of bread while stressed.
Read more (by Dr. Mayer): The Stress That Evolution Has Not Prepared Us For
With this in mind, if we want to look after our gut, then we can start before we even put anything in our mouths. Dr. Mayer recommends managing stress, anxiety, and depression from the head downwards as well as from the gut upwards.
Here’s what we at 10almonds have written previously on how to manage those things:
- No-Frills, Evidence-Based Mindfulness
- How To Set Anxiety Aside
- The Mental Health First-Aid You’ll Hopefully Never Need
Do eat for gut health! Yes, even if…
Unsurprisingly, Dr. Mayer advocates for a gut-friendly, anti-inflammatory diet. We’ve written about these things before:
…but there’s just one problem:
For some people, such as with IBS, Crohn’s, and colitis, the Mediterranean diet that we (10almonds and Dr. Mayer) generally advocate for, is inaccessible. If you (if you have those conditions) eat as we describe, a combination of the fiber in many vegetables and the FODMAPs* in many fruits, will give you a very bad time indeed.
*Fermentable Oligo-, Di-, Monosaccharides And Polyols
Dr. Mayer has the answer to this riddle, and he’s not just guessing; he and his team did science to it. In a study with hundreds of participants, he measured what happened with adherence (or not) to the Mediterranean diet (or modified Mediterranean diet) (or not), in participants with IBS (or not).
The results and conclusions from that study included:
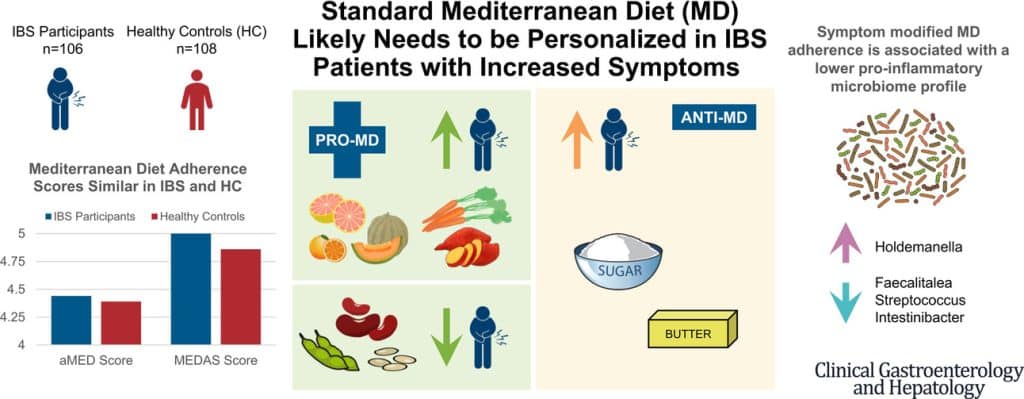
❝Among IBS participants, a higher consumption of fruits, vegetables, sugar, and butter was associated with a greater severity of IBS symptoms. Multivariate analysis identified several Mediterranean Diet foods to be associated with increased IBS symptoms.
A higher adherence to symptom-modified Mediterranean Diet was associated with a lower abundance of potentially harmful Faecalitalea, Streptococcus, and Intestinibacter, and higher abundance of potentially beneficial Holdemanella from the Firmicutes phylum.
A standard Mediterranean Diet was not associated with IBS symptom severity, although certain Mediterranean Diet foods were associated with increased IBS symptoms. Our study suggests that standard Mediterranean Diet may not be suitable for all patients with IBS and likely needs to be personalized in those with increased symptoms.❞
In graphical form:

And if you’d like to read more about this (along with more details on which specific foods to include or exclude to get these results), you can do so…
- The study itself (full article): The Association Between a Mediterranean Diet and Symptoms of Irritable Bowel Syndrome
- Dr. Mayer’s blog (lay explanation): The Benefits of a Modified Mediterranean Diet for Irritable Bowel Syndrome
Want to know more?
Dr. Mayer offers many resources, including a blog, books, recipes, podcasts, and even a YouTube channel:
Share This Post
-

Coach’s Plan – by Mike Kavanagh
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A sports coach’s job is to prepare a plan, give it to the player(s), and hold them accountable to it. Change the strategy if needs be, call the shots. The job of the player(s) is then to follow those instructions.
If you have trouble keeping yourself accountable, Kavanagh argues that it can be good to separate how you approach things.
Not just “coach yourself”, but put yourself entirely in the coach’s shoes, as though you were a separate person, then switch back, and follow those instructions, trusting in your coach’s guidance.
The book also provides illustrative examples and guides the reader through some potential pitfalls—for example, what happens when morning you doesn’t want to do the things that evening you decided would be best?
The absolute backbone of this method is that it takes away the paralysing self-doubt that can occur when we second-guess ourselves mid-task.
In short, this book will fire up your enthusiasm and give you a reliable fall-back for when your motivation’s flagging.
Share This Post
-

Her Mental Health Treatment Was Helping. That’s Why Insurance Cut Off Her Coverage.
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Reporting Highlights
- Progress Denials: Insurers use a patient’s improvement to justify denying mental health coverage.
- Providers Disagree: Therapists argue with insurers and the doctors they employ to continue covering treatment for their patients.
- Patient Harm: Some patients backslid when insurers cut off coverage for treatment at key moments.
These highlights were written by the reporters and editors who worked on this story.
Geneva Moore’s therapist pulled out her spiral notebook. At the top of the page, she jotted down the date, Jan. 30, 2024, Moore’s initials and the name of the doctor from the insurance company to whom she’d be making her case.
She had only one chance to persuade him, and by extension Blue Cross and Blue Shield of Texas, to continue covering intensive outpatient care for Moore, a patient she had come to know well over the past few months.
The therapist, who spoke on the condition of anonymity out of fear of retaliation from insurers, spent the next three hours cramming, as if she were studying for a big exam. She combed through Moore’s weekly suicide and depression assessments, group therapy notes and write-ups from their past few sessions together.
She filled two pages with her notes: Moore had suicidal thoughts almost every day and a plan for how she would take her own life. Even though she expressed a desire to stop cutting her wrists, she still did as often as three times a week to feel the release of pain. She only had a small group of family and friends to offer support. And she was just beginning to deal with her grief and trauma over sexual and emotional abuse, but she had no healthy coping skills.
Less than two weeks earlier, the therapist’s supervisor had struck out with another BCBS doctor. During that call, the insurance company psychiatrist concluded Moore had shown enough improvement that she no longer needed intensive treatment. “You have made progress,” the denial letter from BCBS Texas read.
When the therapist finally got on the phone with a second insurance company doctor, she spoke as fast as she could to get across as many of her points as possible.
“The biggest concern was the abnormal thoughts — the suicidal ideation, self-harm urges — and extensive trauma history,” the therapist recalled in an interview with ProPublica. “I was really trying to emphasize that those urges were present, and they were consistent.”
She told the company doctor that if Moore could continue on her treatment plan, she would likely be able to leave the program in 10 weeks. If not, her recovery could be derailed.
The doctor wasn’t convinced. He told the therapist that he would be upholding the initial denial. Internal notes from the BCBS Texas doctors say that Moore exhibited “an absence of suicidal thoughts,” her symptoms had “stabilized” and she could “participate in a lower level of care.”
The call lasted just seven minutes.
Moore was sitting in her car during her lunch break when her therapist called to give her the news. She was shocked and had to pull herself together to resume her shift as a technician at a veterinary clinic.
“The fact that it was effective immediately,” Moore said later, “I think that was the hardest blow of it all.”
Many Americans must rely on insurers when they or family members are in need of higher-touch mental health treatment, such as intensive outpatient programs or round-the-clock care in a residential facility. The costs are high, and the stakes for patients often are, too. In 2019 alone, the U.S. spent more than $106.5 billion treating adults with mental illness, of which private insurance paid about a third. One 2024 study found that the average quoted cost for a month at a residential addiction treatment facility for adolescents was more than $26,000.
Health insurers frequently review patients’ progress to see if they can be moved down to a lower — and almost always cheaper — level of care. That can cut both ways. They sometimes cite a lack of progress as a reason to deny coverage, labeling patients’ conditions as chronic and asserting that they have reached their baseline level of functioning. And if they make progress, which would normally be celebrated, insurers have used that against patients to argue they no longer need the care being provided.
Their doctors are left to walk a tightrope trying to convince insurers that patients are making enough progress to stay in treatment as long as they actually need it, but not so much that the companies prematurely cut them off from care. And when insurers demand that providers spend their time justifying care, it takes them away from their patients.
“The issues that we grapple with are in the real world,” said Dr. Robert Trestman, the chair of psychiatry and behavioral medicine at the Virginia Tech Carilion School of Medicine and chair of the American Psychiatric Association’s Council on Healthcare Systems and Financing. “People are sicker with more complex conditions.”
Mental health care can be particularly prone to these progress-based denials. While certain tests reveal when cancer cells are no longer present and X-rays show when bones have healed, psychiatrists say they have to determine whether someone has returned to a certain level of functioning before they can end or change their treatment. That can be particularly tricky when dealing with mental illness, which can be fluid, with a patient improving slightly one day only to worsen the next.
Though there is no way to know how often coverage gets cut off mid-treatment, ProPublica has found scores of lawsuits over the past decade in which judges have sharply criticized insurance companies for citing a patient’s improvement to deny mental health coverage. In a number of those cases, federal courts ruled that the insurance companies had broken a federal law designed to provide protections for people who get health insurance through their jobs.
Reporters reviewed thousands of pages of court documents and interviewed more than 50 insiders, lawyers, patients and providers. Over and over, people said these denials can lead to real — sometimes devastating — harm. An official at an Illinois facility with intensive mental health programs said that this past year, two patients who left before their clinicians felt they were ready due to insurance denials had attempted suicide.
Dr. Eric Plakun, a Massachusetts psychiatrist with more than 40 years of experience in residential and intensive outpatient programs, and a former board member of the American Psychiatric Association, said the “proprietary standards” insurers use as a basis for denying coverage often simply stabilize patients in crisis and “shortcut real treatment.”
Plakun offered an analogy: If someone’s house is on fire, he said, putting out the fire doesn’t restore the house. “I got a hole in the roof, and the windows have been smashed in, and all the furniture is charred, and nothing’s working electrically,” he said. “How do we achieve recovery? How do we get back to living in that home?”
Unable to pay the $350-a-day out-of-pocket cost for additional intensive outpatient treatment, Moore left her program within a week of BCBS Texas’ denial. The insurer would only cover outpatient talk therapy.
During her final day at the program, records show, Moore’s suicidal thoughts and intent to carry them out had escalated from a 7 to a 10 on a 1-to-10 scale. She was barely eating or sleeping.
A few hours after the session, Moore drove herself to a hospital and was admitted to the emergency room, accelerating a downward spiral that would eventually cost the insurer tens of thousands of dollars, more than the cost of the treatment she initially requested.
How Insurers Justify Denials
Buried in the denial letters that insurance companies send patients are a variety of expressions that convey the same idea: Improvement is a reason to deny coverage.
“You are better.” “Your child has made progress.” “You have improved.”
In one instance, a doctor working for Regence Blue Cross and Blue Shield of Oregon wrote that a patient who had been diagnosed with major depression was “sufficiently stable,” even as her own doctors wrote that she “continued to display a pattern of severe impairment” and needed round-the-clock care. A judge ruled that “a preponderance of the evidence” demonstrated that the teen’s continued residential treatment was medically necessary. The insurer said it can’t comment on the case because it ended with a confidential settlement.
In another, a doctor working for UnitedHealth Group wrote in 2019 that a teenage girl with a history of major depression who had been hospitalized after trying to take her own life by overdosing “was doing better.” The insurer denied ongoing coverage at a residential treatment facility. A judge ruled that the insurer’s determination “lacked any reasoning or citations” from the girl’s medical records and found that the insurer violated federal law. United did not comment on this case but previously argued that the girl no longer had “concerning medical issues” and didn’t need treatment in a 24-hour monitored setting.
To justify denials, the insurers cite guidelines that they use to determine how well a patient is doing and, ultimately, whether to continue paying for care. Companies, including United, have said these guidelines are independent, widely accepted and evidence-based.
Insurers most often turn to two sets: MCG (formerly known as Milliman Care Guidelines), developed by a division of the multibillion-dollar media and information company Hearst, and InterQual, produced by a unit of UnitedHealth’s mental health division, Optum. Insurers have also used guidelines they have developed themselves.
MCG Health did not respond to multiple requests for comment. A spokesperson for the Optum division that works on the InterQual guidelines said that the criteria “is a collection of established scientific evidence and medical practice intended for use as a first level screening tool” and “helps to move patients safely and efficiently through the continuum of care.”
A separate spokesperson for Optum also said the company’s “priority is ensuring the people we serve receive safe and effective care for their individual needs.” A Regence spokesperson said that the company does “not make coverage decisions based on cost or length of stay,” and that its “number one priority is to ensure our members have access to the care they need when they need it.”
In interviews, several current and former insurance employees from multiple companies said that they were required to prioritize the proprietary guidelines their company used, even if their own clinical judgment pointed in the opposite direction.
“It’s very hard when you come up against all these rules that are kind of setting you up to fail the patient,” said Brittainy Lindsey, a licensed mental health counselor who worked at the Anthem subsidiary Beacon and at Humana for a total of six years before leaving the industry in 2022. In her role, Lindsey said, she would suggest approving or denying coverage, which — for the latter — required a staff doctor’s sign-off. She is now a mental health consultant for behavioral health businesses and clinicians.
A spokesperson for Elevance Health, formerly known as Anthem, said Lindsey’s “recollection is inaccurate, both in terms of the processes that were in place when she was a Beacon employee, and how we operate today.” The spokesperson said “clinical judgment by a physician — which Ms. Lindsey was not — always takes precedence over guidelines.”
In an emailed statement, a Humana spokesperson said the company’s clinician reviewers “are essential to evaluating the facts and circumstances of each case.” But, the spokesperson said, “having objective criteria is also important to provide checks and balances and consistently comply with” federal requirements.
The guidelines are a pillar of the health insurance system known as utilization management, which paves the way for coverage denials. The process involves reviewing patients’ cases against relevant criteria every handful of days or so to assess if the company will continue paying for treatment, requiring providers and patients to repeatedly defend the need for ongoing care.
Federal judges have criticized insurance company doctors for using such guidelines in cases where they were not actually relevant to the treatment being requested or for “solely” basing their decisions on them.
Wit v. United Behavioral Health, a class-action lawsuit involving a subsidiary of UnitedHealth, has become one of the most consequential mental health cases of this century. In that case, a federal judge in California concluded that a number of United’s in-house guidelines did not adhere to generally accepted standards of care. The judge found that the guidelines allowed the company to wrongly deny coverage for certain mental health and substance use services the moment patients’ immediate problems improved. He ruled that the insurer would need to change its practices. United appealed the ruling on grounds other than the court’s findings about the defects in its guidelines, and a panel of judges partially upheld the decision. The case has been sent back to the district court for further proceedings.
Largely in response to the Wit case, nine states have passed laws requiring health insurers to use guidelines that align with the leading standards of mental health care, like those developed by nonprofit professional organizations.
Cigna has said that it “has chosen not to adopt private, proprietary medical necessity criteria” like MCG. But, according to a review of lawsuits, denial letters have continued to reference MCG. One federal judge in Utah called out the company, writing that Cigna doctors “reviewed the claims under medical necessity guidelines it had disavowed.” Cigna did not respond to specific questions about this.
Timothy Stock, one of the BCBS doctors who denied Moore’s request to cover ongoing care, had cited MCG guidelines when determining she had improved enough — something judges noted he had done before. In 2016, Stock upheld a decision on appeal to deny continued coverage for a teenage girl who was in residential treatment for major depression, post-traumatic stress disorder and anxiety. Pointing to the guidelines, Stock concluded she had shown enough improvement.
The patient’s family sued the insurer, alleging it had wrongly denied coverage. Blue Cross and Blue Shield of Illinois argued that there was evidence that showed the patient had been improving. But, a federal judge found the insurer misstated its significance. The judge partially ruled in the family’s favor, zeroing in on Stock and another BCBS doctor’s use of improvement to recommend denying additional care.
“The mere incidence of some improvement does not mean treatment was no longer medically necessary,” the Illinois judge wrote.
In another case, BCBS Illinois denied coverage for a girl with a long history of mental illness just a few weeks into her stay at a residential treatment facility, noting that she was “making progressive improvements.” Stock upheld the denial after an appeal.
Less than two weeks after Stock’s decision, court records show, she cut herself on the arm and leg with a broken light bulb. The insurer defended the company’s reasoning by noting that the girl “consistently denied suicidal ideation,” but a judge wrote that medical records show the girl was “not forthcoming” with her doctors about her behaviors. The judge ruled against the insurer, writing that Stock and another BCBS doctor “unreasonably ignored the weight of the medical evidence” showing that the girl required residential treatment.
Stock declined to comment. A spokesperson for BCBS said the company’s doctors who review requests for mental health coverage are board certified psychiatrists with multiple years of practice experience. The spokesperson added that the psychiatrists review all information received “from the provider, program and members to ensure members are receiving benefits for the right care, at the right place and at the right time.”
The BCBS spokesperson did not address specific questions related to Moore or Stock. The spokesperson said that the examples ProPublica asked about “are not indicative of the experience of the vast majority of our members,” and that it is committed to providing “access to quality, cost-effective physical and behavioral health care.”
A Lifelong Struggle
A former contemporary dancer with a bright smile and infectious laugh, Moore’s love of animals is eclipsed only by her affinity for plants. She moved from Indiana to Austin, Texas, about six years ago and started as a receptionist at a clinic before working her way up to technician.
Moore’s depression has been a constant in her life. It began as a child, when, she said, she was sexually and emotionally abused. She was able to manage as she grew up, getting through high school and attending Indiana University. But, she said, she fell back into a deep sadness after she learned in 2022 that the church she found comfort in as a college student turned out to be what she and others deemed a cult. In September of last year, she began an intensive outpatient program, which included multiple group and individual therapy sessions every week.
Moore, 32, had spent much of the past eight months in treatment for severe depression, post-traumatic stress disorder and anxiety when BCBS said it would no longer pay for the program in January.
The denial had come to her without warning.
“I was starting to get to the point where I did have some hope, and I was like, maybe I can see an actual end to this,” Moore said. “And it was just cut off prematurely.”
At the Austin emergency room where she drove herself after her treatment stopped, her heart raced. She was given medication as a sedative for her anxiety. According to hospital records she provided to ProPublica, Moore’s symptoms were brought on after “insurance said they would no longer pay.”
A hospital social worker frantically tried to get her back into the intensive outpatient program.
“That’s the sad thing,” said Kandyce Walker, the program’s director of nursing and chief operating officer, who initially argued Moore’s case with BCBS Texas. “To have her go from doing a little bit better to ‘I’m going to kill myself.’ It is so frustrating, and it’s heartbreaking.”
After the denial and her brief admission to the hospital emergency department in January, Moore began slicing her wrists more frequently, sometimes twice a day. She began to down six to seven glasses of wine a night.
“I really had thought and hoped that with the amount of work I’d put in, that I at least would have had some fumes to run on,” she said.
She felt embarrassed when she realized she had nothing to show for months of treatment. The skills she’d just begun to practice seemed to disappear under the weight of her despair. She considered going into debt to cover the cost of ongoing treatment but began to think that she’d rather end her life.
“In my mind,” she said, “that was the most practical thing to do.”
Whenever the thought crossed her mind — and it usually did multiple times a day — she remembered that she had promised her therapist that she wouldn’t.
Moore’s therapist encouraged her to continue calling BCBS Texas to try to restore coverage for more intensive treatment. In late February, about five weeks after Stock’s denial, records show that the company approved a request that sent her back to the same facility and at the same level of care as before.
But by that time, her condition had deteriorated so severely that it wasn’t enough.
Eight days later, Moore was admitted to a psychiatric hospital about half an hour from Austin. Medical records paint a harrowing picture of her condition. She had a plan to overdose and the medicine to do it. The doctor wrote that she required monitoring and had “substantial ongoing suicidality.” The denial continued to torment her. She told her doctor that her condition worsened after “insurance stopped covering” her treatment.
Her few weeks stay at the psychiatric hospital cost $38,945.06. The remaining 10 weeks of treatment at the intensive outpatient program — the treatment BCBS denied — would have cost about $10,000.
Moore was discharged from the hospital in March and went back into the program Stock had initially said she no longer needed.
It marked the third time she was admitted to the intensive outpatient program.
A few months later, as Moore picked at her lunch, her oversized glasses sliding down the bridge of her nose every so often, she wrestled with another painful realization. Had the BCBS doctors not issued the denial, she probably would have completed her treatment by now.
“I was really looking forward to that,” Moore said softly. As she spoke, she played with the thick stack of bracelets hiding the scars on her wrists.
A few weeks later, that small facility closed in part because of delays and denials from insurance companies, according to staff and billing records. Moore found herself calling around to treatment facilities to see which ones would accept her insurance. She finally found one, but in October, her depression had become so severe that she needed to be stepped up to a higher level of care.
Moore was able to get a leave of absence from work to attend treatment, which she worried would affect the promotion she had been working toward. To tide her over until she could go back to work, she used up the money her mother sent for her 30th birthday.
She smiles less than she did even a few months ago. When her roommates ask her to hang out downstairs, she usually declines. She has taken some steps forward, though. She stopped drinking and cutting her wrists, allowing scar tissue to cover her wounds.
But she’s still grieving what the denial took from her.
“I believed I could get better,” she said recently, her voice shaking. “With just a little more time, I could discharge, and I could live life finally.”
Kirsten Berg contributed research.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Decoding Hormone Balancing in Ads
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Time!
This is the bit whereby each week, we respond to subscriber questions/requests/etc
Have something you’d like to ask us, or ask us to look into? Hit reply to any of our emails, or use the feedback widget at the bottom, and a Real Human™ will be glad to read it!
Q: As to specific health topics, I would love to see someone address all these Instagram ads targeted to women that claim “You only need to ‘balance your hormones’ to lose weight, get ripped, etc.” What does this mean? Which hormones are they all talking about? They all seem to be selling a workout program and/or supplements or something similar, as they are ads, after all. Is there any science behind this stuff or is it mostly hot air, as I suspect?
Thank you for asking this, as your question prompted yesterday’s main feature, What Does “Balancing Your Hormones” Even Mean?
That’s a great suggestion also about addressing ads (and goes for health-related things in general, not just hormonal stuff) and examining their claims, what they mean, how they work (if they work!), and what’s “technically true but may
be misleading* cause confusion”*We don’t want companies to sue us, of course.
Only, we’re going to need your help for this one, subscribers!
See, here at 10almonds we practice what we preach. We limit screen time, we focus on our work when working, and simply put, we don’t see as many ads as our thousands of subscribers do. Also, ads tend to be targeted to the individual, and often vary from country to country, so chances are good that we’re not seeing the same ads that you’re seeing.
So, how about we pull together as a bit of a 10almonds community project?
- Step 1: add our email address to your contacts list, if you haven’t already
- Step 2: When you see an ad you’re curious about, select “share” (there is usually an option to share ads, but if not, feel free to screenshot or such)
- Step 3: Send the ad to us by email
We’ll do the rest! Whenever we have enough ads to review, we’ll do a special on the topic.
We will categorically not be able to do this without you, so please do join in—Many thanks in advance!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Bird Flu Is Bad for Poultry and Dairy Cows. It’s Not a Dire Threat for Most of Us — Yet.
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Headlines are flying after the Department of Agriculture confirmed that the H5N1 bird flu virus has infected dairy cows around the country. Tests have detected the virus among cattle in nine states, mainly in Texas and New Mexico, and most recently in Colorado, said Nirav Shah, principal deputy director at the Centers for Disease Control and Prevention, at a May 1 event held by the Council on Foreign Relations.
A menagerie of other animals have been infected by H5N1, and at least one person in Texas. But what scientists fear most is if the virus were to spread efficiently from person to person. That hasn’t happened and might not. Shah said the CDC considers the H5N1 outbreak “a low risk to the general public at this time.”
Viruses evolve and outbreaks can shift quickly. “As with any major outbreak, this is moving at the speed of a bullet train,” Shah said. “What we’ll be talking about is a snapshot of that fast-moving train.” What he means is that what’s known about the H5N1 bird flu today will undoubtedly change.
With that in mind, KFF Health News explains what you need to know now.
Q: Who gets the bird flu?
Mainly birds. Over the past few years, however, the H5N1 bird flu virus has increasingly jumped from birds into mammals around the world. The growing list of more than 50 species includes seals, goats, skunks, cats, and wild bush dogs at a zoo in the United Kingdom. At least 24,000 sea lions died in outbreaks of H5N1 bird flu in South America last year.
What makes the current outbreak in cattle unusual is that it’s spreading rapidly from cow to cow, whereas the other cases — except for the sea lion infections — appear limited. Researchers know this because genetic sequences of the H5N1 viruses drawn from cattle this year were nearly identical to one another.
The cattle outbreak is also concerning because the country has been caught off guard. Researchers examining the virus’s genomes suggest it originally spilled over from birds into cows late last year in Texas, and has since spread among many more cows than have been tested. “Our analyses show this has been circulating in cows for four months or so, under our noses,” said Michael Worobey, an evolutionary biologist at the University of Arizona in Tucson.
Q: Is this the start of the next pandemic?
Not yet. But it’s a thought worth considering because a bird flu pandemic would be a nightmare. More than half of people infected by older strains of H5N1 bird flu viruses from 2003 to 2016 died. Even if death rates turn out to be less severe for the H5N1 strain currently circulating in cattle, repercussions could involve loads of sick people and hospitals too overwhelmed to handle other medical emergencies.
Although at least one person has been infected with H5N1 this year, the virus can’t lead to a pandemic in its current state. To achieve that horrible status, a pathogen needs to sicken many people on multiple continents. And to do that, the H5N1 virus would need to infect a ton of people. That won’t happen through occasional spillovers of the virus from farm animals into people. Rather, the virus must acquire mutations for it to spread from person to person, like the seasonal flu, as a respiratory infection transmitted largely through the air as people cough, sneeze, and breathe. As we learned in the depths of covid-19, airborne viruses are hard to stop.
That hasn’t happened yet. However, H5N1 viruses now have plenty of chances to evolve as they replicate within thousands of cows. Like all viruses, they mutate as they replicate, and mutations that improve the virus’s survival are passed to the next generation. And because cows are mammals, the viruses could be getting better at thriving within cells that are closer to ours than birds’.
The evolution of a pandemic-ready bird flu virus could be aided by a sort of superpower possessed by many viruses. Namely, they sometimes swap their genes with other strains in a process called reassortment. In a study published in 2009, Worobey and other researchers traced the origin of the H1N1 “swine flu” pandemic to events in which different viruses causing the swine flu, bird flu, and human flu mixed and matched their genes within pigs that they were simultaneously infecting. Pigs need not be involved this time around, Worobey warned.
Q: Will a pandemic start if a person drinks virus-contaminated milk?
Not yet. Cow’s milk, as well as powdered milk and infant formula, sold in stores is considered safe because the law requires all milk sold commercially to be pasteurized. That process of heating milk at high temperatures kills bacteria, viruses, and other teeny organisms. Tests have identified fragments of H5N1 viruses in milk from grocery stores but confirm that the virus bits are dead and, therefore, harmless.
Unpasteurized “raw” milk, however, has been shown to contain living H5N1 viruses, which is why the FDA and other health authorities strongly advise people not to drink it. Doing so could cause a person to become seriously ill or worse. But even then, a pandemic is unlikely to be sparked because the virus — in its current form — does not spread efficiently from person to person, as the seasonal flu does.
Q: What should be done?
A lot! Because of a lack of surveillance, the U.S. Department of Agriculture and other agencies have allowed the H5N1 bird flu to spread under the radar in cattle. To get a handle on the situation, the USDA recently ordered all lactating dairy cattle to be tested before farmers move them to other states, and the outcomes of the tests to be reported.
But just as restricting covid tests to international travelers in early 2020 allowed the coronavirus to spread undetected, testing only cows that move across state lines would miss plenty of cases.
Such limited testing won’t reveal how the virus is spreading among cattle — information desperately needed so farmers can stop it. A leading hypothesis is that viruses are being transferred from one cow to the next through the machines used to milk them.
To boost testing, Fred Gingrich, executive director of a nonprofit organization for farm veterinarians, the American Association of Bovine Practitioners, said the government should offer funds to cattle farmers who report cases so that they have an incentive to test. Barring that, he said, reporting just adds reputational damage atop financial loss.
“These outbreaks have a significant economic impact,” Gingrich said. “Farmers lose about 20% of their milk production in an outbreak because animals quit eating, produce less milk, and some of that milk is abnormal and then can’t be sold.”
The government has made the H5N1 tests free for farmers, Gingrich added, but they haven’t budgeted money for veterinarians who must sample the cows, transport samples, and file paperwork. “Tests are the least expensive part,” he said.
If testing on farms remains elusive, evolutionary virologists can still learn a lot by analyzing genomic sequences from H5N1 viruses sampled from cattle. The differences between sequences tell a story about where and when the current outbreak began, the path it travels, and whether the viruses are acquiring mutations that pose a threat to people. Yet this vital research has been hampered by the USDA’s slow and incomplete posting of genetic data, Worobey said.
The government should also help poultry farmers prevent H5N1 outbreaks since those kill many birds and pose a constant threat of spillover, said Maurice Pitesky, an avian disease specialist at the University of California-Davis.
Waterfowl like ducks and geese are the usual sources of outbreaks on poultry farms, and researchers can detect their proximity using remote sensing and other technologies. By zeroing in on zones of potential spillover, farmers can target their attention. That can mean routine surveillance to detect early signs of infections in poultry, using water cannons to shoo away migrating flocks, relocating farm animals, or temporarily ushering them into barns. “We should be spending on prevention,” Pitesky said.
Q: OK it’s not a pandemic, but what could happen to people who get this year’s H5N1 bird flu?
No one really knows. Only one person in Texas has been diagnosed with the disease this year, in April. This person worked closely with dairy cows, and had a mild case with an eye infection. The CDC found out about them because of its surveillance process. Clinics are supposed to alert state health departments when they diagnose farmworkers with the flu, using tests that detect influenza viruses, broadly. State health departments then confirm the test, and if it’s positive, they send a person’s sample to a CDC laboratory, where it is checked for the H5N1 virus, specifically. “Thus far we have received 23,” Shah said. “All but one of those was negative.”
State health department officials are also monitoring around 150 people, he said, who have spent time around cattle. They’re checking in with these farmworkers via phone calls, text messages, or in-person visits to see if they develop symptoms. And if that happens, they’ll be tested.
Another way to assess farmworkers would be to check their blood for antibodies against the H5N1 bird flu virus; a positive result would indicate they might have been unknowingly infected. But Shah said health officials are not yet doing this work.
“The fact that we’re four months in and haven’t done this isn’t a good sign,” Worobey said. “I’m not super worried about a pandemic at the moment, but we should start acting like we don’t want it to happen.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: