Women spend more of their money on health care than men. And no, it’s not just about ‘women’s issues’
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Medicare, Australia’s universal health insurance scheme, guarantees all Australians access to a wide range of health and hospital services at low or no cost.
Although access to the scheme is universal across Australia (regardless of geographic location or socioeconomic status), one analysis suggests women often spend more out-of-pocket on health services than men.
Other research has found men and women spend similar amounts on health care overall, or even that men spend a little more. However, it’s clear women spend a greater proportion of their overall expenditure on health care than men. They’re also more likely to skip or delay medical care due to the cost.
So why do women often spend more of their money on health care, and how can we address this gap?

Women have more chronic diseases, and access more services
Women are more likely to have a chronic health condition compared to men. They’re also more likely to report having multiple chronic conditions.
While men generally die earlier, women are more likely to spend more of their life living with disease. There are also some conditions which affect women more than men, such as autoimmune conditions (for example, multiple sclerosis and rheumatoid arthritis).
Further, medical treatments can sometimes be less effective for women due to a focus on men in medical research.
These disparities are likely significant in understanding why women access health services more than men.
For example, 88% of women saw a GP in 2021–22 compared to 79% of men.
As the number of GPs offering bulk billing continues to decline, women are likely to need to pay more out-of-pocket, because they see a GP more often.
In 2020–21, 4.3% of women said they had delayed seeing a GP due to cost at least once in the previous 12 months, compared to 2.7% of men.
Data from the Australian Bureau of Statistics has also shown women are more likely to delay or avoid seeing a mental health professional due to cost.

Women are also more likely to need prescription medications, owing at least partly to their increased rates of chronic conditions. This adds further out-of-pocket costs. In 2020–21, 62% of women received a prescription, compared to 37% of men.
In the same period, 6.1% of women delayed getting, or did not get prescribed medication because of the cost, compared to 4.9% of men.
Reproductive health conditions
While women are disproportionately affected by chronic health conditions throughout their lifespan, much of the disparity in health-care needs is concentrated between the first period and menopause.
Almost half of women aged over 18 report having experienced chronic pelvic pain in the previous five years. This can be caused by conditions such as endometriosis, dysmenorrhoea (period pain), vulvodynia (vulva pain), and bladder pain.
One in seven women will have a diagnosis of endometriosis by age 49.
Meanwhile, a quarter of all women aged 45–64 report symptoms related to menopause that are significant enough to disrupt their daily life.
All of these conditions can significantly reduce quality of life and increase the need to seek health care, sometimes including surgical treatment.
Of course, conditions like endometriosis don’t just affect women. They also impact trans men, intersex people, and those who are gender diverse.
Diagnosis can be costly
Women often have to wait longer to get a diagnosis for chronic conditions. One preprint study found women wait an average of 134 days (around 4.5 months) longer than men for a diagnosis of a long-term chronic disease.
Delays in diagnosis often result in needing to see more doctors, again increasing the costs.
Despite affecting about as many people as diabetes, it takes an average of between six-and-a-half to eight years to diagnose endometriosis in Australia. This can be attributed to a number of factors including society’s normalisation of women’s pain, poor knowledge about endometriosis among some health professionals, and the lack of affordable, non-invasive methods to accurately diagnose the condition.
There have been recent improvements, with the introduction of Medicare rebates for longer GP consultations of up to 60 minutes. While this is not only for women, this extra time will be valuable in diagnosing and managing complex conditions.
But gender inequality issues still exist in the Medicare Benefits Schedule. For example, both pelvic and breast ultrasound rebates are less than a scan for the scrotum, and no rebate exists for the MRI investigation of a woman’s pelvic pain.
Management can be expensive too
Many chronic conditions, such as endometriosis, which has a wide range of symptoms but no cure, can be very hard to manage. People with endometriosis often use allied health and complementary medicine to help with symptoms.
On average, women are more likely than men to use both complementary therapies and allied health.
While women with chronic conditions can access a chronic disease management plan, which provides Medicare-subsidised visits to a range of allied health services (for example, physiotherapist, psychologist, dietitian), this plan only subsidises five sessions per calendar year. And the reimbursement is usually around 50% or less, so there are still significant out-of-pocket costs.
In the case of chronic pelvic pain, the cost of accessing allied or complementary health services has been found to average A$480.32 across a two-month period (across both those who have a chronic disease management plan and those who don’t).
More spending, less saving
Womens’ health-care needs can also perpetuate financial strain beyond direct health-care costs. For example, women with endometriosis and chronic pelvic pain are often caught in a cycle of needing time off from work to attend medical appointments.
Our preliminary research has shown these repeated requests, combined with the common dismissal of symptoms associated with pelvic pain, means women sometimes face discrimination at work. This can lead to lack of career progression, underemployment, and premature retirement.

Similarly, with 160,000 women entering menopause each year in Australia (and this number expected to increase with population growth), the financial impacts are substantial.
As many as one in four women may either shift to part-time work, take time out of the workforce, or retire early due to menopause, therefore earning less and paying less into their super.
How can we close this gap?
Even though women are more prone to chronic conditions, until relatively recently, much of medical research has been done on men. We’re only now beginning to realise important differences in how men and women experience certain conditions (such as chronic pain).
Investing in women’s health research will be important to improve treatments so women are less burdened by chronic conditions.
In the 2024–25 federal budget, the government committed $160 million towards a women’s health package to tackle gender bias in the health system (including cost disparities), upskill medical professionals, and improve sexual and reproductive care.
While this reform is welcome, continued, long-term investment into women’s health is crucial.
Mike Armour, Associate Professor at NICM Health Research Institute, Western Sydney University; Amelia Mardon, Postdoctoral Research Fellow in Reproductive Health, Western Sydney University; Danielle Howe, PhD Candidate, NICM Health Research Institute, Western Sydney University; Hannah Adler, PhD Candidate, Health Communication and Health Sociology, Griffith University, and Michelle O’Shea, Senior Lecturer, School of Business, Western Sydney University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Does PRP Work For Hair Loss?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Ankit Gupta takes us through the details of this hair loss remedy for androgenic alopecia.
The bald truth
Platelet-Rich Plasma (PRP) is a controversial treatment for androgenic hair loss.
What it involves: blood is drawn and separated using a centrifuge. PRP—including growth proteins and hormones—is extracted from the blood; about 30 ml of blood is needed to produce 5 ml of PRP. This is then injected directly into the scalp. As this can be painful, local anaesthetic is sometimes used first. This usually involves monthly sessions for the first 3 months, then booster sessions every 3–6 months thereafter.
Does it work? Research is young; so far 60% of trials have found it worked; 40% found it didn’t. When it works, effectiveness (in terms of hair restoration) is considered to be between 25–43%. Results are inconsistent and seem to vary from person to person.
In short, this doctor’s recommendation is to consider it after already having tried standard treatments such as finasteride and/or minoxidil, as they are more likely to work and don’t involve such exciting procedures as injecting your own blood extracts back into your head.
For more on all of this, plus links to the 13 papers cited, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- Hair-Loss Remedies, By Science
- Hair Growth: Caffeine and Minoxidil Strategies
- Gentler Hair Health Options
Take care!
Share This Post
-
Ketogenic Diet: Burning Fat Or Burning Out?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.

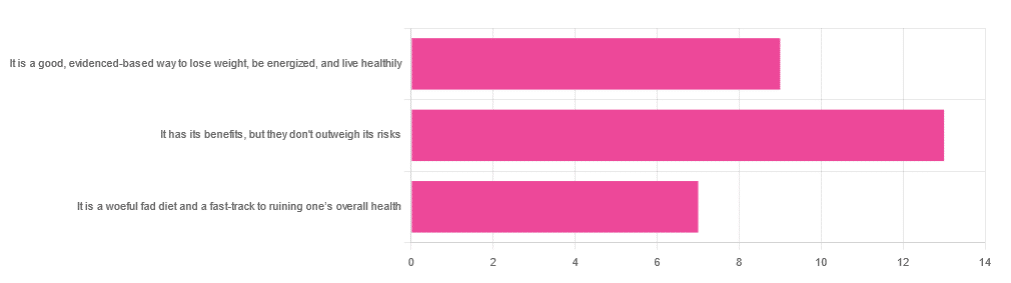
In Wednesday’s newsletter, we asked you for your opinion of the keto diet, and got the above-depicted, below-described set of responses:
- About 45% said “It has its benefits, but they don’t outweigh the risks”
- About 31% said “It is a good, evidence-based way to lose weight, be energized, and live healthily”
- About 24% said “It is a woeful fad diet and a fast-track to ruining one’s overall health”
So what does the science say?
First, what is the ketogenic diet?
There are two different stories here:
- Per science, it’s a medical diet designed to help treat refractory epilepsy in children.
- Per popular lore, it’s an energizing weight loss diet for Instagrammers and YouTubers.
Can it be both? The answer is: yes, but with some serious caveats, which we’ll cover over the course of today’s feature.
The ketogenic diet works by forcing the body to burn fat for energy: True or False?
True! This is why it helps for children with refractory epilepsy. By starving the body (including the brain) of glucose, the liver must convert fat into fatty acids and ketones, which latter the brain (and indeed the rest of the body) can now use for energy instead of glucose, thus avoiding one of the the main triggers of refractory epilepsy in children.
See: The Ketogenic Diet: One Decade Later | Pediatrics
Even the pediatric epilepsy studies, however, conclude it does have unwanted side effects, such as kidney stones, constipation, high cholesterol, and acidosis:
Source: Dietary Therapies for Epilepsy
The ketogenic diet is good for weight loss: True or False?
True! Insofar as it does cause weight loss, often rapidly. Of course, so do diarrhea and vomiting, but these are not usually held to be healthy methods of weight loss. As for keto, a team of researchers recently concluded:
❝As obesity rates in the populace keep rising, dietary fads such as the ketogenic diet are gaining traction.
Although they could help with weight loss, this study had a notable observation of severe hypercholesterolemia and increased risk of atherosclerotic cardiovascular disease among the ketogenic diet participants.❞
~ Dr. Shadan Khdher et al.
On which note…
The ketogenic diet is bad for the heart: True or False?
True! As Dr. Joanna Popiolek-Kalisz concluded recently:
❝In terms of cardiovascular mortality, the low-carb pattern is more beneficial than very low-carbohydrate (including the ketogenic diet). There is still scarce evidence comparing ketogenic to the Mediterranean diet.
Other safety concerns in cardiovascular patients such as adverse events related to ketosis, fat-free mass loss, or potential pharmacological interactions should be also taken into consideration in future research.❞
~ Dr. Joanna Popiolek-Kalisz
Read in full: Ketogenic diet and cardiovascular risk: state of the art review
The ketogenic diet is good for short-term weight loss, but not long-term maintenance: True or False?
True! Again, insofar as it works in the short term. It’s not the healthiest way to lose weight and we don’t recommend it, but it did does indeed precipitate short-term weight loss. Those benefits are not typically observed for longer than a short time, though, as the above-linked paper mentions:
❝The ketogenic diet does not fulfill the criteria of a healthy diet. It presents the potential for rapid short-term reduction of body mass, triglycerides level, Hb1Ac, and blood pressure.
Its efficacy for weight loss and the above-mentioned metabolic changes is not significant in long-term observations.❞
~ Ibid.
The ketogenic diet is a good, evidence-based way to lose weight, be energized, and live healthily: True or False?
False, simply, as you may have gathered from the above, but we’ve barely scratched the surface in terms of the risks.
That said, as mentioned, it will induce short-term weight loss, and as for being energized, typically there is a slump-spike-slump in energy:
- At first, the body is running out of glucose, and so naturally feels weak and tired.
- Next, the body enters ketosis, and so feels energized and enlivened ← this is the part where the popular enthusiastic reviews come from
- Then, the body starts experiencing all the longer-term problems associated with lacking carbohydrates and having an overabundance of fat, so becomes gradually more sick and tired.
Because of this, the signs of symptoms of being in ketosis (aside from: measurably increased ketones in blood, breath, and urine) are listed as:
- Bad breath
- Weight loss
- Appetite loss
- Increased focus and energy
- Increased fatigue and irritability
- Digestive issues
- Insomnia
The slump-spike-slump we mentioned is the reason for the seemingly contradictory symptoms of increased energy and increased fatigue—you get one and then the other.
Here’s a small but illustrative study, made clearer by its participants being a demographic whose energy levels are most strongly affected by dietary factors:
The ketogenic diet is a woeful fad diet and a fast-track to ruining one’s overall health: True or False?
True, subjectively in the first part, as it’s a little harsher than we usually go for in tone, though it has been called a fad diet in scientific literature. The latter part (ruining one’s overall health) is observably true.
One major problem is incidental-but-serious, which is that a low-carb diet is typically a de facto low-fiber diet, which is naturally bad for the gut and heart.
Other things are more specific to the keto diet, such as the problems with the kidneys:
However, kidney stones aren’t the worst of the problems:
Is Losing Weight Worth Losing Your Kidney: Keto Diet Resulting in Renal Failure
We’re running out of space and the risks associated with the keto diet are many, but for example even in the short term, it already increases osteoporosis risk:
❝Markers of bone modeling/remodeling were impaired after short-term low-carbohydrate high-fat diet, and only one marker of resorption recovered after acute carbohydrate restoration❞
~ Dr. Ida Heikura et al.
A Short-Term Ketogenic Diet Impairs Markers of Bone Health in Response to Exercise
Want a healthier diet?
We recommend the Mediterranean diet.
See also: Four Ways To Upgrade The Mediterranean
(the above is about keeping to the Mediterranean diet, while tweaking one’s choices within it for a specific extra health focus such as an anti-inflammatory upgrade, a heart-healthy upgrade, a gut-healthy upgrade, and a brain-healthy upgrade)
Enjoy!
Share This Post
-

Are Electrolyte Supplements Worth It?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When To Take Electrolytes (And When We Shouldn’t!)
Any sports nutrition outlet will sell electrolyte supplements. Sometimes in the form of sports drinks that claim to be more hydrating than water, or tablets that can be dissolved in water to make the same. How do they work, and should we be drinking them?
What are electrolytes?
They’re called “electrolytes” because they are ionized particles (so, they have a positive or negative electrical charge, depending on which kind of ion they are) that are usually combined in the form of salts.
The “first halves” of the salts include:
- Sodium
- Potassium
- Calcium
- Magnesium
The “second halves” of the salts include:
- Chloride
- Phosphate
- Bicarbonate
- Nitrate
It doesn’t matter too much which way they’re combined, provided we get what we need. Specifically, the body needs them in a careful balance. Too much or too little, and bad things will start happening to us.
If we live in a temperate climate with a moderate lifestyle and a balanced diet, and have healthy working kidneys, usually our kidneys will keep them all in balance.
Why might we need to supplement?
Firstly, of course, you might have a dietary deficiency. Magnesium deficiency in particular is very common in North America, as people simply do not eat as much greenery as they ideally would.
But, also, you might sweat out your electrolytes, in which case, you will need to replace them.
In particular, endurance training and High Intensity Interval Training are likely to prompt this.
However… Are you in a rush? Because if not, you might just want to recover more slowly:
❝Vigorous exercise and warm/hot temperatures induce sweat production, which loses both water and electrolytes. Both water and sodium need to be replaced to re-establish “normal” total body water (euhydration).
This replacement can be by normal eating and drinking practices if there is no urgency for recovery.
But if rapid recovery (<24 h) is desired or severe hypohydration (>5% body mass) is encountered, aggressive drinking of fluids and consuming electrolytes should be encouraged to facilitate recovery❞
Source: Fluid and electrolyte needs for training, competition, and recovery
Should we just supplement anyway, as a “catch-all” to be sure?
Probably not. In particular, it is easy to get too much sodium in one’s diet, let alone by supplementation.And, oversupplementation of calcium is very common, and causes its own health problems. See:
To look directly to the science on this one, we see a general consensus amongst research reviews: “this is complicated and can go either way depending on what else people are doing”:
- Trace minerals intake: risks and benefits for cardiovascular health
- Electrolyte minerals intake and cardiovascular health
Well, that’s not helpful. Any clearer pointers?
Yes! Researchers Latzka and Mountain put together a very practical list of tips. Rather, they didn’t put it as a list, but the following bullet points are information extracted directly from their abstract, though we’ve also linked the full article below:
- It is recommended that individuals begin exercise when adequately hydrated.
- This can be facilitated by drinking 400 mL to 600 mL of fluid 2 hours before beginning exercise and drinking sufficient fluid during exercise to prevent dehydration from exceeding 2% body weight.
- A practical recommendation is to drink small amounts of fluid (150-300 mL) every 15 to 20 minutes of exercise, varying the volume depending on sweating rate.
- During exercise lasting less than 90 minutes, water alone is sufficient for fluid replacement
- During prolonged exercise lasting longer than 90 minutes, commercially available carbohydrate electrolyte beverages should be considered to provide an exogenous carbohydrate source to sustain carbohydrate oxidation and endurance performance.
- Electrolyte supplementation is generally not necessary because dietary intake is adequate to offset electrolytes lost in sweat and urine; however, during initial days of hot-weather training or when meals are not calorically adequate, supplemental salt intake may be indicated to sustain sodium balance.
Source: Water and electrolyte requirements for exercise
Bonus tip:
We’ve talked before about the specific age-related benefits of creatine supplementation, but if you’re doing endurance training or HIIT, you might also want to consider a creatine-electrolyte combination sports drink (even if you make it yourself):
Where can I get electrolyte supplements?
They’re easy to find in any sports nutrition store, or you can buy them online; here’s an example product on Amazon for your convenience
You can also opt for natural and/or homemade electrolyte drinks:
Healthline | 8 Healthy Drinks Rich in Electrolytes
Enjoy!
Share This Post

-
Treadmill vs Road
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small 😎
❝Why do I get tired much more quickly running outside, than I do on the treadmill? Every time I get worn out quickly but at home I can go for much longer!❞
Short answer: the reason is Newton’s laws of motion.
In other words: on a treadmill, you need only maintain your position in space relative the the Earth while the treadmill moves beneath you, whereas on the road, you need to push against the Earth with sufficient force to move it relative to your body.
Illustrative thought experiment to make that clearer: if you were to stand on a treadmill with roller skates, and hold onto the bar with even just one finger, you would maintain your speed as far as the treadmill’s computer is concerned—whereas to maintain your speed on a flat road, you’d still need to push with your back foot every few yards or so.
More interesting answer: it’s a qualitatively different exercise (i.e. not just quantitively different). This is because of all that pushing you’re having to do on the road, while on a treadmill, the only pushing you have to do is just enough to counteract gravity (i.e. to keep you upright).
As such, both forms of running are a cardio exercise (because simply moving your legs quickly, even without having to apply much force, is still something that requires oxygenated blood feeding the muscles), but road-running adds an extra element of resistance exercise for the muscles of your lower body. Thus, road-running will enable you to build-maintain muscle much more than treadmill-running will.
Some extra things to bear in mind, however:
1) You can increase the resistance work for either form of running, by adding weight (such as by wearing a weight vest):
Weight Vests Against Osteoporosis: Do They Really Build Bone?
…and while road-running will still be the superior form of resistance work (for the reasons we outlined above), adding a weight vest will still be improving your stabilization muscles, just as it would if you were standing still while holding the weight up.
2) Stationary cycling does not have the same physics differences as stationary running. By this we mean: an exercise bike will require your muscles to do just as much pushing as they would on a road. This makes stationary cycling an excellent choice for high intensity resistance training (HIRT):
3) The best form of exercise is the one that you will actually do. Thus, when it’s raining sidewise outside, a treadmill inside will get exercise done better than no running at all. Similarly, a treadmill exercise session takes a lot less preparation (“switch it on”) than a running session outside (“get dressed appropriately for the weather, apply sunscreen if necessary, remember to bring water, etc etc”), and thus is also much more likely to actually occur. The ability to stop whenever one wants is also a reassuring factor that makes one much more likely to start. See for example:
How To Do HIIT (Without Wrecking Your Body)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Cancer Journey – by Dr. Chadi Nabhan
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
After a brief introduction of what cancer actually is and what causes it, the layout of the rest of the book is in chronological order of patient experience, that is to say, what to expect during the journey from screening and diagnosis, to one’s first oncology visit (the author being an oncologist himself), how cancer staging works, getting second opinions, and a chapter-by-chapter review of many different treatment options, ranging from surgery and chemotherapy, to radiation and hormonal therapies, and even more modern targeted therapies, immunotherapy, cellular therapies, and yes, complementary and alternative therapies, amongst others we haven’t listed for the sake of brevity.
He doesn’t leave it there though; he also talks managing side effects, monitoring for recurrence, and even caring for the caregiver(s), along with eventual survivorship and that emotional journey, or if it comes down to it, palliative and hospice care.
Finishing on a hopeful note, he also brings attention to novel approaches that are being trialled presently, and the prospects for the near future of cancer care.
The style is very human and readable, notwithstanding that the author has hundreds of peer-reviewed publications to his name, the content here is presented in a much more approachable, less clinical way, while still conveying all the information that needs to be conveyed.
Bottom line: if you or a loved one is facing cancer, this book will be an invaluable resource.
Click here to check out The Cancer Journey, and understand each part of it!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Viruses aren’t always harmful. 6 ways they’re used in health care and pest control
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We tend to just think of viruses in terms of their damaging impacts on human health and lives. The 1918 flu pandemic killed around 50 million people. Smallpox claimed 30% of those who caught it, and survivors were often scarred and blinded. More recently, we’re all too familiar with the health and economic impacts of COVID.
But viruses can also be used to benefit human health, agriculture and the environment.
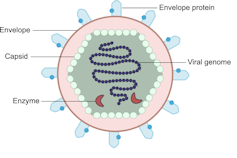
Viruses are comparatively simple in structure, consisting of a piece of genetic material (RNA or DNA) enclosed in a protein coat (the capsid). Some also have an outer envelope.
Viruses get into your cells and use your cell machinery to copy themselves.
Here are six ways we’ve harnessed this for health care and pest control.1. To correct genes
Viruses are used in some gene therapies to correct malfunctioning genes. Genes are DNA sequences that code for a particular protein required for cell function.
If we remove viral genetic material from the capsid (protein coat) we can use the space to transport a “cargo” into cells. These modified viruses are called “viral vectors”.

Viruses consist of a piece of RNA or DNA enclosed in a protein coat called the capsid.
DEXiViral vectors can deliver a functional gene into someone with a genetic disorder whose own gene is not working properly.
Some genetic diseases treated this way include haemophilia, sickle cell disease and beta thalassaemia.
2. Treat cancer
Viral vectors can be used to treat cancer.
Healthy people have p53, a tumour-suppressor gene. About half of cancers are associated with the loss of p53.
Replacing the damaged p53 gene using a viral vector stops the cancerous cell from replicating and tells it to suicide (apoptosis).
Viral vectors can also be used to deliver an inactive drug to a tumour, where it is then activated to kill the tumour cell.
This targeted therapy reduces the side effects otherwise seen with cytotoxic (cell-killing) drugs.
We can also use oncolytic (cancer cell-destroying) viruses to treat some types of cancer.
Tumour cells have often lost their antiviral defences. In the case of melanoma, a modified herpes simplex virus can kill rapidly dividing melanoma cells while largely leaving non-tumour cells alone.
3. Create immune responses
Viral vectors can create a protective immune response to a particular viral antigen.
One COVID vaccine uses a modified chimp adenovirus (adenoviruses cause the common cold in humans) to transport RNA coding for the SARS-CoV-2 spike protein into human cells.
The RNA is then used to make spike protein copies, which stimulate our immune cells to replicate and “remember” the spike protein.
Then, when you are exposed to SARS-CoV-2 for real, your immune system can churn out lots of antibodies and virus-killing cells very quickly to prevent or reduce the severity of infection.
4. Act as vaccines
Viruses can be modified to act directly as vaccines themselves in several ways.
We can weaken a virus (for an attenuated virus vaccine) so it doesn’t cause infection in a healthy host but can still replicate to stimulate the immune response. The chickenpox vaccine works like this.
The Salk vaccine for polio uses a whole virus that has been inactivated (so it can’t cause disease).
Others use a small part of the virus such as a capsid protein to stimulate an immune response (subunit vaccines).
An mRNA vaccine packages up viral RNA for a specific protein that will stimulate an immune response.
5. Kill bacteria
Viruses can – in limited situations in Australia – be used to treat antibiotic-resistant bacterial infections.
Bacteriophages are viruses that kill bacteria. Each type of phage usually infects a particular species of bacteria.
Unlike antibiotics – which often kill “good” bacteria along with the disease-causing ones – phage therapy leaves your normal flora (useful microbes) intact.
Bacteriophages (red) are viruses that kill bacteria (green).
Shutterstock6. Target plant, fungal or animal pests
Viruses can be species-specific (infecting one species only) and even cell-specific (infecting one type of cell only).
This occurs because the proteins viruses use to attach to cells have a shape that binds to a specific type of cell receptor or molecule, like a specific key fits a lock.
The virus can enter the cells of all species with this receptor/molecule. For example, rabies virus can infect all mammals because we share the right receptor, and mammals have other characteristics that allow infection to occur whereas other non-mammal species don’t.
When the receptor is only found on one cell type, then the virus will infect that cell type, which may only be found in one or a limited number of species. Hepatitis B virus successfully infects liver cells primarily in humans and chimps.
We can use that property of specificity to target invasive plant species (reducing the need for chemical herbicides) and pest insects (reducing the need for chemical insecticides). Baculoviruses, for example, are used to control caterpillars.
Similarly, bacteriophages can be used to control bacterial tomato and grapevine diseases.
Other viruses reduce plant damage from fungal pests.
Myxoma virus and calicivirus reduce rabbit populations and their environmental impacts and improve agricultural production.
Just like humans can be protected against by vaccination, plants can be “immunised” against a disease-causing virus by being exposed to a milder version.

Thea van de Mortel, Professor, Nursing, School of Nursing and Midwifery, Griffith University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: