

To Nap Or Not To Nap; That Is The Question
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝Is it good to nap in the afternoon, or better to get the famous 7 to 9 hours at night and leave it at that? I’m worried that daytime napping to make up for a shorter night’s sleep will just perpetuate and worsen it in the long run, is there a categorical answer here?❞
Generally considered best is indeed the 7–9 hours at night (yes, including at older ages):
Why You Probably Need More Sleep
…and sleep efficiency does matter too:
Why 7 Hours Sleep Is Not Enough
…which in turn, is influenced by factors other than just length and depth:
The 6 Dimensions Of Sleep (And Why They Matter)
However! Knowing what is best in theory does not help at all if it’s unattainable in practice. So, if you’re not getting a good night’s sleep (and we’ll assume you’re already practising good sleep hygiene; fresh bedding, lights-off by a certain time, no alcohol or caffeine before bed, that kind of thing), then a first port-of-call may be sleep remedies:
Safe Effective Sleep Aids For Seniors
If even those don’t work, then napping is now likely your best back-up option. But, napping done incorrectly can indeed cause as many problems as it solves. There’s a difference between:
- “I napped and now I have energy again” and you continue with your day
- “Darkness took me, and I strayed out of thought and time. Stars wheeled overhead, and every day was as long as the life age of the earth—but it was not the end.” and now you’re not sure whether it’s day or night, whose house you’re in, or whether you’ve been drugged.
These two very common napping experiences are influenced by factors that we can control:
How To Nap Like A Pro (No More “Sleep Hangovers”!)
If you still prefer to not risk napping but do need at least some kind of refreshment that’s actually a refreshment and not just taking stimulants, then you might consider this practice (from yoga nidra) that gives some of the same benefits of sleep, without actually sleeping:
Non-Sleep Deep Rest: A Neurobiologist’s Insights
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Is Chiropractic All It’s Cracked Up To Be?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Is Chiropractic All It’s Cracked Up To Be?

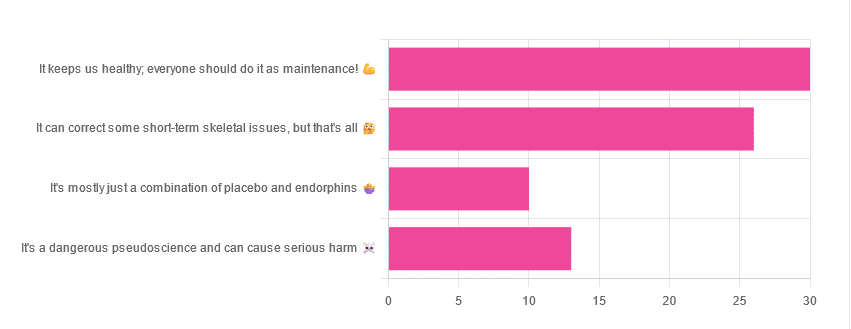
Yesterday, we asked you for your opinions on chiropractic medicine, and got the above-depicted, below-described set of results:
- 38% of respondents said it keeps us healthy, and everyone should do it as maintenance
- 33% of respondents said it can correct some short-term skeletal issues, but that’s all
- 16% of respondents said that it’s a dangerous pseudoscience and can cause serious harm
- 13% of respondents said that it’s mostly just a combination of placebo and endorphins
Respondents also shared personal horror stories of harm done, personal success stories of things cured, and personal “it didn’t seem to do anything for me” stories.
What does the science say?
It’s a dangerous pseudoscience and can cause harm: True or False?
Mixed and True, respectively.
That is to say, chiropractic in its simplest form that makes the fewest claims, is not a pseudoscience. If somebody physically moves your bones around, your bones will be physically moved. If your bones were indeed misaligned, and the chiropractor is knowledgeable and competent, this will be for the better.
However, like any form of medicine, it can also cause harm; in chiropractic’s case, because it more often than not involves manipulation of the spine, this can be very serious:
❝Twenty six fatalities were published in the medical literature and many more might have remained unpublished.
The reported pathology was usually vascular accidents involving the dissection of a vertebral artery.
Conclusion: Numerous deaths have occurred after chiropractic manipulations. The risks of this treatment by far outweigh its benefit.❞
Source: Deaths after chiropractic: a review of published cases
From this, we might note two things:
- The abstract doesn’t note the initial sample size; we would rather have seen this information expressed as a percentage. Unfortunately, the full paper is not accessible, and nor are many of the papers it cites.
- Having a vertebral artery fatally dissected is nevertheless not an inviting prospect, and is certainly a very reasonable cause for concern.
It’s mostly just a combination of placebo and endorphins: True or False?
True or False, depending on what you went in for:
- If you went in for a regular maintenance clunk-and-click, then yes, you will get your clunk-and-click and feel better for it because you had a ritualized* experience and endorphins were released.
- If you went in for something that was actually wrong with your skeletal alignment, to get it corrected, and this correction was within your chiropractor’s competence, then yes, you will feel better because a genuine fault was corrected.
*this is not implying any mysticism, necessarily, though that can certainly also be a component for many, and indeed, chiropractic was originally founded as a new religious movement. Outside of the context of spirituality, however, it means simply that placebo effect is strongest when there is a ritual associated with it. In this case it means going to the place, sitting in a pleasant waiting room, being called in, removing your shoes and perhaps some other clothes, getting the full attention of a confident and assured person for a while, this sort of thing.
With regard to its use to combat specifically spinal pain (i.e., perhaps the most obvious thing to treat by chiropractic spinal manipulation), evidence is slightly in favor, but remains unclear:
❝Due to the low quality of evidence, the efficacy of chiropractic spinal manipulation compared with a placebo or no treatment remains uncertain. ❞
Source: Clinical Effectiveness and Efficacy of Chiropractic Spinal Manipulation for Spine Pain
It can correct some short-term skeletal issues, but that’s all: True or False?
Probably True.
Why “probably”? The effectiveness of chiropractic treatment for things other than short-term skeletal issues has barely been studied. From this, we may wish to keep an open mind, while also noting that it can hardly claim to be evidence-based—and it’s had hundreds of years to accumulate evidence. In all likelihood, publication bias has meant that studies that were conducted and found inconclusive or negative results were simply not published—but that’s just a hypothesis on our part.
In the case of using chiropractic to treat migraines, a very-related-but-not-skeletal issue, researchers found:
❝Pre-specified feasibility criteria were not met, but deficits were remediable. Preliminary data support a definitive trial of MCC+ for migraine.❞
Translating this: “it didn’t score as well as we hoped, but we can do better. We got some positive results, and would like to do another, bigger, better trial; please fund it”
Source: Multimodal chiropractic care for migraine: A pilot randomized controlled trial
Meanwhile, chiropractors’ claims for very unrelated things have been harshly criticized by the scientific community, for example:
Misinformation, chiropractic, and the COVID-19 pandemic
About that “short-term” aspect, one of our subscribers put it quite succinctly:
❝Often a skeletal correction is required for initial alignment but the surrounding fascia and muscles also need to be treated to mobilize the joint and release deep tissue damage surrounding the area. In combination with other therapies chiropractic support is beneficial.❞
This is, by the way, very consistent with what was said in the very clinically-dense book we reviewed yesterday, which has a chapter on the short-term benefits and limitations of chiropractic.
A truism that holds for many musculoskeletal healthcare matters, holds true here too:
❝In a battle between muscle and bone, muscle will always win❞
In other words…
Chiropractic can definitely help put misaligned bones back where they should be. However, once they’re there, if the cause of their misalignment is not treated, they will just re-misalign themselves shortly after you walking out of your session.
This is great for chiropractors, if it keeps you coming back for endless appointments, but it does little for your body beyond give you a brief respite.
So, by all means go to a chiropractor if you feel so inclined (and you do not fear accidental arterial dissection etc), but please also consider going to a physiotherapist, and potentially other medical professions depending on what seems to be wrong, to see about addressing the underlying cause.
Take care!
Share This Post
-

Tomatoes vs Carrots – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing tomatoes to carrots, we picked the carrots.
Why?
Both known for being vitamin-A heavyweights, there is nevertheless a clear winner:
In terms of macros, carrots have a little over 2x the carbs, and/but also a little over 2x the fiber, so we consider category this a win for carrots.
In the category of vitamins, tomatoes have more vitamin C, while carrots have more of vitamins A, B1, B2, B3, B5, B6, B9, E, K, and choline. And about that vitamin A specifically: carrots have over 20x the vitamin A of tomatoes. An easy win for carrots here!
When it comes to minerals, tomatoes have a little more copper, while carrots have more calcium, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc. Another clear win for carrots.
Looking at polyphenols, carrots are good but tomatoes have more, including a good healthy dose of quercetin; they also have more lycopene, not technically a polyphenol by virtue of its chemical structure (it’s a carotenoid), but a powerful phytochemical nonetheless (and much more prevalent in sun-dried tomatoes, in any case, which is not what we were looking at today—perhaps another day we’ll do sun-dried tomatoes and carrots head-to-head!).
Still, a) carrots are not short of carotenoids either (including lycopene), and b) we don’t think the moderate win on polyphenols is enough to outdo carrots having won all the other categories.
All in all, carrots win the day, but of course, do enjoy either or both; diversity is good!
Want to learn more?
You might like to read:
Lycopene’s Benefits For The Gut, Heart, Brain, & More
Enjoy!
Share This Post
-

Caffeine Blues – by Stephen Cherniske
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Caffeine use is an interesting and often-underexamined factor in health. Beyond the most superficial of sleep hygiene advice (à la “if you aren’t sleeping well, consider skipping your triple espresso martini at bedtime”), it’s often considered a “everybody has this” drug.
In this book, Cherniske explores a lot of the lesser-known effects of caffeine, and the book certainly is a litany against caffeine dependence, ultimately arguing strongly against caffeine use itself. The goal is certainly to persuade the reader to desist in caffeine use, and while the book’s selling point is “learn about caffeine” not “how to quit caffeine”, a program for quitting caffeine is nevertheless included.
You may notice the title and cover design are strongly reminiscent of “Sugar Blues”, which came decades before it, and that’s clearly not accidental. The style is similar—very sensationalist, and with a lot of strong claims. In this case, however, there is actually a more robust bibliography, albeit somewhat dated now as science has continued to progress since this book was published.
Bottom line: in this reviewer’s opinion, the book overstates its case a little, and is prone to undue sensationalism, but there is a lot of genuinely very good information in here too, making it definitely worth reading.
Share This Post
Related Posts
-
How to support a loved one with opioid use disorder
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Stacey Foley started using opioids while she was in an abusive relationship. When the relationship ended, her opioid use increased.
“I didn’t know how to work through the trauma,” Foley tells Public Good News. “I didn’t know how to handle my nervous system, and so opioids became my escape.”
Years later, after starting a new relationship and having two children, Foley recognized that her opioid use was affecting her parenting. She decided to make a change. Now, the Canadian speaker and writer has been in recovery from opioid use disorder for seven years.
Foley isn’t alone. After a doctor prescribed Lauren Wassum opioids to manage pain from an injury, she started using the medication to cope with the death of her uncle.
“I felt like the world was crashing around me. Really, it was that I just didn’t know how to deal with the grief,” Wassum says. Ten years later, after an overdose, she entered treatment. Now Wassum is a certified recovery specialist in Pennsylvania who helps others with substance use disorder live healthier lives.
Both Foley and Wassum say that support from others has been critical to their recovery.
“Every addiction is different. Every person is different. The best thing that you can really, truly do for someone is to be there to support them when they need it,” Foley says.
Read on to learn how you can support loved ones with OUD.
How does opioid addiction happen?
Taking opioids repeatedly, or differently than prescribed, can change how the brain works. The body may make fewer endorphins, chemicals that help regulate pain and stress. When people try to stop or reduce opioid use, they may experience withdrawal symptoms such as changes in body temperature, irritability, tremors, trouble sleeping, and intense cravings. This can make opioids hard to stop using and may lead to OUD.
OUD is a chronic health condition that can cause mental and physical distress. Because opioids can slow or stop breathing, OUD can also increase the risk of overdose and death. It can affect anyone at any stage of life.
“There’s no group that’s spared [from OUD],” Dr. Sarah S. Kawasaki, an addiction medicine specialist and associate professor at Penn State College of Medicine, explains.
What are signs that a loved one might be struggling with OUD?
OUD can cause physical symptoms like changes in pupil size, drowsiness, changes in appetite and weight, and flu-like symptoms. It can also show up in behavior, including pulling away from family, work, or daily responsibilities.
“Any addiction revolves around a pathologic craving,” Kawasaki says. “That craving leads to an inordinate amount of time spent thinking about how to earn money to get their next fix, how to achieve their next fix, how to avoid the negative symptoms of withdrawal. It’s doing so while neglecting family relationships, work relationships, financial obligations—at a great risk to personal freedom, to personal safety.”
James Sherman, a clinical research coordinator and lead substance use navigator at University of Pennsylvania’s Center for Addiction Medicine and Policy, is in recovery from OUD. He has firsthand experience with those behavioral changes.
“In my addiction, I often avoided interacting with my loved ones because I was fueled with so much guilt and shame due to my opioid use,” Sherman tells PGN. “In my drug use, work, family events, going to the doctor, adhering to my probation responsibilities—all of it went on the back burner.”
People with OUD might also show signs of emotional distress or mood changes.
“I think my husband always sort of had an inkling [that I was using opioids] because the high and low of opioids causes some pretty intense mood swings,” Foley says.
Seeing multiple health care providers for opioid prescriptions, or running out of medication early, can also be signs that someone may need help.
“If somebody has a prescription for opioids, but they find that they’re running out early, they need more and more, they’re frequenting emergency departments because they are running out of medicine and not feeling well and sometimes they use multiple prescribers—that is also a sign of addiction,” Kawasaki notes.
How can I support a loved one who’s living with OUD or in recovery?
Stay open and nonjudgmental.
Shame can keep people from seeking treatment or staying in recovery. A nonjudgmental approach can help loved ones with OUD make healthier choices.
“Sympathize with the person by focusing on concern rather than criticism,” Sherman says. “Emphasizing that ‘I care about you….’ rather than, ‘How could you do this?’”
Wassum’s partner modeled that approach when she sought treatment.
“When my overdose happened, he was like, ‘I will be here every step of the way. I know you can do this. I know you’re a good mom.’ Having that support makes a big difference,” she says.
Words and person-first language matter, too.
“Changing our language is really important—not calling someone an addict, a junkie, etc.,” Sherman says. “This is a person with a use disorder. This is someone you want to get better, instead of putting so much blame [on them].”
Check in regularly.
People living with OUD or in recovery may pull back from others, even when connection could help. Foley says regular phone calls, texts, and invitations can make a difference.
“[Support] really is about making sure that that person in your life knows that you’re there, that you’re checking on them, and that you’re supporting them because there are going to be so many days when temptation comes to use again,” she says.
Be patient.
A loved one may not be ready to seek help right away.
“When people try to push you into treatment and you’re not ready, that’s one of the hardest things,” Wassum says. “It’s almost like you feel like you have to go just to make them happy, and then you end up leaving or making it worse [for yourself] down the line.”
Being encouraging—rather than demanding—can help loved ones feel supported.
“I have found that using ‘we’ statements helps make loved ones feel like they’re not in this alone—‘We should schedule you an appointment,’ ‘We should try and get you into treatment,’” Sherman says.
When they’re ready, help them find treatment that fits their needs.
Treatment for OUD looks different from person to person. It may include counseling, peer support, in-patient treatment, or medication that helps people stop or reduce opioid use. Learning about and supporting a loved one’s treatment plan can help them stay in recovery.“All too often, the treatments for opioid use disorder are equally as stigmatized as the illness of opioid use disorder, and that can be lethal,” Kawasaki says.
Medication for opioid use disorder is often misunderstood as “trading” one addiction for another. That’s not the case.
“You can think of [MOUD] in terms of any medication that you need to control a chronic illness. If you have high blood pressure, if you have diabetes, if you have HIV, if you need to take medicine to suppress an illness that can cause catastrophic outcomes, you depend on that medicine,” Kawasaki explains. “If you stopped any one of those medicines, eventually, you would need to be seen in the emergency department with complications from those issues. Similarly, that’s the case with [MOUD].”
Find treatment resources by contacting SAMHSA’s National Helpline (1-800-662-HELP) or talking to a health care provider.
This article first appeared on Public Good News and is republished here under a Creative Commons Attribution-NoDerivatives 4.0 International License.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
The first night effect: why it’s hard to sleep when you’re somewhere new
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s nighttime and you’re exhausted. But the hotel bed feels wrong. The mini fridge won’t stop making that low, irritating hum. The power outlet lights feel brighter than the sun. Outside, random car honks and noises make sleep feel like a distant possibility.
Many of us struggle to sleep in new environments, even when we’re physically tired. But why? The short answer: a mix of biology and psychology.

Vitaly Gariev/Unsplash Broken routines and missing sleep cues
Your brain is wired for predictability, especially at night, during our most vulnerable behaviour: sleep.
A combination of internal and external cues work together to create the right conditions for rest.
Internally, your body signals that it’s time to sleep by decreasing core body temperature and increasing the sleep-promoting hormone melatonin. This makes you less alert.
Externally, your environment needs to support these signals, not compete with it. At home, your typical pre-sleep wind-down habits and familiar surroundings tell your body it is safe to sleep.
But sleeping somewhere new often disrupts these sights, sounds and sensations your body relies on.
There may be different light levels (for example, from hotel room clocks or street lights), unfamiliar noises (such as elevators, traffic and neighbours) and different bedding (for instance, a firmer mattress or softer pillows).
And you may be doing different activities, such as eating out late or working on a laptop on your bed.
An alert brain in a new place
From an evolutionary perspective, lighter sleep or more frequent awakenings when we’re somewhere new may be protective, allowing us to detect potential threats more quickly and respond to danger.
This is known as the “first-night effect”. It means when we sleep somewhere new, our brains don’t fully switch off.
Brain activity recordings have shown that during the first night in a new environment, the left side of the brain remains more responsive to unfamiliar sounds, even during deep sleep, compared to the second night. Once we become familiar with the space, this vigilance usually fades.
But even when we start to get used to a new environment, other factors can still interfere with our sleep.
Stress, travel and emotions
Sleeping in a new environment can also be stressful.
Your brain may be running through logistics and to-do lists, thinking about your early flight, or scenarios where you forget important belongings. Maybe you’re also experiencing jet lag.
Emotions such as homesickness, excitement, anticipation or anxiety can disrupt sleep as well. Even positive stress – for example, feeling excited about a big trip – activates the same arousal systems in the brain as negative stress. The brain doesn’t distinguish why those systems are switched on.
Unfortunately, a heightened arousal system and sleep are competitors. When your stress response is active, it directly interferes with the brain’s ability to disengage and transition into sleep, even when you’re physically exhausted.
But some people actually sleep better away from home
For some of us, being away from home can actually remove everyday distractions: there are no household responsibilities, no unfinished tasks competing for attention, and clearer boundaries between “work time” and “rest time”.
The change of environment may also reduce bedtime rumination, which is often triggered by familiar home environments tied to stress, deadlines or to-do lists.
Better sleep when we are away may be to do with the amount of sleep we usually get at home. Research shows that individuals who are not getting enough sleep at home are likely to get better sleep when travelling.
If your sleep improves when you’re away, it might be an opportunity to consider how stimulating or busy your usual sleep environment has become – and what you can do to make it calmer.
Tips for sweet dreams at home or away
Reassure yourself. If you have a rough night of sleep in a new place it doesn’t mean something is “wrong” with you. It’s a normal, protective response from a brain that’s tuned to safety and familiarity. You might need a night or two to settle in.
Choose sleep-friendly accommodation when you can. Many hotels are deliberately designed to support good sleep and these features, such as pillow menus, melatonin-rich foods on the room-service menu, or even a personal sleep butler, can make a real difference.
Plan for a slower first day. If you know you’re sleeping somewhere new, expect that the first night might not be your best. Where possible, avoid scheduling demanding tasks the next morning and give yourself time to adjust.
Pack your sleep routine in your suitcase. Just as parents might do for their small child, pack your sleep routine with you. If you have a particular pillow case or a sleep mask, or a certain scent that helps you sleep at home, try bringing these with you so your brain has some familiar cues in an unfamiliar environment.
If you notice you sleep better away from home, take a look at your home sleep routine and environment. Keep your room cool and dark and make your bed comfortable with supportive pillows and fresh bedding. Establish a relaxing wind-down routine: dim lights and limit screens in the evening, and stick to consistent bed and wake times, even on weekends.
Charlotte Gupta, Sleep Researcher, Appleton Institute, HealthWise Research Group, CQUniversity Australia and Dayna Easton, Postdoctoral Research Fellow, College of Medicine and Public Health, Flinders University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Apricots vs Blueberries – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing apricots to blueberries, we picked the apricots.
Why?
Both have their merits!
In terms of macros, apricots have about 2x the protein (but it’s not a lot) while blueberries have very slightly more fiber and carbs. Ultimately we’re calling this category a tie, but it could be swung one way or the other if you have strong feelings about prioritizing things.
In the category of vitamins, apricots have more of vitamins A, B3, B5, B7, B9, C, and E, while blueberries have more of vitamins B1, K, and choline. A clear win for apricots here, even before considering the huge margin of difference on vitamin A (apricots having 32x the amount that blueberries do).
When it comes to minerals, apricots have more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, and zinc, while blueberries have more manganese. Another win for apricots.
Looking at phytochemicals, apricots have some cancer-killing properties, while blueberries have more polyphenols in total. Pros and cons to each, here. We’re going to call this category a tie, but as with the macros, an argument could be made for either fruit.
Adding up the sections gives us an overall win for apricots, but it’s close, and blueberries are certainly great too, so by all means enjoy either or both!
Want to learn more?
You might like:
Top 8 Fruits That Prevent & Kill Cancer
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:



