The Sardinian Cholesterol Paradox
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Broadly speaking, low-density lipoprotein (LDL), or “bad” cholesterol, is generally considered to be… Well… Bad. Specifically because of how it can functionally narrow arteries, causing bits of floating detritus to get stuck in it, narrow it further, and eventually harden into atherosclerotic plaque, at which point it becomes even harder for the body to clear out.
We wrote about the process here: Demystifying Cholesterol
When it comes to cholesterol, the most common lay understanding (especially under a certain age) is “it’s bad”.
A more informed view (and more common after a certain age) is “LDL cholesterol is bad; HDL cholesterol is good”.
A more nuanced view is “LDL cholesterol is established as significantly associated with (and almost certainly a causal factor of) atherosclerotic cardiovascular disease and related mortality in men; in women it is less strongly associated and may or may not be a causal factor”
We wrote more about that, here: Statins: His & Hers? ← despite most research being on men, statins have very different effects (and side effects) for women, often being relatively less useful, and more dangerous. There are exceptions (for some women’s specific profiles they can still be worthwhile), but the trend is certainly troubling.
What, then, of Sardinia?
Sardinia is well-known for being one of the “Supercentenarian Blue Zones”, a place whose inhabitants enjoy (on average, statistically) unusually healthy longevity. These places have been looked to for clues as to how to live the healthiest life.
For example: From Blue To Green: News From The Centenarian Blue Zones
However, researchers recently were investigating life in a region of Sardinia where a lot of people are aged 90+, and followed the health of 168 of them for up to 6 years (because in the case of those who died during that time, obviously the time was less than 6 years).
Note: because this was specifically a Blue Zones study, they only included participants of whom all four grandparents were born within the Blue Zone—so not, for example, looking at the health of someone who just moved there from New York, say.
They collected a lot of interesting data (of course), but what we’re talking about today is that they found that participants with LDL levels above 130 mg/dL had a significantly longer average survival than those with LDL levels below this threshold. Specifically, a 40% lower mortality risk.
This is interesting, because LDL levels ≥130 mg/dL are considered moderate hypercholesterolemia (i.e., the LDL levels are a bit too high).
However, if the same participants had total cholesterol levels over 250mg/dL, they got no extra survival benefits, and very high cholesterol was still linked with shorter survival.
You can read the paper here: The Cholesterol Paradox in Long-Livers from a Sardinia Longevity Hot Spot (Blue Zone)
But before you reach for the butter…
The researchers have several hypotheses about why these results could be so, including:
- The longevity has less to do with LDL itself, and more to do with the diet, with the ratio of grain to olive oil.
- Most of the participants with higher LDL cholesterol were on antihypertensive drugs, which a) will obviously have a cardioprotective effect, and b) means that their heart health is probably enjoying greater scrutiny, and medical scrutiny can also have a protective effect (indeed, that’s the point of it).
- It was also speculated that the locals of that region may have a genetic defense against the harm of moderate hypercholesterolemia, due to historical exposure to malaria meaning that naturally slightly higher cholesterol levels without increased cardiovascular risk may have been naturally selected-for (i.e. those without it were more likely to die of malaria and not pass on their genes).
Thus, it may be that it’s not so applicable more generally. However, it is still reason to at least re-examine how bad LDL cholesterol actually is, and whether for some demographics it could have a protective factor (much like “overweight” BMI is a protective factor for people over 65).
Still, if you’d like to keep on top of your cholesterol levels, check out:
How To Lower Cholesterol Naturally, Without Statins
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Breaking Free from Emotional Eating – Geneen Roth

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The isn’t a book about restrictive dieting, or even willpower. Rather, it’s about making the unconscious conscious, and changing your relationship with food from being one of compulsion, to one of choice, wherein you also get the choice of saying “no”.
Roth takes us through the various ways in which life seems to conspire to take consciousness away from eating, from obvious distractions such as TV, to less obvious ones, like “it doesn’t count if you’re not sitting down”. She also tackles other psychological aspects, such as those people get from parents—which can be a big factor for many.
Importantly, she teaches us that when it comes to “have your cake and eat it”, you can also, in fact, have your cake and not eat it. That’s an option too. Its mere presence in our house is not the boss of us. However, overcoming the “this then that” automatic process that goes from having to eating, is something that Roth gives quite some attention to, offering a number of reframes to make it a lot easier.
The style is friendly, conversational, pop-science, and the format dates it a little—this is very much a book formatted the way pop-science books were formatted 20–50 years ago (the book itself is from 2003, for what it’s worth). However, a lack of modern format doesn’t take away from its very valuable insights, and if anything, the older format rather promotes reading a book from cover to cover, which can be beneficial.
Bottom line: if emotional or compulsive eating is something that you’ve found tricky to overcome, then this book can help make it a lot easier.
Share This Post
-

The Most Annoying Nutrition Tips (7 Things That Actually Work)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You can’t out-exercise a bad diet, and getting a good diet can be a challenge depending on your starting point. Here’s Cori Lefkowith’s unglamorous seven-point plan:
Step by step
Seven things to do:
- Start tracking first: track your food intake (as it is, without changing anything) without judgment to identify realistic areas for improvement.
- Add protein: add 10g of protein to three meals daily to improve satiety, aid fat loss, and retain muscle.
- Fiber swaps: swap foods for higher-fiber options where possible to improve gut health, improve heart health, support fat loss, and promote satiety.
- Hydration: take your body weight in kilograms (or half your body weight in pounds), then get that many ounces of water daily to support metabolism and reduce cravings.
- Calorie swaps: replace or reduce calorie-dense foods to create a small, modestly sustainable calorie deficit. Your body will still adjust to this after a while; that’s fine; it’s about a gradual reduction.
- Tweak and adjust: regularly reassess and adjust your diet and habits to fit your lifestyle and progress.
- Guard against complacency: track consistently, and stay on course.
For more on all of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
The Smartest Way To Get To 20% Body Fat (Or 10% For Men)
Take care!
Share This Post
-
What Harm Can One Sleepless Night Do?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ll not bury the lede: a study found that just one night of 24-hour sleep deprivation can alter immune cell profiles in young, lean, healthy people to resemble those of people with obesity and chronic inflammation.
Chronic inflammation, in turn, causes very many other chronic diseases, and worsens most of the ones it doesn’t outright cause.
The reason this happens is because in principle, inflammation is supposed to be good for us—it’s our body’s defenses coming to the rescue. However, if we imagine our immune cells as firefighters, then compare:
- A team of firefighters who are in great shape and ready to deploy at a moment’s notice, are mostly allowed to rest, sometimes get training, and get called out to a fire from time time, just enough to keep them on their toes. Today, something in your house caught fire, and they showed up in 5 minutes and put it out safely.
- A team of firefighters who have been pulling 24-hour shifts every day for the past 20 years, getting called out constantly for lost cats, burned toast, wrong numbers, the neighbor’s music, a broken fridge, and even the occasional fire. Today, your printer got jammed so they broke down your door and also your windows just for good measure, and blasted your general desk area with a fire hose, which did not resolve the problem but now your computer itself is broken.
Which team would you rather have?
The former team is a healthy immune system; the latter is the immune system of someone with chronic inflammation.
But if it’s one night, it’s not chronic, right?
Contingently true. However, the problem is that because the immune profile was made to be like the bad team we described (imagine that chaos in your house, now remember that for this metaphor, it’s your body that that’s happening to), the immediate strong negative health impact will already have knock-on effects, which in turn make it more likely that you’ll struggle to get your sleep back on track quickly.
For example, the next night you may oversleep “to compensate”, but then the following day your sleep schedule is now slid back considerably; one thing leads to another, and a month later you’re thinking “I really must sort my sleep out”.
See also: How Regularity Of Sleep Can Be Even More Important Than Duration ← A recent, large (n=72,269) 8-year prospective* observational study of adults aged 40-79 found a strong association between irregular sleep and major cardiovascular events, to such an extent that it was worse than undersleeping.
*this means they started the study at a given point, and measured what happened for the next eight years—as opposed to a retrospective study, which would look at what had happened during the previous 8 years.
What about sleep fragmentation?
In other words: getting sleep, but heavily disrupted sleep.
The answer is: basically the same deal as with missed sleep.
Specifically, elevated proinflammatory cytokines (in this context, that’s bad) and an increase in nonclassical monocytes—as are typically seen in people with obesity and chronic inflammation.
Remember: these were young, lean, healthy participants going into the study, who signed up for a controlled sleep deprivation experiment.
This is important, because the unhealthy inflammatory profile means that people with such are a lot more likely to develop diabetes, heart disease, Alzheimer’s, and many more things besides. And, famously, most people in the industrialized world are not sleeping that well.
Even amongst 10almonds readers, a health-conscious demographic by nature, 62% of 10almonds readers do not regularly get the prescribed 7–9 hours sleep (i.e. they get under 7 hours).
You can see the data on this one, here: Why You Probably Need More Sleep ← yes, including if you are in the older age range; we bust that myth in the article too!*
*Unless you have a (rare!) mutated ADRB1 gene, which reduces that. But we also cover that in the article, and how to know whether you have it.
With regard to “most people in the industrialized world are not sleeping that well”, this means that most people in the industrialized world are subject to an unseen epidemic of sleep-deprivation-induced inflammation that is creating vulnerability to many other diseases. In short, the lifestyle of the industrialized world (especially: having to work certain hours) is making most of the working population sick.
Dr. Fatema Al-Rashed, lead researcher, concluded:
❝In the long term, we aim for this research to drive policies and strategies that recognize the critical role of sleep in public health.
We envision workplace reforms and educational campaigns promoting better sleep practices, particularly for populations at risk of sleep disruption due to technological and occupational demands.
Ultimately, this could help mitigate the burden of inflammatory diseases like obesity, diabetes, and cardiovascular diseases.❞
You can read the paper in full here: Impact of sleep deprivation on monocyte subclasses and function
What can we do about it?
With regard to sleep, we’ve written so much about this, but here are three key articles that contain a lot of valuable information:
- Get Better Sleep: Beyond The Basics
- Calculate (And Enjoy) The Perfect Night’s Sleep
- Safe Effective Sleep Aids For Seniors
…and with regard to inflammation, a good concise overview of how to dial it down is:
How To Prevent Or Reduce Inflammation
Take care!
Share This Post
-

The FIRST Program: Fighting Insulin Resistance with Strength Training – by Dr. William Shang
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A lot of advice about fighting insulin resistance focuses on diet. And, that’s worthwhile! How we eat does make a huge difference to our insulin responses (as does fasting). But, we expect our regular 10almonds readers either know these things now, or can read one of several very good books we’ve already reviewed about such.
This one’s different: it focuses, as the title promises, on fighting insulin resistance with strength training. And why?
It’s because of the difference that our body composition makes to our metabolism. Now, our body fat percentage is often talked about (or, less usefully but more prevalently, even if woefully misleadingly, our BMI), but Dr. Shang makes the case for it being our musculature that has the biggest impact; because of how it hastens our metabolism, and because of how it is much healthier for the body to store glycogen in muscle tissue, than just cramming whatever it can into the liver and visceral fat. It becomes relevant, then, that there’s a limit to how much glycogen can be stored in muscle tissue, and that limit is how much muscle you have.
This is not, however, 243 pages to say “lift some weights, lazybones”. Rather, he explains the relevant pathophysiology (we will be more likely to adhere to things we understand, than things we do not), and gives practical advice on exercising the different kinds of muscle fibers, arguing that the whole is greater than the sum of its parts, as well as outlining an exercise program for the gym, plus a chapter on no-gym exercises too.
The style is quite dense, which may be offputting for some, but it suffices to take one’s time and read thoughtfully; the end result is worth it.
Bottom line: if you’d like to keep insulin resistance at bay, this book is an excellent extra tool for that.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How Much Can Hypnotherapy Really Do?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Sit Back, Relax, And…

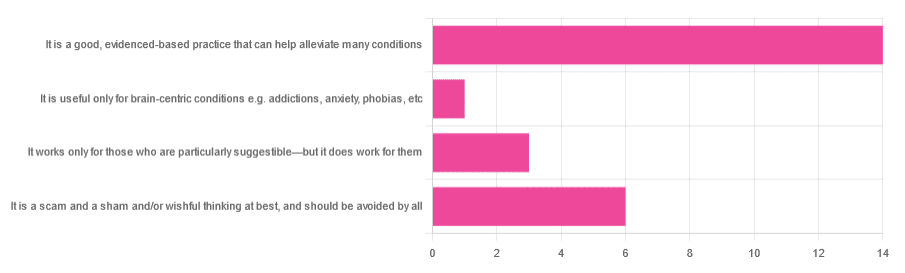
In Tuesday’s newsletter, we asked you for your opinions of hypnotherapy, and got the above-depicted, below-described, set of responses:
- About 58% said “It is a good, evidenced-based practice that can help alleviate many conditions”
- Exactly 25% said “It is a scam and sham and/or wishful thinking at best, and should be avoided by all”
- About 13% said “It works only for those who are particularly suggestible—but it does work for them”
- One (1) person said “It is useful only for brain-centric conditions e.g. addictions, anxiety, phobias, etc”
So what does the science say?
Hypnotherapy is all in the patient’s head: True or False?
True! But guess which part of your body controls much of the rest of it.
So while hypnotherapy may be “all in the head”, its effects are not.
Since placebo effect, nocebo effect, and psychosomatic effect in general are well-documented, it’s quite safe to say at the very least that hypnotherapy thus “may be useful”.
Which prompts the question…
Hypnotherapy is just placebo: True or False?
False, probably. At the very least, if it’s placebo, it’s an unusually effective placebo.
And yes, even though testing against placebo is considered a good method of doing randomized controlled trials, some placebos are definitely better than others. If a placebo starts giving results much better than other placebos, is it still a placebo? Possibly a philosophical question whose answer may be rooted in semantics, but happily we do have a more useful answer…
Here’s an interesting paper which: a) begins its abstract with the strong, unequivocal statement “Hypnosis has proven clinical utility”, and b) goes on to examine the changes in neural activity during hypnosis:
Brain Activity and Functional Connectivity Associated with Hypnosis
It works only for the very suggestible: True or False?
False, broadly. As with any medical and/or therapeutic procedure, a patient’s expectations can affect the treatment outcome.
And, especially worthy of note, a patient’s level of engagement will vastly affect it treatment that has patient involvement. So for example, if a doctor prescribes a patient pills, which the patient does not think will work, so the patient takes them intermittently, because they’re slow to get the prescription refilled, etc, then surprise, the pills won’t get as good results (since they’re often not being taken).
How this plays out in hypnotherapy: because hypnotherapy is a guided process, part of its efficacy relies on the patient following instructions. If the hypnotherapist guides the patient’s mind, and internally the patient is just going “nope nope nope, what a lot of rubbish” then of course it will not work, just like if you ask for directions in the street and then ignore them, you won’t get to where you want to be.
For those who didn’t click on the above link by the way, you might want to go back and have a look at it, because it included groups of individuals with “high/low hypnotizability” per several ways of scoring such.
It works only for brain-centric things, e.g. addictions, anxieties, phobias, etc: True or False?
False—but it is better at those. Here for example is the UK’s Royal College of Psychiatrists’ information page, and if you go to “What conditions can hypnotherapy help to treat”, you’ll see two broad categories; the first is almost entirely brain-stuff; the second is more varied, and includes pain relief of various kinds, burn care, cancer treatment side effects, and even menopause symptoms. Finally, warts and other various skin conditions get their own (positive) mention, per “this is possible through the positive effects hypnosis has on the immune system”:
RCPsych | Hypnosis And Hypnotherapy
Wondering how much psychosomatic effect can do?
You might like this previous article; it’s not about hypnotherapy, but it is about the difference the mind can make on physical markers of aging:
Aging, Counterclockwise: When Age Is A Flexible Number
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Dentists Are Pulling ‘Healthy’ and Treatable Teeth To Profit From Implants, Experts Warn
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Becky Carroll was missing a few teeth, and others were stained or crooked. Ashamed, she smiled with lips pressed closed. Her dentist offered to fix most of her teeth with root canals and crowns, Carroll said, but she was wary of traveling a long road of dental work.
Then Carroll saw a TV commercial for another path: ClearChoice Dental Implant Centers. The company advertises that it can give patients “a new smile in as little as one day” by surgically replacing teeth instead of fixing them.
So Carroll saved and borrowed for the surgery, she said. In an interview and a lawsuit, Carroll said that at a ClearChoice clinic in New Jersey in 2021, she agreed to pay $31,000 to replace all her natural upper teeth with pearly-white prosthetic ones. What came next, Carroll said, was “like a horror movie.”
Carroll alleged that her anesthesia wore off during implant surgery, so she became conscious as her teeth were removed and titanium screws were twisted into her jawbone. Afterward, Carroll’s prosthetic teeth were so misaligned that she was largely unable to chew for more than two years until she could afford corrective surgery at another clinic, according to a sworn deposition from her lawsuit.
ClearChoice has denied Carroll’s claims of malpractice and negligence in court filings and did not respond to requests for comment on the ongoing case.
“I thought implants would be easier, and all at once, so you didn’t have to keep going back to the dentist,” Carroll, 52, said in an interview. “But I should have asked more questions … like, Can they save these teeth?”
Dental implants have been used for more than half a century to surgically replace missing or damaged teeth with artificial duplicates, often with picture-perfect results. While implant dentistry was once the domain of a small group of highly trained dentists and specialists, tens of thousands of dental providers now offer the surgery and place millions of implants each year in the U.S.
Amid this booming industry, some implant experts worry that many dentists are losing sight of dentistry’s fundamental goal of preserving natural teeth and have become too willing to remove teeth to make room for expensive implants, according to a months-long investigation by KFF Health News and CBS News. In interviews, 10 experts said they had each given second opinions to multiple patients who had been recommended for mouths full of implants that the experts ultimately determined were not necessary. Separately, lawsuits filed across the country have alleged that implant patients like Carroll have experienced painful complications that have required corrective surgery, while other lawsuits alleged dentists at some implant clinics have persuaded, pressured, or forced patients to remove teeth unnecessarily.
The experts warn that implants, for a single tooth or an entire mouth, expose patients to costs and surgery complications, plus a new risk of future dental problems with fewer treatment options because their natural teeth are forever gone.
“There are many cases where teeth, they’re perfectly fine, and they’re being removed unnecessarily,” said William Giannobile, dean of the Harvard School of Dental Medicine. “I really hate to say it, but many of them are doing it because these procedures, from a monetary standpoint, they’re much more beneficial to the practitioner.”
Giannobile and nine other experts say they are combating a false public perception that implants are more durable and longer-lasting than natural teeth, which some believe stems in part from advertising on TV and social media. Implants require upkeep, and although they can’t get cavities, studies have shown that patients can be susceptible to infections in the gums and bone around their implants.
“Just because somebody can afford implants doesn’t necessarily mean that they’re a good candidate,” said George Mandelaris, a Chicago-area periodontist and member of the American Academy of Periodontology Board of Trustees. “When an implant has infection, or when an implant has bone loss, an implant dies a much quicker death than do teeth.”
In its simplest form, implant surgery involves extracting a single tooth and replacing it with a metal post that is screwed into the jaw and then affixed with a prosthetic tooth commonly made of porcelain, also known as a crown. Patients can also use “full-arch” or “All-on-4” implants to replace all their upper or lower teeth — or all their teeth.
For this story, KFF Health News and CBS News sought interviews with large dental chains whose clinics offer implant surgery — ClearChoice, Aspen Dental, Affordable Care, and Dental Care Alliance — each of which declined to be interviewed or did not respond to multiple requests for comment. The Association of Dental Support Organizations, which represents these companies and others like them, also declined an interview request.
ClearChoice, which specializes in full-arch implants, did not answer more than two dozen questions submitted in writing. In an emailed statement, the company said full-arch implants “have become a well-accepted standard of care for patients with severe tooth loss and teeth with poor prognosis.”
“The use of full-arch restorations reflects the evolution of modern dentistry, offering patients a solution that restores their ability to eat, speak, and live comfortably — far beyond what traditional dentures can provide,” the company said.
Carroll said she regrets not letting her dentist try to fix her teeth and rushing to ClearChoice for implants.
“Because it was a nightmare,” she said.
‘They Are Not Teeth’
Dental implant surgery can be a godsend for patients with unsalvageable teeth. Several experts said implants can be so transformative that their invention should have contended for a Nobel Prize. And yet, these experts still worry that implants are overused, because it is generally better for patients to have their natural teeth.
Paul Rosen, a Pennsylvania periodontist who said he has worked with implants for more than three decades, said many patients believe a “fallacy” that implants are “bulletproof.”
“You can’t just have an implant placed and go off riding into the sunset,” Rosen said. “In many instances, they need more care than teeth because they are not teeth.”
Generally, a single implant costs a few thousand dollars while full-arch implants cost tens of thousands. Neither procedure is well covered by dental insurance, so many clinics partner with credit companies that offer loans for implant surgeries. At ClearChoice, for example, loans can be as large as $65,000 paid off over 10 years, according to the company’s website.
Despite the price, implants are more popular than ever. Sales increased by more than 6% on average each year since 2010, culminating in more than 3.7 million implants sold in the U.S. in 2022, according to a 2023 report produced by iData Research, a health care market research firm.
Some worry implant dentistry has gone too far. In 10 interviews, dentists and dental specialists with expertise in implants said they had witnessed the overuse of implants firsthand. Each expert said they’d examined multiple patients in recent years who were recommended for full-arch implants by other dentists despite their teeth being treatable with conventional dentistry.
Giannobile, the Harvard dean, said he had given second opinions to “dozens” of patients who were recommended for implants they did not need.
“I see many of these patients now that are coming in and saying, ‘I’ve been seen, and they are telling me to get my entire dentition — all of my teeth — extracted.’ And then I’ll take a look at them and say that we can preserve most of your teeth,” Giannobile said.
Tim Kosinski, who is a representative of the Academy of General Dentistry and said he has placed more than 19,000 implants, said he examines as many as five patients a month who have been recommended for full-arch implants that he deems unnecessary.
“There is a push in the profession to remove teeth that could be saved,” Kosinski said. “But the public isn’t aware.”
Luiz Gonzaga, a periodontist and prosthodontist at the University of Florida, said he, too, had turned away patients who wanted most or all their teeth extracted. Gonzaga said some had received implant recommendations that he considered “an atrocity.”
“You don’t go to the hospital and tell them ‘I broke my finger a couple of times. This is bothering me. Can you please cut my finger off?’ No one will do that,” Gonzaga said. “Why would I extract your tooth because you need a root canal?”
Jaime Lozada, director of an elite dental implant residency program at Loma Linda University, said he’d not only witnessed an increase in dentists extracting “perfectly healthy teeth” but also treated a rash of patients with mouths full of ill-fitting implants that had to be surgically replaced.
Lozada said in August that he’d treated seven such patients in just three months.
“When individuals just make a decision of extracting teeth to make it simple and make money quick, so to speak, that’s where I have a problem,” Lozada said. “And it happens quite often.”
When full-arch implants fail, patients sometimes don’t have enough jawbone left to anchor another set. These patients have little choice but to get implants that reach into cheekbones, said Sohail Saghezchi, an oral and maxillofacial surgeon at the University of California-San Francisco.
“It’s kind of like a last resort,” Saghezchi said. “If those fail, you don’t have anywhere else to go.”
‘It Was Horrendous Dentistry’
Most of the experts interviewed for this article said their rising alarm corresponded with big changes in the availability of dental implants. Implants are now offered by more than 70,000 dental providers nationwide, two-thirds of whom are general dentists, according to the iData Research report.
Dentists are not required to learn how to place implants in dental school, nor are they required to complete implant training before performing the surgery in nearly all states. This year, Oregon started requiring dentists to complete 56 hours of hands-on training before placing any implants. Stephen Prisby, executive director of the Oregon Board of Dentistry, said the requirement — the first and only of its kind in the U.S. — was a response to dozens of investigations in the state into botched surgeries and other implant failures, split evenly between general dentists and specialists.
“I was frankly stunned at how bad some of these dentists were practicing,” Prisby said. “It was horrendous dentistry.”
Many dental clinics that offer implants have consolidated into chains owned by private equity firms that have bought out much of implant dentistry. In health care, private equity investment is sometimes criticized for overtreatment and prioritizing short-term profit over patients.
Private equity firms have spent about $5 billion in recent years to buy large dental chains that offer implants at hundreds of clinics owned by individual dentists and dental specialists. ClearChoice was bought for an estimated $1.1 billion in 2020 by Aspen Dental, which is owned by three private equity firms, according to PitchBook, a research firm focused on the private equity industry. Private equity firms also bought Affordable Care, whose largest clinic brand is Affordable Dentures & Implants, for an estimated $2.7 billion in 2021, according to PitchBook. And the private equity wing of the Abu Dhabi government bought Dental Care Alliance, which offers implants at many of its affiliated clinics, for an estimated $1 billion in 2022, according to PitchBook.
ClearChoice and Aspen Dental each said in email statements that the companies’ private equity owners “do not have influence or control over treatment recommendations.” Both companies said dentists or dental specialists make all clinical decisions.
Private equity deals involving dental practices increased ninefold from 2011 to 2021, according to an American Dental Association study published in August. The study also said investors showed an interest in oral surgery, possibly because of the “high prices” of implants.
“Some argue this is a negative thing,” said Marko Vujicic, vice president of the association’s Health Policy Institute, who co-authored the study. “On the other hand, some would argue that involvement of private equity and outside capital brings economies of scale, it brings efficiency.”
Edwin Zinman, a San Francisco dental malpractice attorney and former periodontist who has filed hundreds of dental lawsuits over four decades, said he believed many of the worst fears about private equity owners had already come true in implant dentistry.
“They’ve sold a lot of [implants], and some of it unnecessarily, and too often done negligently, without having the dentists who are doing it have the necessary training and experience,” Zinman said. “It’s for five simple letters: M-O-N-E-Y.”
Hundreds of Implant Clinics With No Specialists
For this article, journalists from KFF Health News and CBS News analyzed the webpages for more than 1,000 clinics in the nation’s largest private equity-owned dental chains, all of which offer some implants. The analysis found that more than 70% of those clinics listed only general dentists on their websites and did not appear to employ the specialists — oral surgeons, periodontists, or prosthodontists — who traditionally have more training with implants.
Affordable Dentures & Implants listed specialists at fewer than 5% of its more than 400 clinics, according to the analysis. The rest were staffed by general dentists, most of whom did not list credentialing from implant training organizations, according to the analysis.
ClearChoice, on the other hand, employs at least one oral surgeon or prosthodontist at each of its more than 100 centers, according to the analysis. But its new parent company, Aspen Dental, which offers implants in many of its more than 1,100 clinics, does not list any specialists at many of those locations.
Not everyone is worried about private equity in implant dentistry. In interviews arranged by the American Academy of Implant Dentistry, which trains dentists to use implants, two other implant experts did not express concerns about private equity firms.
Brian Jackson, a former academy president and implant specialist in New York, said he believed dentists are too ethical and patients are too smart to be pressured by private equity owners “who will never see a patient.”
Jumoke Adedoyin, a chief clinical officer for Affordable Care, who has placed implants at an Affordable Dentures & Implants clinic in the Atlanta suburbs for 15 years, said she had never felt pressure from above to sell implants.
“I’ve actually felt more pressure sometimes from patients who have gone around and been told they need to take their teeth out,” she said. “They come in and, honestly, taking a look at them, maybe they don’t need to take all their teeth out.”
Still, lawsuits filed across the country have alleged that dentists at implant clinics have extracted patients’ teeth unnecessarily.
For example, in Texas, a patient alleged in a 2020 lawsuit that an Affordable Care dentist removed “every single tooth from her mouth when such was not necessary,” then stuffed her mouth with gauze and left her waiting in the lobby as he and his staff left for lunch. In Maryland, a patient alleged in a 2021 lawsuit that ClearChoice “convinced” her to extract “eight healthy upper teeth,” by “greatly downplay[ing] the risks.” In Florida, a patient alleged in a 2023 lawsuit that ClearChoice provided her with no other treatment options before extracting all her teeth, “which was totally unnecessary.”
ClearChoice and Affordable Care denied wrongdoing in their respective lawsuits, then privately settled out of court with each patient. ClearChoice and Affordable Care did not respond to requests for comment submitted to the companies or attorneys. Lawyers for all three plaintiffs declined to comment on these lawsuits or did not respond to requests for comment.
Fred Goldberg, a Maryland dental malpractice attorney who said he has represented at least six clients who sued ClearChoice, said each of his clients agreed to get implants after meeting with a salesperson — not a dentist.
“Every client I’ve had who has gone to ClearChoice has started off meeting a salesperson and actually signing up to get their financing through ClearChoice before they ever meet with a dentist,” Goldberg said. “You meet with a salesperson who sells you on what they like to present as the best choice, which is almost always that they’re going to take out all your natural teeth.”
Becky Carroll, the ClearChoice patient from New Jersey, told a similar story.
Carroll said in her lawsuit that she met first with a ClearChoice salesperson referred to as a “patient education consultant.” In an interview, Carroll said the salesperson encouraged her to borrow money from family members for the surgery and it was not until after she agreed to a loan and passed a credit check that a ClearChoice dentist peered into her mouth.
“It seems way backwards,” Carroll said. “They just want to know you’re approved before you get to talk to a dentist.”
CBS News producer Nicole Keller contributed to this report.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
This article first appeared on KFF Health News and is republished here under a Creative Commons license.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: