10almonds Tells The Tea…
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Let’s Bust Some Myths!
It’s too late after puberty, hormones won’t change xyz
While yes, many adult trans people dearly wish they’d been able to medically transition before going through the “wrong” puberty, the truth is that a lot of changes will still occur later… even to “unchangeable” things like the skeleton.
The body is remaking itself throughout life, and hormones tell it how to do that. Some parts are just quicker or slower than others. Also: the skeleton is pulled-on constantly by our muscles, and in a battle of muscle vs bone, muscle will always win over time.
Examples of this include:
- trans men building bigger bones to support their bigger muscles
- trans women getting smaller, with wider hips and a pelvic tilt
Trans people have sporting advantages
Assuming at least a year’s cross-sex hormonal treatment, there is no useful advantage to being trans when engaging in a sport. There are small advantages and disadvantages (which goes for any person’s body, really). For example:
- Trans women will tend to be taller than cis women on average…
- …but that larger frame is now being powered by smaller muscles, because they shrink much quicker than the skeleton.
- Trans men taking T are the only athletes allowed to take testosterone…
- …but they will still often be smaller than their fellow male competitors, for example.
Read: Do Trans Women Athletes Have Advantages? (A rather balanced expert overview, which does also cover trans men)
There’s a trans population explosion; it’s a social contagion epidemic!
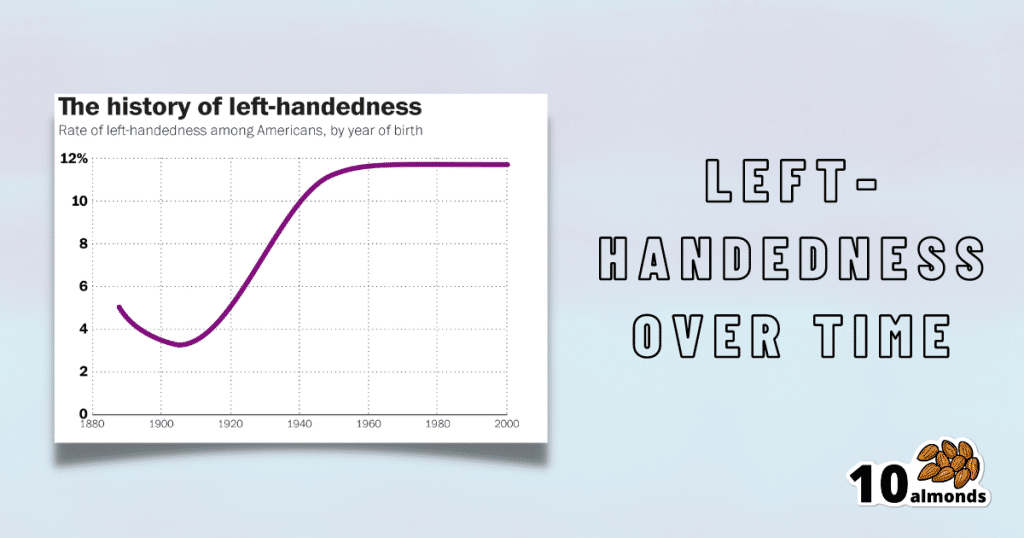
Source for figures: The Overall Rate Of Left-Handedness (Researchgate)
Left-handed people used to make up around 3% of the population… Until the 1920s, when that figure jumped sharply upwards, before plateauing at around 12% in around 1960, where it’s stayed since. What happened?! Simple, schools stopped forcing children to use their right hand.
Today, people ask for trans healthcare because they know it exists! Decades ago, it wasn’t such common knowledge.
The same explanation can be applied to other “population explosions” such as for autism and ADHD.
Fun fact: Mt. Everest was “discovered” in 1852, but scientists suspect it probably existed long before then! People whose ancestors were living on it long before 1852 also agree. Sometimes something exists for a long time, and only comes to wider public awareness later.
Transgender healthcare is too readily available, especially to children!
To believe some press outlets, you’d think:
- HRT is available from school vending machines,
- kids can get a walk-in top surgery at recess,
- and there’s an after-school sterilization club.
In reality, while availability varies from place to place, trans healthcare is heavily gatekept. Even adults have trouble getting it, often having to wait years and/or pay large sums of money… and get permission from a flock of doctors, psychologists, and the like. For those under the age of 18, it’s almost impossible in many places, even with parental support.
Puberty-blockers shouldn’t be given to teenagers, as the effects are irreversible
Quick question: who do you think should be given puberty-blockers? For whom do you think they were developed? Not adults, for sure! They were not developed for trans teens either, but for cis pre-teens with precocious puberty, to keep puberty at bay, to do it correctly later. Nobody argues they’re unsafe for much younger cis children, and only object when it’s trans teens.
They’re not only safe and reversible, but also self-reversing. Stop taking them, and the normally scheduled puberty promptly ensues by itself. For trans kids, the desired effect is to buy the kid time to make an informed and well-considered decision. After all, the effects of the wrong puberty are really difficult to undo!
A lot of people rush medical transition and regret it!
Trans people wish it could be rushed! It’s a lot harder to get gender-affirming care as a trans person, than it is to get the same (or comparable) care as a cis person. Yes, cis people get gender-affirming care, from hormones to surgeries, and have done for a long time.
As for regret… Medical transition has around a 1% regret rate. For comparison, hip replacement has a 4.8% regret rate and knee replacement has a 17.1% regret rate.
A medical procedure with a 99% success rate would generally be considered a miracle cure!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:

Younger Next Year – by Chris Crowley & Dr. Henry Lodge

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Is it diet and exercise? Well, of course that’s a component. Specific kinds of exercise, too. But, as usual when we feature a book, there’s more:
In this case, strong throughout is the notion of life being a marathon not a sprint—and training for it accordingly.
Doing the things now that you’ll really wish you’d started doing sooner, and finding ways to build them into daily life.
Not just that, though! The authors take a holistic approach to life and health, and thus also cover work life, social life, and so forth. Now, you may be thinking “I’m already in the 80 and beyond category; I don’t work” and well, the authors advise that you do indeed work. You don’t have to revamp your career, but science strongly suggests that people who work longer, live longer.
Of course that doesn’t have to mean going full-throttle like a 20-year-old determined to make their mark on the world (you can if you want, though). It could be volunteering for a charity, or otherwise just finding a socially-engaging “work-like” activity that gives you purpose.
About the blend of motivational pep talk and science—this book is heavily weighted towards the former. It has, however, enough science to keep it on the right track throughout. Hence the two authors! Crowley for motivational pep, and Dr. Lodge for the science (with extra input from brain surgeon Dr. Hamilton, too).
Bottom line: if you want to feel the most prepared possible for the coming years and decades, this is a great book that covers a lot of bases.
Click here to check out “Younger Next Year” and get de-aging!
Share This Post

Age & Aging: What Can (And Can’t) We Do About It?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How old do you want to be?

We asked you how old you are, and got an interesting spread of answers. This wasn’t too surprising; of course we have a general idea of who our readership is and we write accordingly.
What’s interesting is the gap for “40s”.
And, this wasn’t the case of a broken poll button, it’s something that crops up a lot in health-related sociological research. People who are most interested in taking extra care of their body are often:
- Younger people full of optimism about maintaining this perfectly healthy body forever
- Older people realizing “if I don’t want to suffer avoidable parts of age-related decline, now is the time to address these things”
In between, we often have a gap whereby people no longer have the optimism of youth, but do not yet feel the pressure of older age.
Which is not to say there aren’t 40-somethings who do care! Indeed, we know for a fact we have some subscribers in their 40s (and some in their 90s, too), just, they evidently didn’t vote in this poll.
Anyway, let’s bust some myths…
Aging is inevitable: True or False?
False, probably. That seems like a bold (and fortune-telling) claim, so let’s flip it to deconstruct it more logically:
Aging is, and always will be, unstoppable: True or False?
That has to be “False, probably”. To say “true” now sounds like an even bolder claim. Just like “the moon will always be out of reach”.
- When CPR was first developed, first-aiders were arrested for “interfering with a corpse”.
- Many diseases used to be death sentences that are now “take one of these in the morning”
- If you think this is an appeal to distant history, HIV+ status was a death sentence in the 90s. Now it’s “take one of these in the morning”.
But, this is an appeal to the past, and that’s not always a guarantee of the future. Where does the science stand currently? How is the research and development doing on slowing, halting, reversing aging?
We can slow aging: True or False?
True! There’s a difference between chronological age (i.e., how much time has passed while we’ve been alive) and biological age (i.e., what our diverse markers of aging look like).
Biological age often gets talked about as a simplified number, but it’s more complex than that, as we can age in different ways at different rates, for example:
- Visual markers of aging (e.g. wrinkles, graying hair)
- Performative markers of aging (e.g. mobility tests)
- Internal functional markers of aging (e.g. tests for cognitive decline, eyesight, hearing, etc)
- Cellular markers or aging (e.g. telomere length)
- …and more, but we only have so much room here
There are things we can do to slow most of those, including:
- Good nutrition (e.g. collagen and lutein, to keep specific parts of the body functioning “like those of a younger person” ranging from the joints to the eyes and brain)
- Anti-oxidant activity (e.g. eating anti-oxidant foods, supplementing with anti-oxidants or other things that mitigate oxidative stress, and avoiding foods that hasten oxidative stress which causes many kinds of aging)
- Getting good sleep (not to be underestimated for its restorative importance)
- Taking care of our cognitive health
- Taking care of our mental health (especially: reducing stress)
- Taking care of our mobility (prevention is better than cure!)
In the case of cognitive decline particularly, check out our previous article:
How To Reduce Your Alzheimer’s Risk
It’s too early to worry about… / It’s too late to do anything about… True or False?
False and False!
Many things that affect our health later in life are based on early-life choices and events. So it’s important for young people to take advantage of that. The earlier one adopts a healthy lifestyle, the better, because, and hold onto your hats for the shocker here: aging is cumulative.
However, that doesn’t mean that taking up healthy practices (or dropping unhealthy ones) is pointless later in life, even in one’s 70s and beyond!
Read about this and more from the National Institute of Aging:
What Do We Know About Healthy Aging?
We can halt aging: True or False?
False, for now at least. Our bodies are not statues; they are living organisms, constantly rebuilding themselves, constantly changing, every second of every day, for better or for worse. Every healthy or unhealthy choice you make, every beneficial or adverse experience you encounter, affects your body on a cellular level.
Your body never, ever, stops changing for as long as you live.
But…
We can reverse aging: True or False?
True! Contingently and with limitations, for now at least.
Remember what we said about your body constantly rebuilding itself? That goes for making itself better as well as making itself worse.
- If yesterday you couldn’t touch your toes and today you can, congratulations, you just got younger by a biological marker of aging.
- If you stopped drinking/smoking/eating a certain way last year, and this year your skin has fewer wrinkles, congratulations, you got younger by a biological marker of aging.
- If you’ve been exercising and now your heart rate variability and VO2 max are better than last month, congratulations, you got younger by a biological marker aging.
- If you took supplements that reduce and/or mitigate oxidative stress (e.g. resveratrol, CoQ10, l-theanine, etc), and you took up intermittent fasting, and now your telomeres are longer than they were six months ago, congratulations, you got younger by a biological marker of aging.
But those aren’t really being younger, we’ll still die when our time is up: True or False?
False and True, respectively.
Those kinds of things are really being younger, biologically. What else do you think being biologically younger is?
We may indeed die when our time is up, but (unless we suffer fatal accident or incident first) “when our time is up” is something that is decided mostly by the above factors.
Genetics—the closest thing we have to biological “fate”—accounts for only about 25% of our longevity-related health*.
Genes predispose, but they don’t predetermine.
*Read more: Human longevity: Genetics or Lifestyle? It takes two to tango
(from the Journal of Immunity and Ageing)
Share This Post

What To Eat, Take, And Do Before A Workout
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What to eat, take, and do before a workout
We’ve previously written about how to recover quickly after a workout:
Overdone It? How To Speed Up Recovery After Exercise
Today we’ll look at the flipside: how to prepare for exercise.
Pre-workout nutrition
As per what we wrote (and referenced) above, a good dictum is “protein whenever; carbs after”. See also:
Pre- versus post-exercise protein intake has similar effects on muscular adaptations
It’s recommended to have a light, balanced meal a few hours before exercising, though there are nuances:
International society of sports nutrition position stand: nutrient timing
Hydration
You will not perform well unless you are well-hydrated:
Influence of Dehydration on Intermittent Sprint Performance
However, you also don’t want to just be sloshing around when exercising because you took care to get in your two litres before hitting the gym.
For this reason, quality can be more important than quantity, and sodium and other electrolytes can be important and useful, but will not be so for everyone in all circumstances.
Here’s what we wrote previously about that:
Are Electrolyte Supplements Worth It?
Pre-workout supplements
We previously wrote about the use of creatine specifically:
Creatine: Very Different For Young & Old People
Caffeine is also a surprisingly effective pre-workout supplement:
International society of sports nutrition position stand: caffeine and exercise performance
Depending on the rate at which you metabolize caffeine (there are genes for this), the effects will come/go earlier/later, but as a general rule of thumb, caffeine should work within about 20 minutes, and will peak in effect 1–2 hours after consumption:
Nutrition Supplements to Stimulate Lipolysis: A Review in Relation to Endurance Exercise Capacity
Branched Chain Amino Acids, or BCAAs, are commonly enjoyed as pre-workout supplement to help reduce creatine kinase and muscle soreness, but won’t accelerate recovery:
…but will help boost muscle-growth (or maintenance, depending on your exercise and diet) in the long run:
Where can I get those?
We don’t sell them, but here’s an example product on Amazon, for your convenience
There are also many multi-nutrient pre-workout supplements on the market (like the secondary product offered with the BCAA above). We’d need a lot more room to go into all of those (maybe we’ll include some in our Monday Research Review editions), but meanwhile, here’s some further reading:
The 11 Best Pre-Workout Supplements According to a Dietitian
(it’s more of a “we ranked these commercial products” article than a science article, but it’s a good starting place for understanding about what’s on offer)
Enjoy!
Share This Post

Related Posts

Rewire Your OCD Brain – by Dr. Catherine Pittman & Dr. William Youngs
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
OCD is just as misrepresented in popular media as many other disorders, and in this case, it’s typically not “being a neat freak” or needing to alphabetize things, so much as having uncontrollable obsessive intrusive thoughts, and often in response to those, unwanted compulsions. This can come from unchecked spiralling anxiety, and/or PTSD, for example.
What Drs. Pittman & Young offer is an applicable set of solutions, to literally rewire the brain (insofar as synapses can be considered neural wires). Leveraging neuroplasticity to work with us rather than against us, the authors talk us through picking apart the crossed wires, and putting them back in more helpful ways.
This is not, by the way, a book of CBT, though it does touch on that too.
Mostly, the book explains—clearly and simply and sometimes with illustrations—what is going wrong for us neurologically, and how to neurologically change that.
Bottom line: whether you have OCD or suffer from anxiety or just need help dealing with obsessive thoughts, this book can help a lot in, as the title suggests, rewiring that.
Click here to check out Rewire Your OCD Brain, and banish obsessive thoughts!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:

7 Steps to Get Off Sugar and Carbohydrates – by Susan Neal
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We will not keep the steps a mystery; abbreviated, they are:
- decide to really do this thing
- get knowledge and support
- clean out that pantry/fridge/etc and put those things behind you
- buy in healthy foods while starving your candida
- plan for an official start date, so that everything is ready
- change the way you eat (prep methods, timings, etc)
- keep on finding small ways to improve, without turning back
Particularly important amongst those are starving the candida (the fungus in your gut that is responsible for a lot of carb cravings, especially sugar and alcohol—which latter can be broken down easily into sugar), and changing the “how” of eating as well as the “what”; those are both things that are often overlooked in a lot of guides, but this one delivers well.
Walking the reader by the hand through things like that is probably the book’s greatest strength.
In the category of subjective criticism, the author does go off-piste a little at the end, to take a moment while she has our attention to talk about other things.
For example, you may not need “Appendix 7: How to Become A Christian and Disciple of Jesus Christ”.
Of course if that calls to you, then by all means, follow your heart, but it certainly isn’t a necessary step of quitting sugar. Nevertheless, the diversion doesn’t detract from the good dietary change advice that she has just spent a book delivering.
Bottom line: there’s no deep science here, but there’s a lot of very good, very practical advice, that’s consistent with good science.
Click here to check out 7 Steps to Get Off Sugar, and watch your health improve!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:

Managing Major Chronic Diseases – by Alexis Dupree
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our author, Alexis Dupree, is herself in her 70s, and writing with more than three decades of experience of surviving multiple chronic diseases (in her case, Multiple Sclerosis, and then a dozen comorbidities that came with such).
She is not a doctor or a scientist, but for more than 30 years she’s been actively working to accumulate knowledge not just on her own conditions, but on the whole medical system, and what it means to be a “forever patient” without giving up hope.
She talks lived-experience “life management” strategies for living with chronic disease, and she talks—again from lived experience—about navigating the complexities of medical care; not on a legalistic “State regulations say…” level, because that kind of thing changes by the minute, but on a human level.
Perhaps most practically: how to advocate strongly for yourself while still treating medical professionals with the respect and frankly compassion that they deserve while doing their best in turn.
But also: how to change your attitude to that of a survivor, and yet also redefine your dreams. How to make a new game plan of life—while working to make life easier for yourself. How to deal, psychologically, with the likelihood that not only will you probably not get better, but also, you will probably get worse, while still never, ever, giving up.
After all, many things are easily treatable today that mere decades ago were death sentences, and science is progressing all the time. We just have to stay alive, and in as good a condition as we reasonably can, to benefit from those advances!
Bottom line: if you have a chronic disease, or if a loved one does, then this is an immensely valuable book to read.
Click here to check out Managing Major Chronic Diseases, and make life easier!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: