Apples vs Bananas – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing apples to bananas, we picked the bananas.
Why?
Both apples and bananas contain lots of vitamins, but bananas contain far more of Vitamins A, B, and C.
Apples beat bananas only for vitamins E and K.
This may seem like “well that’s 2 vs 3; that’s pretty close” until one remembers that vitamin B is actually eight vitamins in a trenchcoat. Bananas have more of vitamins B1, B2, B3, B5, B6, and B9.
If you’re wondering about the other numbers: neither fruit contains vitamins B7 (biotin) or B12 (cobalamins of various kinds). Vitamins B4, B8, B10, and B11 do not exist as such (due to changes in how vitamins are classified).
Both apples and bananas contain lots of minerals, but bananas contain far more of iron, magnesium, phosphorus, potassium, zinc, copper, manganese, and selenium.
Apples beat bananas only for calcium (and then, only very marginally)
Both apples and bananas have plenty of fiber.
Apples have marginally less sugar, but given the fiber content, this is pretty much moot when it comes to health considerations, and apples are higher in fructose in any case.
In short, both are wonderful fruits (and we encourage you to enjoy both!), and/but bananas beat apples healthwise in almost all measures.
PS: top tip if you find it challenging to get bananas at the right level of ripeness for eating… Try sun-dried! Not those hard chip kinds (those are mechanically and/or chemically dried, and usually have added sugar and preservatives), but sun-dried.
Here’s an example product on Amazon
Warning: since there aren’t many sun-dried bananas available on Amazon, double-check you haven’t been redirected to mechanically/chemically dried ones, as Amazon will try that sometimes!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How often should you wash your sheets and towels?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Everyone seems to have a different opinion when it comes to how often towels and bed sheets should be washed. While many people might wonder whether days or weeks is best, in one survey from the United Kingdom, almost half of single men reported not washing their sheets for up to four months at a time.
It’s fairly clear that four months is too long to leave it, but what is the ideal frequency?
Bed linen and towels are quite different and so should be washed at different intervals. While every week or two will generally suffice for sheets, towels are best washed every few days.
Anyway, who doesn’t love the feeling of a fresh set of sheets or the smell of a newly laundered towel?
Why you should wash towels more often
When you dry yourself, you deposit thousands of skin cells and millions of microbes onto the towel. And because you use your towel to dry yourself after a shower or bath, your towel is regularly damp.
You also deposit a hefty amount of dead skin, microbes, sweat and oils onto your sheets every night. But unless you’re a prolific night sweater, your bedding doesn’t get wet after a night’s sleep.
Towels are also made of a thicker material than sheets and therefore tend to stay damp for longer.
So what is it about the dampness that causes a problem? Wet towels are a breeding ground for bacteria and moulds. Moulds especially love damp environments. Although mould won’t necessarily be visible (you would need significant growth to be able to see it) this can lead to an unpleasant smell.
As well as odours, exposure to these microbes in your towels and sheets can cause asthma, allergic skin irritations, or other skin infections.

People don’t always agree on how often to change the sheets.
http://rawpixel.com/ShutterstockSo what’s the ideal frequency?
For bedding, it really depends on factors such as whether you have a bath or shower just before going to bed, or if you fall into bed after a long, sweaty day and have your shower in the morning. You will need to wash your sheets more regularly in the latter case. As a rule of thumb, once a week or every two weeks should be fine.
Towels should ideally be washed more regularly – perhaps every few days – while your facecloth should be cleaned after every use. Because it gets completely wet, it will be wet for a longer time, and retain more skin cells and microbes.
Wash your towels at a high temperature (for example, 65°C) as that will kill many microbes. If you are conscious of saving energy, you can use a lower temperature and add a cup of vinegar to the wash. The vinegar will kill microbes and prevent bad smells from developing.
Clean your washing machine regularly and dry the fold in the rubber after every wash, as this is another place microbes like to grow.
Smelly towels
What if you regularly wash your towels, but they still smell bad? One of the reasons for this pong could be that you’ve left them in the washing machine too long after the wash. Especially if it was a warm wash cycle, the time they’re warm and damp will allow microbes to happily grow. Under lab conditions the number of these bacteria can double every 30 minutes.
It’s important to hang your towel out to dry after use and not to leave towels in the washing machine after the cycle has finished. If possible, hang your towels and bedding out in the sun. That will dry them quickly and thoroughly and will foster that lovely fresh, clean cotton smell. Using a dryer is a good alternative if the weather is bad, but outdoors in the sun is always better if possible.
Also, even if your towel is going to be washed, don’t throw a wet towel into the laundry basket, as the damp, dirty towel will be an ideal place for microbes to breed. By the time you get to doing your washing, the towel and the other laundry around it may have acquired a bad smell. And it can be difficult to get your towels smelling fresh again.
Towels should be washed more often than sheets.
New Africa/ShutterstockWhat about ‘self-cleaning’ sheets and towels?
Some companies sell “quick-dry” towels or “self-cleaning” towels and bedding. Quick-dry towels are made from synthetic materials that are weaved in a way to allow them to dry quickly. This would help prevent the growth of microbes and the bad smells that develop when towels are damp for long periods of time.
But the notion of self-cleaning products is more complicated. Most of these products contain nanosilver or copper, antibacterial metals that kill micro-organisms. The antibacterial compounds will stop the growth of bacteria and can be useful to limit smells and reduce the frequency with which you need to clean your sheets and towels.
However, they’re not going to remove dirt like oils, skin flakes and sweat. So as much as I would love the idea of sheets and towels that clean themselves, that’s not exactly what happens.
Also, excessive use of antimicrobials such as nanosilver can lead to microbes becoming resistant to them.

Rietie Venter, Associate professor, Clinical and Health Sciences, University of South Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Cherries vs Dates – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing cherries to dates, we picked the dates.
Why?
Cherries are great too! But…
In terms of macros, dates have more fiber and carbs, for a comparable glycemic index, making dates the more nutrient-dense option in the macros category.
In the category of vitamins, cherries have more of vitamins A, C, and E, while dates have more of vitamins B1, B2, B3, B5, B6, B7, B9, K, and choline—another win for dates.
Looking at minerals, cherries are not higher in any mineral*, while dates are higher in calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc. One more win for dates!
*Well, technically cherries are marginally higher in sodium, but it’s a tiny amount in both cases, so let’s disregard that as irrelevant.
When it comes to phytochemicals, it’s worth noting that cherries do have some beneficial properties beyond what dates have (see the link below for more about those).
Adding up the sections makes for an overall win for dates, but by all means enjoy either or both; they’re both very beneficial!
Want to learn more?
You might like:
Cherries’ Very Healthy Wealth Of Benefits!
Enjoy!
Share This Post
-
South Indian-Style Chickpea & Mango Salad
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We have a double-dose of chickpeas today, but with all the other ingredients, this dish is anything but boring. Fun fact about chickpeas though: they’re rich in sitosterol, a plant sterol that, true to its name, sits on cholesterol absorption sites, reducing the amount of dietary cholesterol absorbed. If you are vegan, this will make no difference to you because your diet does not contain cholesterol, but for everyone else, this is a nice extra bonus!
You will need
- 1 can white chickpeas, drained and rinsed
- 1 can black chickpeas (kala chana), drained and rinsed
- 9 oz fresh mango, diced (or canned is fine if that’s what’s available)
- 1½ oz ginger, peeled and grated
- 2 green chilis, finely chopped (adjust per heat preferences)
- 2 tbsp desiccated coconut (or 3 oz grated coconut, if you have it fresh)
- 8 curry leaves (dried is fine if that’s what’s available)
- 1 tsp mustard seeds
- 1 tsp cumin seeds
- 1 tsp black pepper, coarse ground
- ½ tsp MSG or 1 tsp low-sodium salt
- Juice of 1 lime
- Extra virgin olive oil
Method
(we suggest you read everything at least once before doing anything)
1) Heat some oil in a skillet over a medium heat. When it’s hot but not smoking, add the ginger, chilis, curry leaves, mustard seeds, and cumin seeds, stirring well to combine, keep going until the mustard seeds start popping.
2) Add the chickpeas (both kinds), as well as the black pepper and the MSG/salt. Once they’re warm through, take it off the heat.
3) Add the mango, coconut, and lime juice, mixing thoroughly.
4) Serve warm, at room temperature, or cold:

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- What Matters Most For Your Heart?
- Can Saturated Fats Be Healthy?
- Our Top 5 Spices: How Much Is Enough For Benefits?
Take care!
Share This Post



Related Posts
-
5 Golden Rules To Lose Belly Fat
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our belly is often the first place we gain fat and the last to lose it—due to hormonal changes, poor blood flow, and fat cell types. This also means that weight loss efforts can result in it looking worse before it looks better, as we lose weight from elsewhere around it. But, there is a way forwards:
What to do about it
Cori Lefkowith, of “Redefining Strength” and “Strength At Any Age” fame, advise that we follow the following “5 golden rules”:
- Mindset: avoid “All or Nothing” thinking; focus on small, sustainable changes and consistent habits.
- Macros: prioritize protein (40%+ of calories), balance fats and carbs for hormonal health, and avoid extreme calorie deficits (your body will try to save you from starvation by slowing your metabolism to conserve energy, and storing fat).
- Nutrition quality: focus on whole, nutrient-dense foods for better satiety, gut health, and energy. Get plenty of fiber and water; your body still needs those too.
- Muscle building: strength training preserves muscle, boosts metabolism, and improves body composition—don’t ditch your strength training for cardio; it won’t help and that swap would hinder..
- Daily walks: 15–20 minutes of walking after dinner aids digestion, and reduces stress (remember: stress invites your body to store extra fat, especially at the belly). It also incidentally burns calories without stressing the body, but honestly, it’s really not very many calories, so that’s not the main reason to do it.
For more on each of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Visceral Belly Fat & How To Lose It ← this is not the same thing as subcutaneous fat; the remedy is partly the same though, and it’s important to do both if you’re carrying excess weight both on your belly and in your viscera, if you want to reduce your overall waist size.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Four Easy Ways To Better Shoulder Mobility
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Shoulders are important, and often neglected by women who do not generally have the same social impetus to have large shoulders as men do.
But, size won’t happen by accident, so please do train strength, because yes, strength is necessary for mobility. And why is strength necessary?
Think of it this way: if your car has wheels but no engine power, then it can be moved by outside forces yes, but it’s not really fulfilling the job requirements of “automobile“, is it?
Same deal with your shoulders. If your shoulders can be moved through a range of motion much further than they have the power to move themselves, then that’s not mobility, that’s hypermobility and it’s a liability.
That’s how you end up pulling a muscle while reaching something from a high shelf.
So instead…
From the thoracic up
Here are four easy ways to do it:
- Dumbbell pullover: lie on a bench with your feet on the floor and your lower back in neutral. Hold a dumbbell above your chest with a slight bend in your elbows, then lower the weight behind your head in an arc while keeping your core tight so your ribs and hip bones draw towards each other; avoid letting your lower back over-arch so your lats stay stretched. Exhale as you bring the weight back above your chest, to build lat, chest, thoracic, and shoulder strength and mobility.
- Hand-elevated push-up: put your hands on yoga blocks set slightly wider than your shoulders. Keep your shoulders over your wrists and your tailbone slightly tucked, and lower your chest between the blocks to put your pecs and delts into a deeper stretch than a regular push-up, increasing strength through a fuller range.
- Around the world: stand tall with dumbbells at your sides, palms forwards; keep a soft bend in your elbows as you draw wide circles up until the weights meet overhead. Let your shoulder blades move naturally—starting low, rising into elevation as your arms pass shoulder height, then lowering again on the return, to strengthen your rotator cuff and expand your shoulder mobility beyond a standard lateral raise.
- Y-shaped chest fly: lie on a bench with feet planted on the floor; hold dumbbells in a slight V-shape with palms facing your head; keep your core tight and lower your arms into a wide Y-shape to stretch your chest fully; squeeze your mid-chest to bring the weights back over your chest. This one’s an excellent antidote for desk, car, and couch postures, by the way.
For more on all of this plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Shoulder Mobility Hack (Measurable Results In 60 Seconds)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What happens in my brain when I get a migraine? And what medications can I use to treat it?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Migraine is many things, but one thing it’s not is “just a headache”.
“Migraine” comes from the Greek word “hemicrania”, referring to the common experience of migraine being predominantly one-sided.
Some people experience an “aura” preceding the headache phase – usually a visual or sensory experience that evolves over five to 60 minutes. Auras can also involve other domains such as language, smell and limb function.
Migraine is a disease with a huge personal and societal impact. Most people cannot function at their usual level during a migraine, and anticipation of the next attack can affect productivity, relationships and a person’s mental health.
Francisco Gonzelez/Unsplash What’s happening in my brain?
The biological basis of migraine is complex, and varies according to the phase of the migraine. Put simply:
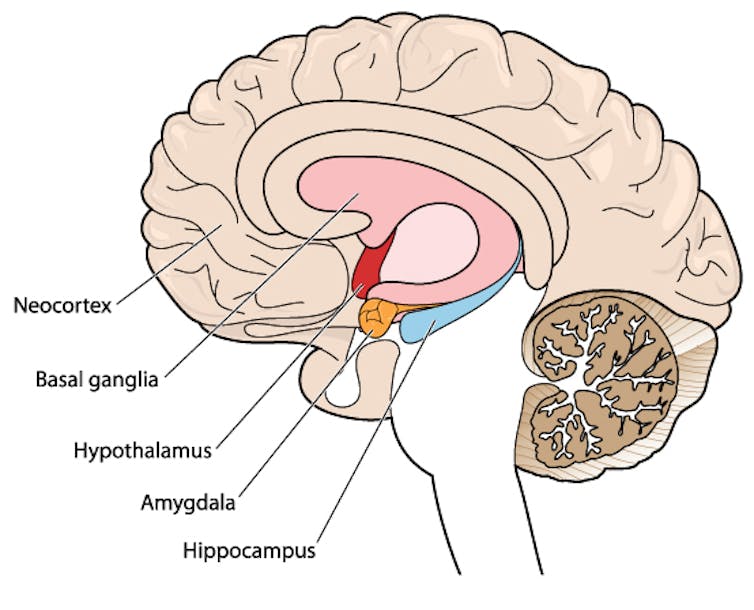
The earliest phase is called the prodrome. This is associated with activation of a part of the brain called the hypothalamus which is thought to contribute to many symptoms such as nausea, changes in appetite and blurred vision.
The hypothalamus is shown here in red. Blamb/Shutterstock Next is the aura phase, when a wave of neurochemical changes occur across the surface of the brain (the cortex) at a rate of 3–4 millimetres per minute. This explains how usually a person’s aura progresses over time. People often experience sensory disturbances such as flashes of light or tingling in their face or hands.
In the headache phase, the trigeminal nerve system is activated. This gives sensation to one side of the face, head and upper neck, leading to release of proteins such as CGRP (calcitonin gene-related peptide). This causes inflammation and dilation of blood vessels, which is the basis for the severe throbbing pain associated with the headache.
Finally, the postdromal phase occurs after the headache resolves and commonly involves changes in mood and energy.
What can you do about the acute attack?
A useful way to conceive of migraine treatment is to compare putting out campfires with bushfires. Medications are much more successful when applied at the earliest opportunity (the campfire). When the attack is fully evolved (into a bushfire), medications have a much more modest effect.
Aspirin
For people with mild migraine, non-specific anti-inflammatory medications such as high-dose aspirin, or standard dose non-steroidal medications (NSAIDS) can be very helpful. Their effectiveness is often enhanced with the use of an anti-nausea medication.
Triptans
For moderate to severe attacks, the mainstay of treatment is a class of medications called “triptans”. These act by reducing blood vessel dilation and reducing the release of inflammatory chemicals.
Triptans vary by their route of administration (tablets, wafers, injections, nasal sprays) and by their time to onset and duration of action.
The choice of a triptan depends on many factors including whether nausea and vomiting is prominent (consider a dissolving wafer or an injection) or patient tolerability (consider choosing one with a slower onset and offset of action).
As triptans constrict blood vessels, they should be used with caution (or not used) in patients with known heart disease or previous stroke.
Triptans should be used cautiously in patients with heart disease. CDC/Unsplash Gepants
Some medications that block or modulate the release of CGRP, which are used for migraine prevention (which we’ll discuss in more detail below), also have evidence of benefit in treating the acute attack. This class of medication is known as the “gepants”.
Gepants come in the form of injectable proteins (monoclonal antibodies, used for migraine prevention) or as oral medication (for example, rimegepant) for the acute attack when a person has not responded adequately to previous trials of several triptans or is intolerant of them.
They do not cause blood vessel constriction and can be used in patients with heart disease or previous stroke.
Ditans
Another class of medication, the “ditans” (for example, lasmiditan) have been approved overseas for the acute treatment of migraine. Ditans work through changing a form of serotonin receptor involved in the brain chemical changes associated with the acute attack.
However, neither the gepants nor the ditans are available through the Pharmaceutical Benefits Scheme (PBS) for the acute attack, so users must pay out-of-pocket, at a cost of approximately A$300 for eight wafers.
What about preventing migraines?
The first step is to see if lifestyle changes can reduce migraine frequency. This can include improving sleep habits, routine meal schedules, regular exercise, limiting caffeine intake and avoiding triggers such as stress or alcohol.
Despite these efforts, many people continue to have frequent migraines that can’t be managed by acute therapies alone. The choice of when to start preventive treatment varies for each person and how inclined they are to taking regular medication. Those who suffer disabling symptoms or experience more than a few migraines a month benefit the most from starting preventives.
Some people will take medicines to prevent migraines. Tbel Abuseridze/Unsplash Almost all migraine preventives have existing roles in treating other medical conditions, and the physician would commonly recommend drugs that can also help manage any pre-existing conditions. First-line preventives include:
- tablets that lower blood pressure (candesartan, metoprolol, propranolol)
- antidepressants (amitriptyline, venlafaxine)
- anticonvulsants (sodium valproate, topiramate).
Some people have none of these other conditions and can safely start medications for migraine prophylaxis alone.
For all migraine preventives, a key principle is starting at a low dose and increasing gradually. This approach makes them more tolerable and it’s often several weeks or months until an effective dose (usually 2- to 3-times the starting dose) is reached.
It is rare for noticeable benefits to be seen immediately, but with time these drugs typically reduce migraine frequency by 50% or more.
‘Nothing works for me!’
In people who didn’t see any effect of (or couldn’t tolerate) first-line preventives, new medications have been available on the PBS since 2020. These medications block the action of CGRP.
The most common PBS-listed anti-CGRP medications are injectable proteins called monoclonal antibodies (for example, galcanezumab and fremanezumab), and are self-administered by monthly injections.
These drugs have quickly become a game-changer for those with intractable migraines. The convenience of these injectables contrast with botulinum toxin injections (also effective and PBS-listed for chronic migraine) which must be administered by a trained specialist.
Up to half of adolescents and one-third of young adults are needle-phobic. If this includes you, tablet-form CGRP antagonists for migraine prevention are hopefully not far away.
Data over the past five years suggest anti-CGRP medications are safe, effective and at least as well tolerated as traditional preventives.
Nonetheless, these are used only after a number of cheaper and more readily available first-line treatments (all which have decades of safety data) have failed, and this also a criterion for their use under the PBS.
Mark Slee, Associate Professor, Clinical Academic Neurologist, Flinders University and Anthony Khoo, Lecturer, Flinders University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: