Menopause can bring increased cholesterol levels and other heart risks. Here’s why and what to do about it
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Menopause is a natural biological process that marks the end of a woman’s reproductive years, typically between 45 and 55. As women approach or experience menopause, common “change of life” concerns include hot flushes, sweats and mood swings, brain fog and fatigue.
But many women may not be aware of the long-term effects of menopause on the heart and blood vessels that make up the cardiovascular system. Heart disease accounts for 35% of deaths in women each year – more than all cancers combined.
What should women – and their doctors – know about these risks?
Hormones protect hearts – until they don’t
As early as 1976, the Framingham Heart Study reported more than twice the rates of cardiovascular events in postmenopausal than pre-menopausal women of the same age. Early menopause (younger than age 40) also increases heart risk.
Before menopause, women tend to be protected by their circulating hormones: oestrogen, to a lesser extent progesterone and low levels of testosterone.
These sex hormones help to relax and dilate blood vessels, reduce inflammation and improve lipid (cholesterol) levels. From the mid-40s, a decline in these hormone levels can contribute to unfavourable changes in cholesterol levels, blood pressure and weight gain – all risk factors for heart disease.

4 ways hormone changes impact heart risk
1. Dyslipidaemia– Menopause often involves atherogenic changes – an unhealthy imbalance of lipids in the blood, with higher levels of total cholesterol, triglycerides, and low-density lipoprotein (LDL-C), dubbed the “bad” cholesterol. There are also reduced levels of high-density lipoprotein (HDL-C) – the “good” cholesterol that helps remove LDL-C from blood. These changes are a major risk factor for heart attack or stroke.
2. Hypertension – Declines in oestrogen and progesterone levels during menopause contribute to narrowing of the large blood vessels on the heart’s surface, arterial stiffness and raise blood pressure.
3. Weight gain – Females are born with one to two million eggs, which develop in follicles. By the time they stop ovulating in midlife, fewer than 1,000 remain. This depletion progressively changes fat distribution and storage, from the hips to the waist and abdomen. Increased waist circumference (greater than 80–88 cm) has been reported to contribute to heart risk – though it is not the only factor to consider.
4. Comorbidities – Changes in body composition, sex hormone decline, increased food consumption, weight gain and sedentary lifestyles impair the body’s ability to effectively use insulin. This increases the risk of developing metabolic syndromes such as type 2 diabetes.
While risk factors apply to both genders, hypertension, smoking, obesity and type 2 diabetes confer a greater relative risk for heart disease in women.
So, what can women do?
Every woman has a different level of baseline cardiovascular and metabolic risk pre-menopause. This is based on their genetics and family history, diet, and lifestyle. But all women can reduce their post-menopause heart risk with:
- regular moderate intensity exercise such as brisk walking, pushing a lawn mower, riding a bike or water aerobics for 30 minutes, four or five times every week
- a healthy heart diet with smaller portion sizes (try using a smaller plate or bowl) and more low-calorie, nutrient-rich foods such as vegetables, fruit and whole grains
- plant sterols (unrefined vegetable oil spreads, nuts, seeds and grains) each day. A review of 14 clinical trials found plant sterols, at doses of at least 2 grams a day, produced an average reduction in serum LDL-C (bad cholesterol) of about 9–14%. This could reduce the risk of heart disease by 25% in two years
- less unhealthy (saturated or trans) fats and more low-fat protein sources (lean meat, poultry, fish – especially oily fish high in omega-3 fatty acids), legumes and low-fat dairy
- less high-calorie, high-sodium foods such as processed or fast foods
- a reduction or cessation of smoking (nicotine or cannabis) and alcohol
- weight-gain management or prevention.

What about hormone therapy medications?
Hormone therapy remains the most effective means of managing hot flushes and night sweats and is beneficial for slowing the loss of bone mineral density.
The decision to recommend oestrogen alone or a combination of oestrogen plus progesterone hormone therapy depends on whether a woman has had a hysterectomy or not. The choice also depends on whether the hormone therapy benefit outweighs the woman’s disease risks. Where symptoms are bothersome, hormone therapy has favourable or neutral effects on coronary heart disease risk and medication risks are low for healthy women younger than 60 or within ten years of menopause.
Depending on the level of stroke or heart risk and the response to lifestyle strategies, some women may also require medication management to control high blood pressure or elevated cholesterol levels. Up until the early 2000s, women were underrepresented in most outcome trials with lipid-lowering medicines.
The Cholesterol Treatment Trialists’ Collaboration analysed 27 clinical trials of statins (medications commonly prescribed to lower cholesterol) with a total of 174,000 participants, of whom 27% were women. Statins were about as effective in women and men who had similar risk of heart disease in preventing events such as stroke and heart attack.
Every woman approaching menopause should ask their GP for a 20-minute Heart Health Check to help better understand their risk of a heart attack or stroke and get tailored strategies to reduce it.
Treasure McGuire, Assistant Director of Pharmacy, Mater Health SEQ in conjoint appointment as Associate Professor of Pharmacology, Bond University and as Associate Professor (Clinical), The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Pasteurization: What It Does And Doesn’t Do

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Pasteurization’s Effect On Risks & Nutrients

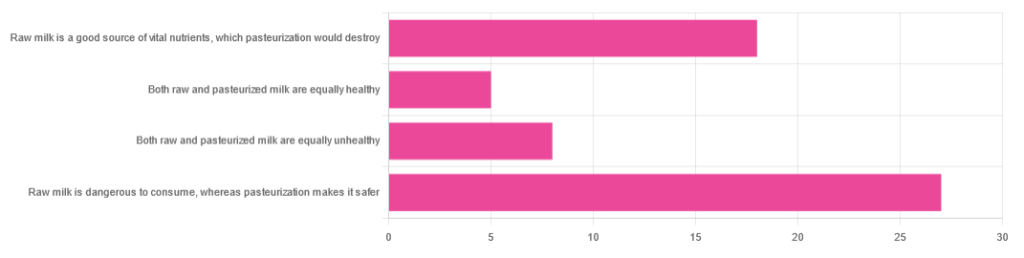
In Wednesday’s newsletter, we asked you for your health-related opinions of raw (cow’s) milk, and got the above-depicted, below-described, set of responses:
- About 47% said “raw milk is dangerous to consume, whereas pasteurization makes it safer”
- About 31% said “raw milk is a good source of vital nutrients which pasteurization would destroy”
- About 14% said “both raw milk and pasteurized milk are equally unhealthy”
- About 9% said “both raw milk and pasteurized milk are equally healthy”
Quite polarizing! So, what does the science say?
“Raw milk is dangerous to consume, whereas pasteurization makes it safer: True or False?”
True! Coincidentally, the 47% who voted for this are mirrored by the 47% of the general US population in a similar poll, deciding between the options of whether raw milk is less safe to drink (47%), just as safe to drink (15%), safer to drink (9%), or not sure (30%):
Public Fails to Appreciate Risk of Consuming Raw Milk, Survey Finds
As for what those risks are, by the way, unpasteurized dairy products are estimated to cause 840x more illness and 45x more hospitalizations than pasteurized products.
This is because unpasteurized milk can (and often does) contain E. coli, Listeria, Salmonella, Cryptosporidium, and other such unpleasantries, which pasteurization kills.
Source for both of the above claims:
(we know the title sounds vague, but all this information is easily visible in the abstract, specifically, the first two paragraphs)
Raw milk is a good source of vital nutrients which pasteurization would destroy: True or False?
False! Whether it’s a “good” source can be debated depending on other factors (e.g., if we considered milk’s inflammatory qualities against its positive nutritional content), but it’s undeniably a rich source. However, pasteurization doesn’t destroy or damage those nutrients.
Incidentally, in the same survey we linked up top, 16% of the general US public believed that pasteurization destroys nutrients, while 41% were not sure (and 43% knew that it doesn’t).
Note: for our confidence here, we are skipping over studies published by, for example, dairy farming lobbies and so forth. Those do agree, by the way, but nevertheless we like sources to be as unbiased as possible. The FDA, which is not completely unbiased, has produced a good list of references for this, about half of which we would consider biased, and half unbiased; the clue is generally in the journal names. For example, Food Chemistry and the Journal of Food Science and Journal of Nutrition are probably less biased than the International Dairy Association and the Journal of Dairy Science:
FDA | Raw Milk Misconceptions and the Danger of Raw Milk Consumption
this page covers a lot of other myths too, more than we have room to “bust” here, but it’s very interesting reading and we recommend to check it out!
Notably, we also weren’t able to find any refutation by counterexample on PubMed, with the very slight exception that some studies sometimes found that in the case of milks that were of low quality, pasteurization can reduce the vitamin E content while increasing the vitamin A content. For most milks however, no significant change was found, and in all cases we looked at, B-vitamins were comparable and vitamin D, popularly touted as a benefit of cow’s milk, is actually added later in any case. And, importantly, because this is a common argument, no change in lipid profiles appears to be findable either.
In science, when something has been well-studied and there aren’t clear refutations by counterexample, and the weight of evidence is clearly very much tipped into one camp, that usually means that camp has it right.
Milk generally is good/bad for the health: True or False?
True or False, depending on what we want to look at. It’s definitely not good for inflammation, but the whole it seems to be cancer-neutral and only increases heart disease risk very slightly:
- Keep Inflammation At Bay ← short version is milk is bad, fermented milk products are fine in moderation
- Is Dairy Scary? ← short version is that milk is neither good nor terrible; fermented dairy products however are health-positive in numerous ways when consumed in moderation
You may be wondering…
…how this goes for the safety of dairy products when it comes to the bird flu currently affecting dairy cows, so:
Take care!
Share This Post
-

‘I went out and I had a cry’: what aged-care staff say about their grief when residents die
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
As our population ages, we’re living longer and dying older. End-of-life care is therefore an increasingly important part of aged care. In Australia, around 50% of people aged over 85 die in an aged care home.
But what does this mean for those who work in aged care? Research suggests aged-care staff experience a unique type of grief when residents die. However, their grief often goes unrecognised, and they may be left with insufficient support.
Maskot/Getty Images Forming relationships over time
Aged-care staff don’t just do tasks such as helping with showering or delivering meals, but engage actively and connect with residents.
In our own research we’ve spoken with aged-care staff who care for older people both in aged-care facilities and in their own homes.
Aged-care staff are aware many of those they look after will die, and that they have a role in supporting older people as they come to the end of their life. In their caring role, they will often form meaningful and rewarding relationships with the older people in their care.
As a result, when the older person dies, this can be a source of profound loss for aged-care workers. As one told us:
I know I cry over some of them that die […] You spend time with them and you love them.
Some aged-care workers we interviewed talked about being present with the older person, talking to them or holding their hands as they died. Others spoke of how they shed tears for the person who had died, but that the tears were also for their loss, because they have known the older person and been involved in their life.
I think what made it worse was when her breathing got very shallow, and I knew she was coming to the end. I did go out. I told her I was going out for a minute. I went out and I had a cry because I wish that I could have saved her, but I knew that I couldn’t.
Sometimes aged-care staff indicated there wasn’t an opportunity for them to say goodbye or be acknowledged as someone who had suffered a loss, even if they had been providing care to the person for a number of months or years. One aged-care worker noted:
If people die in hospital, that’s another grief. Because they don’t get to say goodbye. Often the hospital won’t tell you.
Aged-care staff often must also support families and loved ones as they come to terms with the death of a parent, relative or friend. This can add to the to the emotional toll for staff who may be experiencing their own feelings of grief.
Cumulative grief
Repeated experiences of death can lead to cumulative grief and emotional strain. While staff saw meaning and value in their work, they also found regular exposure to death challenging.
One staff member told us that with time and seeing multiple deaths, you can “feel a little robotic. Because you’ve had to become that way to manage”.
Organisational issues such as staff shortages or high workloads can also exacerbate these feelings of burnout and dissatisfaction. Staff highlighted the need for support in coping.
Sometimes all you want to do is talk. You don’t need someone to solve anything for you. You just want to be heard.
Supporting aged-care staff to manage their grief
Aged-care organisations must take steps to support the wellbeing of their workforce, including acknowledging the grief many feel when older people die.
Following the death of an older person, offering support to staff who have worked closely with that person and acknowledging the emotional bonds that existed are powerful ways of recognising and validating staff grief. Simply asking the staff member how they are going or giving them the chance to take some time to process that the person has died is a good place to start.
Workplaces should also encourage self-care more broadly, promoting activities such as taking scheduled breaks, connecting with colleagues, and prioritising time for relaxation and physical activities. Staff value workplaces that encourage, normalise, and support their self-care practices.
We also need to look at how we can normalise the ability to talk about death and dying within our families and communities. A reluctance to recognise death as part of life can add to the emotional load staff carry, especially if families see dying as a failure of care.
Conversely, aged-care staff have consistently told us how meaningful it is to receive positive feedback and acknowledgement from families. As one worker recalled:
We had a death over the weekend. A really long-term resident here. And the daughter drove in especially this morning to tell me what fantastic care she had. That makes me feel better, that what we’re doing is right.
As members of families and communities, we need to recognise aged-care workers are uniquely vulnerable to feelings of grief and loss, often having built relationships with those in their care over months or years. Supporting the wellbeing of this important workforce supports them to continue to care for us and our loved ones as we age and come to the end of our lives.
Jennifer Tieman, Matthew Flinders Professor and Director of the Research Centre for Palliative Care, Death and Dying, Flinders University and Priyanka Vandersman, Senior Research Fellow, College of Nursing and Health Sciences, Flinders University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Water Bath + More Cookbook for Beginners – by Sarah Roslin
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Whether you want to be prepared for the next major crisis that shuts down food supply chains, or just learn a new skill, this book provides the tools!
Especially beneficial if you also grow your own vegetables, but even you just buy those… Home-canned food is healthy, contains fewer additives and preservatives, and costs less in the long run.
Roslin teaches an array of methods, including most importantly:
- fermentation and pickling
- water bath canning, and
- pressure canning.
As for what’s inside? She covers not just vegetables, but also fruit, seafood, meat… Basically, anything that can be canned.
The book explains the tools and equipment you will need as well as how to perform it safely—as well as common mistakes to avoid!
Lest we be intimidated by the task of acquiring appropriate equipment, she also walks us through what we’ll need in that regard too!
Last but not least, there’s also a (sizeable) collection of simple, step-by-step recipes, catering to a wide variety of tastes.
Bottom line: a highly valuable resource that we recommend heartily.
Share This Post



-
Mounjaro/Zepbound’s Stable Weight Loss Curve
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When it comes to GLP-1 Receptor Agonists (GLP-1 RAs), most of the talk is about semaglutide (e.g. Ozempic and Wegovy), but there are other options. For example:
Ozempic’s cousin drug liraglutide is about to get cheaper. But how does it stack up?
Today, though, we’re going to talk about tirzepatide.
What is tirzepatide?
It’s another GLP-1 RA, meaning that although it’s chemically different from the other aforementioned drugs (and thus gets a separate patent), it’s doing fundamentally the same job in the same fundamental way.
For this reason, sometimes they all get held under the same umbrella when it comes to science examining their effects, for example:
Most People Who Start GLP-1 RAs Quit Them Within A Year (Here’s Why)
Still, there are small differences in their performance in various ways, so they call get different studies, too.
In the main study we’re going to talk about today, they looked at tirzepatide use for weight loss over the course of three years.
Note:
- Mounjaro is terzepatide licensed for use in diabetes
- Zepbound is terzepatide licensed for use in weight loss
They’re the exact same drug and are even made by the same company; the distinction is only because the FDA likes to be paid twice.
About the study
The study followed 690 participants who were took tirzepatide consistently over three years (65% being female, average age 49, average BMI 38.6).
Some results:
- The average time to reach nadir weight (i.e. their lowest recorded weight over the observation period) was 22 months
- Over that time, participants enjoyed a 23.1% mean weight reduction.
- Over the full three years, participants regained an average of 3.7 of those percentage points.
- This means that after the full three years, they had enjoyed, on average, a sustained net loss of 19.4%.
To break it down by dosages (participants were taking 5mg/day, 10mg/day, or 15mg/day):
- 5 mg: 73% regained <5%, 19% regained 5–10%, 8% regained ≥10%
- 10 mg: 65% regained <5%, 26% regained 5–10%, 9% regained ≥10%
- 15 mg: 73% regained <5%, 20% regained 5–10%, 7% regained ≥10%
Which is pretty good! You can read all about it here:
However! Headlines quoting that stat without any kind of caveat are a little misleading, as it can look like it is claiming that if you stop taking it, then you’ll only regain 5% or less from your lowest weight. Which is not true.
If you stop taking it, you’ll indeed bounce back to more or less your original weight, or potentially a little higher, because of metabolic adjustments as a result of losing muscle along with the fat due to eating less.
See also: What happens when I stop taking a drug like Ozempic or Mounjaro?
Want a natural method instead?
It is possible to get many of the effects of GLP-1 RAs without taking GLP-1RAs, by enjoying foods that increase incretin, a hormone group (the most well-known of which is GLP-1) that slows down stomach emptying, which means a gentler blood sugar curve and feeling fuller for longer. It also acts on the hypothalamus, controlling appetite via the brain too (signalling fullness and reducing hunger).
For what foods to focus on, see:
5 Ways To Naturally Boost The “Ozempic Effect” ← this is from Dr. Jason Fung, who is perhaps most well-known for his work in functional medicine for reversing diabetes, and he’s once again giving us sound advice about metabolic hormone-hacking with dietary tweaks!
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
1 Min Fix For Slouched Shoulders (No Equipment Required)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s not actually about your shoulders, which is why trying to fix your shoulder position directly will never work in any useful fashion.
To address the actual issue instead, we must get to the seat of the problem…
It’s about your hips
Slouched shoulders are usually caused by pelvic misalignment, not the shoulders themselves. When the pelvis tilts forward, it creates a chain reaction causing the back to round and the head to push forward, none of which is good for your health. Here’s what to do about it:
- Locate your “sit bone”: sit on a chair or similar surface, and feel for the bone under your hips (sit bone). This bone should sit vertically for proper alignment.
- Loosen your pelvis: place your hands on your pelvis and gently roll it back and forth for a moment to release muscular tension.
- Find the perfect pelvis position: continue rolling the pelvis until the sit bone feels balanced and vertical, like balancing a pan. This automatically engages the core, thoracic spine muscles, and neck support muscles.
- Engage your muscles: while maintaining this alignment, stand up and sit back down slowly 10 times, keeping muscle engagement throughout.
Repeat this exercise whenever you feel slouchy and especially after sitting too long (which is of course best to avoid in the first place, but we know, sometimes it’s unavoidable); it takes less than a minute and helps shoulders straighten naturally.
For more on this plus a visual demonstration, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Stand Up For Your Health (Or Don’t) ← about reducing sitting, and also about reducing the harm of the sitting that you do have to do, including which sitting positions are better for your spine than others.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How To Grow New Brain Cells (At Any Age)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How To Grow New Brain Cells (At Any Age)
It was long believed that brain growth could not occur later in life, due to expending our innate stock of pluripotent stem cells. However, this was mostly based on rodent studies.
Rodent studies are often used for brain research, because it’s difficult to find human volunteers willing to have their brains sliced thinly (so that the cells can be viewed under a microscope) at the end of the study.
However, neurobiologist Dr. Maura Boldrini led a team that did a lot of research by means of autopsies on the hippocampi of (previously) healthy individuals ranging in age from 14 to 79.
What she found is that while indeed the younger subjects did predictably have more young brain cells (neural progenitors and immature neurons), even the oldest subject, at the age of 79, had been producing new brain cells up until death.
Read her landmark study: Human Hippocampal Neurogenesis Persists throughout Aging
There was briefly a flurry of news articles about a study by Dr. Shawn Sorrels that refuted this, however, it later came to light that Dr. Sorrels had accidentally destroyed his own evidence during the cell-fixing process—these things happen; it’s just unfortunate the mistake was not picked up until after publication.
A later study by a Dr. Elena Moreno-Jiménez fixed this flaw by using a shorter fixation time for the cell samples they wanted to look at, and found that there were tens of thousands of newly-made brain cells in samples from adults ranging from 43 to 87.
Now, there was still a difference: the samples from the youngest adult had 30% more newly-made braincells than the 87-year-old, but given that previous science thought brain cell generation stopped in childhood, the fact that an 87-year-old was generating new brain cells 30% less quickly than a 43-year-old is hardly much of a criticism!
As an aside: samples from patients with Alzheimer’s also had a 30% reduction in new braincell generation, compared to samples from patients of the same age without Alzheimer’s. But again… Even patients with Alzheimer’s were still growing some new brain cells.
Read it for yourself: Adult hippocampal neurogenesis is abundant in neurologically healthy subjects and drops sharply in patients with Alzheimer’s disease
Practical advice based on this information
Since we can do neurogenesis at any age, but the rate does drop with age (and drops sharply in the case of Alzheimer’s disease), we need to:
Feed your brain. The brain is the most calorie-consuming organ we have, by far, and it’s also made mostly of fat* and water. So, get plenty of healthy fats, and get plenty of water.
*Fun fact: while depictions in fiction (and/or chemically preserved brains) may lead many to believe the brain has a rubbery consistency, the untreated brain being made of mostly fat and water gives it more of a blancmange-like consistency in reality. That thing is delicate and spatters easily. There’s a reason it’s kept cushioned inside the strongest structure of our body, far more protected than anything in our torso.
Exercise. Specifically, exercise that gets your blood pumping. This (as our earlier-featured video today referenced) is one of the biggest things we can do to boost Brain-Derived Neurotrophic Factor, or BDNF.
Here be science: Brain-Derived Neurotrophic Factor, Depression, and Physical Activity: Making the Neuroplastic Connection
However, that’s not the only way to increase BDNF; another is to enjoy a diet rich in polyphenols. These can be found in, for example, berries, tea, coffee, and chocolate. Technically those last two are also botanically berries, but given how we usually consume them, and given how rich they are in polyphenols, they merit a special mention.
See for example: Effects of nutritional interventions on BDNF concentrations in humans: a systematic review
Some supplements can help neuron (re)growth too, so if you haven’t already, you might want to check out our previous main feature on lion’s mane mushroom, a supplement which does exactly that.
For those who like videos, you may also enjoy this TED talk by neuroscientist Dr. Sandrine Thuret:
Prefer text? Click here to read the transcript
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: