Pine Nuts vs Peanuts – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing pine nuts to peanuts, we picked the pine nuts.
Why?
An argument could be made for either, honestly, as it depends on what we prioritize the most. These are both very high-calorie foods, and/but are far from empty calories, as they both contain main nutrients. Obviously, if you are allergic to nuts, this one is just not a comparison for you, sorry.
Looking at the macros first, peanuts are higher in protein, carbs, and fiber, while pine nuts are higher in fats—though the fats are healthy, being mostly polyunsaturated, with about a third of the total fats monounsaturated, and a low amount of saturated fat (peanuts have nearly 2x the saturated fat). On balance, we’ll call the macros category a moderate win for peanuts, though.
In terms of vitamins, peanuts have more of vitamins B1, B3, B5, B6, and B9, while pine nuts have more of vitamins A, B2, C, E, K, and choline. All in all, a marginal win for pine nuts.
In the category of minerals, peanuts have more calcium and selenium, while pine nuts have more copper, iron, magnesium, manganese, phosphorus, and zinc. An easy win for pine nuts, even before we take into account that peanuts have nearly 10x as much sodium. And yes, we are talking about the raw nuts, not nuts that have been roasted and salted.
Adding up the categories gives a win for pine nuts—but if you have certain particular priorities, you might still prefer peanuts for the areas in which peanuts are stronger.
Of course, the best solution is to enjoy both!
Want to learn more?
You might like to read:
Why You Should Diversify Your Nuts!
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Not-So-Sweet Science Of Sugar Addiction

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
One
LumpMechanism Of Addiction Or Two?
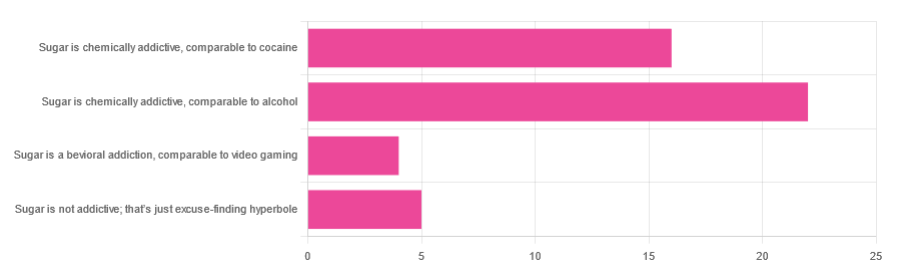
In Tuesday’s newsletter, we asked you to what extent, if any, you believe sugar is addictive; we got the above-depicted, below-described, set of responses:
- About 47% said “Sugar is chemically addictive, comparable to alcohol”
- About 34% said “Sugar is chemically addictive, comparable to cocaine”
- About 11% said “Sugar is not addictive; that’s just excuse-finding hyperbole”
- About 9% said “Sugar is a behavioral addiction, comparable to video gaming”
So what does the science say?
Sugar is not addictive; that’s just excuse-finding hyperbole: True or False?
False, by broad scientific consensus. As ever, the devil’s in the
detailsdefinitions, but while there is still discussion about how best to categorize the addiction, the scientific consensus as a whole is generally: sugar is addictive.That doesn’t mean scientists* are a hive mind, and so there will be some who disagree, but most papers these days are looking into the “hows” and “whys” and “whats” of sugar addiction, not the “whether”.
*who are also, let us remember, a diverse group including chemists, neurobiologists, psychologists, social psychologists, and others, often collaborating in multidisciplinary teams, each with their own focus of research.
Here’s what the Center of Alcohol and Substance Use Studies has to say, for example:
Sugar Addiction: More Serious Than You Think
Sugar is a chemical addiction, comparable to alcohol: True or False?
True, broadly, with caveats—for this one, the crux lies in “comparable to”, because the neurology of the addiction is similar, even if many aspects of it chemically are not.
In both cases, sugar triggers the release of dopamine while also (albeit for different chemical reasons) having a “downer” effect (sugar triggers the release of opioids as well as dopamine).
Notably, the sociology and psychology of alcohol and sugar addictions are also similar (both addictions are common throughout different socioeconomic strata as a coping mechanism seeking an escape from emotional pain).
See for example in the Journal of Psychoactive Drugs:
On the other hand, withdrawal symptoms from heavy long-term alcohol abuse can kill, while withdrawal symptoms from sugar are very much milder. So there’s also room to argue that they’re not comparable on those grounds.
Sugar is a chemical addiction, comparable to cocaine: True or False?
False, broadly. There are overlaps! For example, sugar drives impulsivity to seek more of the substance, and leads to changes in neurobiological brain function which alter emotional states and subsequent behaviours:
The impact of sugar consumption on stress driven, emotional and addictive behaviors
However!
Cocaine triggers a release of dopamine (as does sugar), but cocaine also acts directly on our brain’s ability to remove dopamine, serotonin, and norepinephrine:
The Neurobiology of Cocaine Addiction
…meaning that in terms of comparability, they (to use a metaphor now, not meaning this literally) both give you a warm feeling, but sugar does it by turning up the heating a bit whereas cocaine does it by locking the doors and burning down the house. That’s quite a difference!
Sugar is a behavioral addiction, comparable to video gaming: True or False?
True, with the caveat that this a “yes and” situation.
There are behavioral aspects of sugar addiction that can reasonably be compared to those of video gaming, e.g. compulsion loops, always the promise of more (without limiting factors such as overdosing), anxiety when the addictive element is not accessible for some reason, reduction of dopaminergic sensitivity leading to a craving for more, etc. Note that the last is mentioning a chemical but the mechanism itself is still behavioral, not chemical per se.
So, yes, it’s a behavioral addiction [and also arguably chemical in the manners we’ve described earlier in this article].
For science for this, we refer you back to:
The impact of sugar consumption on stress driven, emotional and addictive behaviors
Want more?
You might want to check out:
Beating Food Addictions: When It’s More Than “Just” Cravings
Take care!
Share This Post
-

Orange vs Watermelon – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing orange to watermelon, we picked the orange.
Why?
In terms of macros, oranges have nearly 5x the fiber for only slightly more carbs. Now, the glycemic load of watermelon is still low (that’s a good thing), so that’s not a bad point for watermelon, but it does mean that oranges win this round easily by the numbers.
In the category of vitamins, oranges have more of vitamins B1, B2, B3, B5, B6, B9, C, E, and choline, while watermelon has more of vitamins A and K. Another win for oranges!
When it comes to minerals, oranges have more calcium, phosphorus, potassium, and selenium, while watermelon has more iron, manganese, and zinc. A more modest 4:3 win this time for oranges.
Adding up the sections makes for a clear overall win for oranges, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
From Apples to Bees, and High-Fructose Cs: Which Sugars Are Healthier, And Which Are Just The Same?
Enjoy!
Share This Post
-
Does masturbating really help menopause symptoms? New research says yes
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
About one in ten perimenopausal or menopausal women masturbate to relieve their symptoms, according to a study that has generated media interest around the world.
The attention is likely because masturbation is a novel (and possibly somewhat salacious) strategy to ease these symptoms, and older women are often seen as asexual.
So does masturbating really relieve symptoms, as the study published in the journal Menopause suggests? Let’s see if the evidence stacks up.

Deon Black/Pexels The health benefits of masturbation
The study was conducted in the United States and was led by researchers at the Kinsey Institute at Indiana University, one of the world’s best known research institutes that specialises in sex and relationships. The study was funded by sex toy company Womanizer.
Researchers surveyed a representative sample of 1,178 perimenopausal and menopausal women aged 40–65.
Women who reported changes in their periods but still had at least one period in the previous year were categorised as perimenopausal. Women who said they had not had a period in a year or longer were categorised as menopausal.
About four in five of the women said they had ever masturbated. Of those, about 20% said masturbating relieved their symptoms to some degree.
For perimenopausal women, the most improved symptoms were sleep difficulties and irritability. For a small number of menopausal women, it helped most with vaginal pain, bloating and painful urination.
The findings are consistent with previous research showing masturbating to orgasm may help reduce anxiety and psychological distress, improve sleep and reduce vaginal pain.
However, research on the health, social or relationship benefits of masturbation, including for menopause relief, is sparse.
In particular, we cannot be sure exactly how masturbating might improve symptoms. But researchers propose the relaxation effects of orgasm, and the release of endorphins, can improve mood, help sleep and reduce pain. Sexual stimulation may also induce vaginal lubrication and blood flow to the genital area, which can help maintain vaginal function.
A small number of women in the study said masturbating worsened their symptoms, although it was unclear why.
There’s still stigma around masturbation
Masturbation is mostly no longer regarded as sinful or dangerous. But it still carries a level of stigma.
Women, in particular, often associate masturbation with sexual shame and tend not to talk openly about their masturbation habits.
So the stigma and invisibility of masturbation means it is rarely the subject of clinical research investigating its benefits.
As a result, we have very little evidence on its effectiveness to relieve menopause symptoms, especially compared to other non-medical interventions such as physical activity or stress relief.
The US study showed women were substantially more likely to manage menopause symptoms through evidence-based strategies of physical activity, diet or stress reduction, than with masturbation.
However, many women in the study might have never considered masturbation to relieve their symptoms.
Masturbation isn’t for everyone
Masturbation is free, relatively easy and, for most women, enjoyable. There is no reason why it should not be promoted as an accessible menopause relief strategy that may benefit some women. However, it is not always so simple. There may be barriers for some women.
Not all women masturbate or enjoy masturbation. The US study showed nearly one in five women surveyed had never masturbated. This number was higher among older, menopausal women, perhaps reflecting generational change in attitudes about masturbation. Some women in the study indicated a moral or religious resistance to masturbation.
Other studies have similarly shown that a number of women do not masturbate. There may be many reasons for this, from lack of desire through to limited privacy or “alone time”. Older women may experience complex physical barriers, including loss of libido or limited dexterity and flexibility.
Silence and stigma around masturbation may also make it difficult for health professionals to discuss masturbation with women. This was evident in the US study, with almost all reporting they had never spoken to a doctor about masturbation for any reason.
Many women were open to these conversations, however, with about 56% of perimenopausal women indicating they would masturbate more often to treat menopause symptoms if their doctor recommended it.
Masturbation as a novel strategy
Although there can be no guarantee masturbation will relieve menopause symptoms for all women, suggesting women give it a go is unlikely to cause harm. It is the safest sex available.
We don’t talk much about masturbation, especially among older women. But by demonstrating that most older women do masturbate and this may offer health benefits, this latest study is novel and valuable.
Jennifer Power, Principal Research Fellow, Australian Research Centre in Sex, Health and Society, La Trobe University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post




Related Posts
-
Demystifying Peptides
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small 😎
❝Would love some in depth look at peptides. Benefits, side effects of several of the popular ones❞
Great question! It’s a huge topic that can easily be confusing, but not if we break it down a bit.
Which, as you’ll see, is what peptides are all about:
Breaking it down
In a nutshell: peptides are short chains of amino acids—smaller than proteins—that do a variety of things for us, perhaps most noteably including:
- act as chemical messengers within the body*
- act as the building blocks of larger proteins (the general stuff that most of our body is made of)**
*If that first one sounds familiar and you’re thinking “you mean hormones?”, then you’re on the right track, and indeed there’s an overlap, because there are such things as peptide hormones, for example:
❝Peptide hormones play a prominent role in controlling energy homeostasis and metabolism. They have been implicated in controlling appetite, the function of the gastrointestinal and cardiovascular systems, energy expenditure, and reproduction. Furthermore, there is growing evidence indicating that peptide hormones and their receptors contribute to energy homeostasis regulation by interacting with white and brown adipose tissue.❞
Read in full: The Role of Peptide Hormones Discovered in the 21st Century in the Regulation of Adipose Tissue Functions
And about that brown adipose tissue (BAT), this is very important to understand: The BAT-pause! When Cold Weather & The Menopause Battle It Out
**As for these building blocks, then here there are two important things to know about:
- Why You Can’t Skimp On Amino Acids ← when it comes to essential amino acids, the ill effects of deficiency can range from “muscle atrophy” to “brain stops working” and “bones fall apart” and more. In short, any essential amino acid deficiency not remedied will ultimately result in death; we literally become non-viable as organisms without these 9 things.
- We Are Such Stuff As Fish Are Made Of ← this is about collagen, which brings us to collagen peptides next.
A common question about collagen is whether the molecules can actually be absorbed. And the answer is, broadly speaking “not without being broken down first”.
This is because collagen molecules are absolutely huge (as molecules go) and cannot be absorbed by the skin. Not only that, but the epidermis (the outer part of your skin) is not where collagen synthesis happens, so this is a bit like trying to fix a structural problem in your house by flinging mud at it from the outside. The mud may have the same minerals that are needed, but it’s just going to sit on the outside of your house until it gets washed off.
Collagen molecules are also too large to be absorbed by the gut, too. So, for both cases, collagen peptides are the answer. This is what is meant when a product says “hydrolysed collagen” or “collagen peptides” or perhaps “hydrolysed collagen peptides” to cover all bases, but really that is a redundant tautology repeated more than once unnecessarily—it refers to the same thing: collagen that has been broken down into bits (peptides) for ease of absorption.
You can read about this in full, here: Are Collagen Molecules Too Big To Be Absorbed?
You also asked for several of the popular ones, so in terms of benefits (and how backed those benefits are by scientific evidence), and side effects:
- Collagen peptides: support skin elasticity and joint health; evidence moderate but growing, and to our eyes, it looks promising.
- See also: 16 Ways To Boost Collagen, for more ways than just supplementing
- Creatine or BPC-157: tissue repair and inflammation control; most data from non-human animals, limited clinical trials, astonishingly.
- See also: Creatine: Very Different For Young & Old People ← younger people get more muscle benefits, older people get more brain benefits
- Melanotan II: stimulates tanning; can cause nausea, blood-pressure spikes, and pigment changes. Generally a terrible idea, and we certainly do not recommend it.
- GLP-1 mimetics (e.g., semaglutide): originally for diabetes, now known for weight loss; strong clinical evidence but really does need medical supervision, and has a long list of potential (and even, probable) side effects
- Thymosin beta-4 and GHK-Cu: wound healing and hair growth claims; evidence early-stage or cosmetic only.
- We haven’t done a main feature yet, in part for that precise reason—the paucity of evidence. But, we’ll see what we can find, so watch this space for a main feature coming soon!
There are also other kinds of peptides relevant for health (and beauty, which is after all in large part a factor of health) too, including:
- Carrier peptides: deliver metals like copper or manganese to aid repair.
- Enzyme-inhibiting peptides: slow down collagen/elastin breakdown (e.g. tripeptide-1).
- Neurotransmitter-inhibiting peptides: reduce muscle activity to soften expression lines (e.g. argireline/acetyl hexapeptide-8).
- Specialty peptides: target brightening (e.g. hexapeptide-2) or barrier repair.
However, not all of them actually have a lot of evidence for helping. When it comes to skincare specifically, one of the dermatologists we feature sometimes recommends these ones as being “worth the hype”:
- Signal peptides like matrixyl: tried-and-true for firmness and plumpness.
- Copper peptides: aid repair and overall skin health.
- Argireline: softer alternative to Botox for fine lines.
- Hexapeptide-2: gentle brightening when paired with vitamin C.
You can learn about why, here: Not All Peptides Are Equal (So, Which Are Worth the Hype?)
Do be aware also that with almost any of these there are other potential (but much less common) risks, including allergic reactions, hormonal disruption, infection from injections, and unknown long-term effects for most things that haven’t been studied nearly enough yet.
If in doubt, speak with a dermatologist (or, if it’s not about skincare, speak with a relevant professional who can give you advice tailored to you), and know that it’s always better to err on the side of caution.
Want to learn more?
Check out:
What Really Works For Anti-Aging? Science-Backed Skincare Ingredients
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Erythritol & Brain Damage: Is The Science As Scary As It Sounds?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A couple of years ago, we examined some news about another sweetener: The Sucralose News: Scaremongering Or Serious?
…and the short version is that initial headlines are often not a completely honest representation of the truth (in the above case, the reality was “this doesn’t look good, but we need to do a lot more science to declare it with confidence”).
We wrote about that, too: How Science News Outlets Can Lie To You (Yes, Even If They Cite Studies!)
So, what’s the deal with erythritol?
Erythritol is a sugar alcohol, which so far as the body is concerned is neither sugar nor alcohol in the way those words are commonly understood; it’s just a chemical term. The sugar isn’t processed as such by the body and are passed as dietary fiber, and nor is there any intoxicating effect as one might expect from an alcohol. However, as it has a sweet taste, it can be used a sweetener.
This is general (sweetening things, no matter with what), can lead to a slippery slope of craving increasingly sweeter things, which is generally a bad idea.
See what the WHO had to say about that (and why), here: The Problem With Sweeteners
The WHO recommendation (avoid sweeteners) applied to artificial and naturally-occurring non-sugar sweeteners, such as:
- Acesulfame K
- Advantame
- Aspartame
- Cyclamates
- Neotame
- Saccharin
- Stevia
Erythritol (and sucralose, for that matter) didn’t make the list, because as they are technically sugars, they don’t go on a list of non-sugar sweeteners.
That said, around the same time a study did find that erythritol was linked to a higher risk of heart attack, stroke, and early death, so it was clear even then that it may not be an amazing sweetener either:
Read: The artificial sweetener erythritol and cardiovascular event risk
We further explored that in one of our “This or That” head-to heads: Xylitol vs Erythritol – Which is Healthier?
The answer we came to was:
❝The one thing that sets them apart is their respective safety profiles. Xylitol is prothrombotic and associated with major adverse cardiac events (CI=95, adjusted hazard ratio=1.57, range=1.12-2.21). Erythritol is also prothrombotic and more strongly associated with major adverse cardiac events (CI=95, adjusted hazard ratio=2.21, range=1.20-4.07).
So, xylitol is bad and erythritol is worse, which means the relatively “healthier” is xylitol. We don’t recommend either, though.❞
(we showed studies for this, linked in the “This or That” page here)
As a quick aside: readers with good memories may recall that we’ve sometimes recommended xylitol for good oral health (it’s not just “not too bad as sweeteners go”, it actively does good things too; the crux is that it’s being used in the mouth (such as with xylitol-sweetened gum) but not actually ingested in meaningful amounts.
You can learn more about that here: Xylitol: Cavity Fighter Or Gut Disruptor? The Dose Makes the Poison
Now, back to erythritol and the science of the day:
A team of researchers (Dr. Auburn Berry et al.) investigated the effects of erythritol directly on the brain.
This was prompted by the research we mentioned up above about the major adverse cardiac events, and others, showing higher blood erythritol levels to increased risk of heart attack or stroke within three years.
This study, however, was all about the brain. And when a moment ago we said “directly on the brain”, we do mean exactly that; this was an in vitro study, because it’s difficult to get live human volunteers to give the scientists permission to slice their brains into thin slices to look at them under the microscope, and while many advances have been made in scanning techniques and “liquid biopsies”, we’re not quite there yet for this kind of research.
What they found, in few words, was that exposing brain blood vessel cells to erythritol levels similar to a typical sugar-free drink caused:
- increased reactive oxygen species (which age and inflame tissues)
- reduced nitric oxide (leading to less vessel relaxation)
- increased endothelin-1 (causing more vessel constriction)
- impaired production of t-PA (reducing the ability to break down clots)
This all has important implications for stroke risk, since especially the combination of:
- narrower vessels,
- less clot-busting capability, and
- more cellular stress
…are all things that increase stroke risk. Alone, never mind together.
And together, they don’t just add up, but rather compound to make things even worse.
All that said, Dr. Berry herself does emphasize that the study was done on cells in petri dishes, that as such…
- while yes the findings do add to growing concern, and
- people are advised to read labels and limit intake of erythritol and similar sweeteners,
- it still cannot be said absolutely conclusively that the same things definitely happens in vivo (i.e. in live humans outside of the laboratory).
You can read the paper in full, here: The non-nutritive sweetener erythritol adversely affects brain microvascular endothelial cell function
Want to learn more?
Check out:
How To Reduce Your Stroke Risk ← 8 ways
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Foam Rolling – by Karina Inkster
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
If you’ve ever bought a foam roller only to place it under your lower back once and then put it somewhere for safekeeping and never use it again, this book will help fix that.
Karina Inkster (what a cool name) is a personal trainer, and the book also features tips and advice from physiotherapists and sports medicine specialist doctors too, so all bases are well and truly covered.
This is not, in case you’re wondering, a book that could have been a pamphlet, with photos of the exercises and one-liner explanation and that’s it. Rather, Inkster takes us through the anatomy and physiology of what’s going on, so that we can actually use this thing correctly and get actual noticeable improvements to our health from it—as promised in the subtitle’s mention of “for massage, injury prevention, and core strength”. To be clear, a lot of it is also about soft tissue mobilization, and keeping our fascia healthy (an oft-underestimated aspect of general mobility).
We would mention that since the photos are pleasantly colorful (like those on the cover) and this adds to the clarity, we’d recommend springing for the (quite inexpensive) physical copy, rather than a Kindle edition (if your e-reader is a monochrome e-ink device like this reviewer’s, anyway).
Bottom line: this book will enable your foam roller to make a difference to your life.
Click here to check out Foam Rolling, and get rolling (correctly)!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: