Make Your Negativity Work For You
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What’s The Right Balance?
We’ve written before about positivity the pitfalls and perils of toxic positivity:
How To Get Your Brain On A More Positive Track (Without Toxic Positivity)
…as well as the benefits that can be found from selectively opting out of complaining:
A Bone To Pick… Up And Then Put Back Where We Found It
So… What place, if any, does negativity usefully have in our lives?
Carrot and Stick
We tend to think of “carrot and stick” motivation being extrinsic, i.e. there is some authority figure offering is reward and/or punishment, in response to our reactions.
In those cases when it really is extrinsic, the “stick” can still work for most people, by the way! At least in the short term.
Because in the long term, people are more likely to rebel against a “stick” that they consider unjust, and/or enter a state of learned helplessness, per “I’ll never be good enough to satisfy this person” and give up trying to please them.
But what about when you have your own carrot and stick? What about when it comes to, for example, your own management of your own healthy practices?
Here it becomes a little different—and more effective. We’ll get to that, but first, bear with us for a touch more about extrinsic motivation, because here be science:
We will generally be swayed more easily by negative feelings than positive ones.
For example, a study was conducted as part of a blood donation drive, and:
- Group A was told that their donation could save a life
- Group B was told that their donation could prevent a death
The negative wording given to group B boosted donations severalfold:
Read the paper: Life or Death Decisions: Framing the Call for Help
We have, by the way, noticed a similar trend—when it comes to subject lines in our newsletters. We continually change things up to see if trends change (and also to avoid becoming boring), but as a rule, the response we get from subscribers is typically greater when a subject line is phrased negatively, e.g. “how to avoid this bad thing” rather than “how to have this good thing”.
How we can all apply this as individuals?
When we want to make a health change (or keep up a healthy practice we already have)…
- it’s good to note the benefits of that change/practice!
- it’s even better to note the negative consequences of not doing it
For example, if you want to overcome an addiction, you will do better for your self-reminders to be about the bad consequences of using, more than the good consequences of abstinence.
See also: How To Reduce Or Quit Alcohol
This goes even just for things like diet and exercise! Things like diet and exercise can seem much more low-stakes than substance abuse, but at the end of the day, they can add healthy years onto our lives, or take them off.
Because of this, it’s good to take time to remember, when you don’t feel like exercising or do feel like ordering that triple cheeseburger with fries, the bad outcomes that you are planning to avoid with good diet and exercise.
Imagine yourself going in for that quadruple bypass surgery, asking yourself whether the unhealthy lifestyle was worth it. Double down on the emotions; imagine your loved ones grieving your premature death.
Oof, that was hard-hitting
It was, but it’s effective—if you choose to do it. We’re not the boss of you! Either way, we’ll continue to send the same good health advice and tips and research and whatnot every day, with the same (usually!) cheery tone.
One last thing…
While it’s good to note the negative, in order to avoid the things that lead to it, it’s not so good to dwell on the negative.
So if you get caught in negative thought spirals or the like, it’s still good to get yourself out of those.
If you need a little help with that sometimes, check out these:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Teriyaki Chickpea Burgers

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Burgers are often not considered the healthiest food, but they can be! Ok, so the teriyaki sauce component itself isn’t the healthiest, but the rest of this recipe is, and with all the fiber this contains, it’s a net positive healthwise, even before considering the protein, vitamins, minerals, and assorted phytonutrients.
You will need
- 2 cans chickpeas, drained and rinsed (or 2 cups of chickpeas, cooked drained and rinsed)
- ¼ cup chickpea flour (also called gram flour or garbanzo bean flour)
- ¼ cup teriyaki sauce
- 2 tbsp almond butter (if allergic, substitute with a seed butter if available, or else just omit; do not substitute with actual butter—it will not work)
- ½ bulb garlic, minced
- 1 large chili, minced (your choice what kind, color, or even whether or multiply it)
- 1 large shallot, minced
- 1″ piece of ginger, grated
- 2 tsp teriyaki sauce (we’re listing this separately from the ¼ cup above as that’ll be used differently)
- 1 tsp yeast extract (even if you don’t like it; trust us, it’ll work—this writer doesn’t like it either but uses it regularly in recipes like these)
- 1 tbsp black pepper
- 1 tsp fennel powder
- ½ tsp sweet cinnamon
- ½ tsp MSG or 1 tsp low-sodium salt
- Extra virgin olive oil for frying
For serving:
- Burger buns (you can use our Delicious Quinoa Avocado Bread recipe)
- Whatever else you want in there; we recommend mung bean sprouts, red onion, and a nice coleslaw
Method
(we suggest you read everything at least once before doing anything)
1) Preheat the oven to 400℉ / 200℃.
2) Roast the chickpeas spaced out on a baking tray (lined with baking paper) for about 15 minutes. Leave the oven on afterwards; we still need it.
3) While that’s happening, heat a little oil in a skillet to a medium heat and fry the shallot, chili, garlic, and ginger, for about 2–3 minutes. You want to release the flavors, but not destroy them.
4) Let them cool, and when the chickpeas are done, let them cool for a few minutes too, before putting them all into a food processor along with the rest of the ingredients from the main section, except the oil and the ¼ cup teriyaki sauce. Process them into a dough.
5) Form the dough into patties; you should have enough dough for 4–6 patties depending on how big you want them.
6) Brush them with the teriyaki sauce; turn them onto a baking tray (lined with baking paper) and brush the other side too. Be generous.
7) Bake them for about 15 minutes, turn them (taking the opportunity to add more teriyaki sauce if it seems to merit it) and bake for another 5–10 minutes.
8) Assemble; we recommend the order: bun, a little coleslaw, burger, red onion, more coleslaw, mung bean sprouts, bun, but follow your heart!

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Three Daily Servings of Beans/Legumes?
- Hoisin Sauce vs Teriyaki Sauce – Which is Healthier?
- Sprout Your Seeds, Grains, Beans, Etc
- Our Top 5 Spices: How Much Is Enough For Benefits? ← we scored 4/5 today!
- Monosodium Glutamate: Sinless Flavor-Enhancer Or Terrible Health Risk?
Take care!
Share This Post
-

100 Hikes of a Lifetime – by Kate Siber
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This is published by National Geographic, so you can imagine the quality of the photos throughout.
Inside, and after a general introduction and guide to gear and packing appropriately, it’s divided into continents, with a diverse array of “trips of a lifetime” for anyone who enjoys hiking.
It’s not a narrative book, rather, it is a guide, a little in the style of “Lonely Planet”, with many “know before you go” tips, information about the best time to go, difficult level, alternative routes if you want to get most of the enjoyment while having an easier time of it (or, conversely, if you want to see some extra sights along the way), and what to expect at all points.
Where the book really excels is in balancing inspiration with information. There are some books that make you imagine being in a place, but you’ll never actually go there. There are other books that are technical manuals but not very encouraging. This one does both; it provides the motivation and the “yes, you really can, here’s how” information that, between them, can actually get you packing and on your way.
Bottom line: if you yearn for breathtaking views and time in the great outdoors, but aren’t sure where to start, this will give you an incredible menu to choose from, and give you the tools to go about doing it.
Click here to check out 100 Hikes Of A Lifetime, and live it!
Share This Post
-

Every Body Should Know This – by Dr. Federica Amati
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This book is very much a primer on how to eat healthily. The science is high-quality (the author is the head nutritionist at ZOE) and well-explained, and the advice is reasonable.
Limitations: this book is not very deep, which we might expect from a book with this title. So, if you’ve been a long-time 10almonds reader, you might not learn a lot here, and this book might make a better gift for someone else.
In particular, the book may be well-suited for someone who is thinking of having children soon, as there is an unusual amount of focus on fertility and young motherhood—perhaps because the author herself has young children and so was preoccupied with this when writing. For those of us who are definitely not having any more children, the focus on young motherhood is a little superfluous.
The writing style is very readable pop-science, and nobody who is able to read English is likely to struggle with this one. It’s also quite conversational in parts, as the author discusses her own experiences with implementing the science at hand.
Bottom line: if you want a good, solid, primer of how to eat well for a lifetime of health, especially if you are (or are thinking of becoming) a young mother, then this is a very good book. Otherwise, it’s probably a better to give it as a gift.
Click here to check out Every Body Should Know This, and know the things!
Share This Post

Related Posts
-
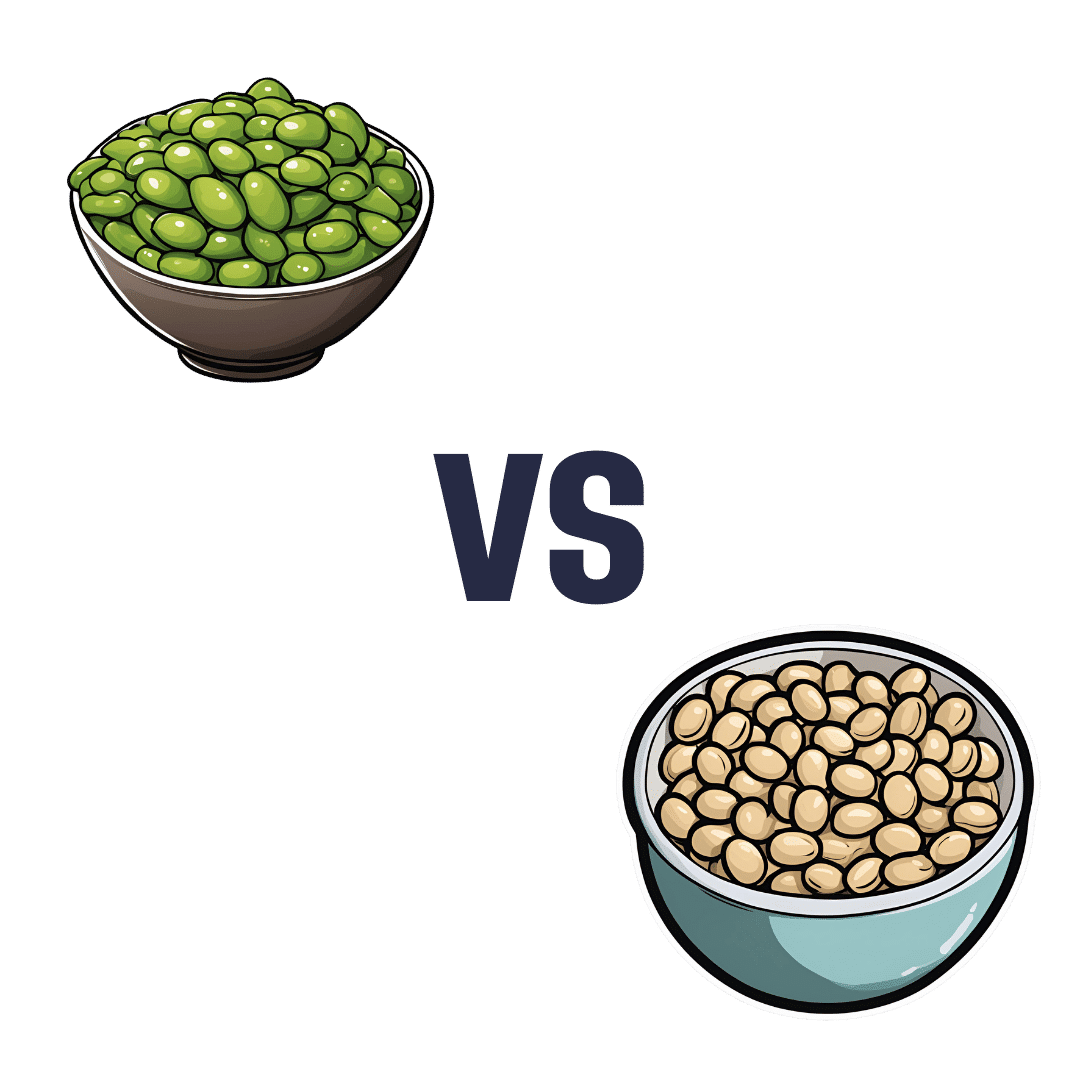
Edamame vs Soybeans – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing edamame to soybeans, we picked the soybeans.
Why?
You may be thinking: aren’t edamame soybeans? And yes, yes they are. But just like our many instances of pitting Brassica oleracea vs Brassica oleracea (one species, many cultivars e.g. broccoli, cauliflower, kale, cabbage, Brussels sprouts, etc), there are still differences. In this case, edamame and soybeans aren’t even different cultivars, what are conventionally called edamame are just the young beans of the plant, while what are conventionally called soybeans are the mature beans of the plant.
The main nutritional difference is: as they get older, they lose vitamins and gain minerals. More on that later. But first, “main difference” isn’t “only difference”, so…
In terms of macros, edamame have more carbs, while soybeans have a little more fiber and a lot more protein. An easy win for the mature soybeans.
In the category of vitamins, edamame have more of vitamins A, B1, B3, B5, B9, C, E, K, and choline, while soybeans have more of vitamins B2 and B6. A clear win for edamame, this time.
When it comes to minerals, the nutritional tables are turned, and edamame have more manganese and zinc, while soybeans have more calcium, copper, iron, magnesium, phosphorus, potassium, and selenium. An easy win for soybeans.
Adding up the sections makes for a two-to-one victory for soybeans, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like to read:
What’s Your Plant Diversity Score?
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Brain Maker – by Dr. David Perlmutter
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Regular 10almonds readers probably know about the gut-brain connection already, so what’s new here?
Dr. David Perlmutter takes us on a tour of gut and brain health, specifically, the neuroprotective effect of healthy gut microbiota.
This seems unlikely! After all, vagus nerve or no, the gut microbiota are confined to the gut, and the brain is kept behind the blood-brain barrier. So how does one thing protect the other?
Dr. Perlmutter presents the relevant science, and the honest answer is, we’re not 100% sure how this happens! We do know part of it: that bad gut microbiota can result in a “leaky gut”, and that may in turn lead to such a thing as a “leaky brain”, where the blood-brain barrier has been compromised and some bad things can get in with the blood.
When it comes to gut-brain health…
Not only is the correlation very strong, but also, in tests where someone’s gut microbiota underwent a radical change, e.g. due to…
- antibiotics (bad)
- fasting (good)
- or a change in diet (either way)
…their brain health changed accordingly—something we can’t easily check outside of a lab, but was pretty clear in those tests.
We’re also treated to an exposé on the links between gut health, brain health, inflammation, and dementia… Which links are extensive.
In closing, we’ll mention that throughout this book we’re also given many tips and advices to improve our gut/brain health, reverse damage done already, and set ourselves up well for the future.
Click here to check out “Brain Maker” on Amazon and take care of this important part of your health!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
New Year, New Health Habits?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s that time of the year, and many of us hope to make this our healthiest year yet—or at least significantly improve it in some particular area that’s important to us! So, what news from the health world?
The rise of GLP-1 agonists continues
GLP-1 agonists have surged in popularity in the past year, and it looks like that trend is set to continue in the new one. The title of the below-linked pop-science article is slightly misleading, it’s not “almost three quarters of UK women”, but rather, “72% of the women using the digital weight loss platform Juniper”, which means the sample is confined to people interested in weight loss. Still, of those interested in weight loss, 72% is a lot, and the sample size was over 1000:
Read in full: New Year, new approach to weight loss: Almost three quarters of UK women are considering using GLP-1s in 2025
Related: 5 ways to naturally boost the “Ozempic Effect” ← these natural methods “hack” the same metabolic pathways as GLP-1 agonists do (it has to do with incretin levels), causing similar results
The lesser of two evils
Smoking is terrible, for everything. Vaping is… Not great, honestly, but as the below-discussed study shows, at the very least it results in much less severe respiratory symptoms than actual smoking. For many, vaping is a halfway-house to actually quitting; for some, it’s just harm reduction, and that too can be worthwhile.
We imagine that probably very few 10almonds readers smoke cigarettes, but we know quite a few use cannabis, which is discussed also:
Read in full: Switching to e-cigarettes may ease respiratory symptoms, offering hope for smokers
Related: Vaping: A Lot Of Hot Air? ← we look at the pros, cons, and popular beliefs that were true a little while ago but now they’re largely not (because of regulatory changes re what’s allowed in vapes)
Sometimes, more is more
The below-linked pop-science article has a potentially confusingly-worded title that makes it sound like increased exercise duration results in decreasing marginal returns (i.e., after a certain point, you’re getting very limited extra benefits), but in fact the study says the opposite.
Rather, increased moderate exercise (so, walking etc) results in a commensurately decreasing weight and a decreasing waistline.
In short: walk more, lose more (pounds and inches). The study examined those who moved their bodies for 150–300 minutes per week:
Read in full: Increased exercise duration linked to decreasing results in weight and waistline
Related: The Doctor Who Wants Us To Exercise Less, & Move More
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: