
Ozempic’s cousin drug liraglutide is about to get cheaper. But how does it stack up?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
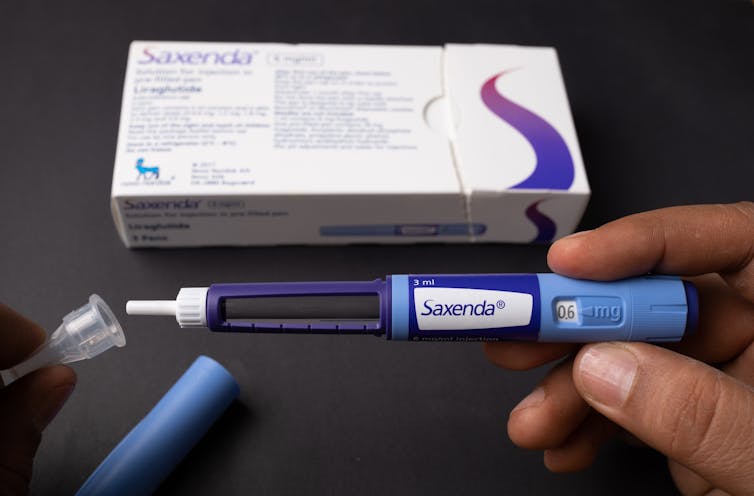
Fourteen years ago, the older drug cousin of semaglutide (Ozempic and Wegovy) came onto the market. The drug, liraglutide, is sold under the brand names Victoza and Saxenda.
Patents for Victoza and Saxenda have now expried. So other drug companies are working to develop “generic” versions. These are likely be a fraction of current cost, which is around A$400 a month.
So how does liraglutide compare with semaglutide?

How do these drugs work?
Liraglutide was not originally developed as a weight-loss treatment. Like semaglutide (Ozempic), it originally treated type 2 diabetes.
The class of drugs liraglutide and semaglutide belong to are known as GLP-1 mimetics, meaning they mimic the natural hormone GLP-1. This hormone is released from your small intestines in response to food and acts in several ways to improve the way your body handles glucose (sugar).
How do they stop hunger?
Liraglutide acts in several regions of the unconscious part of your brain, specifically the hypothalamus, which controls metabolism, and parts of the brain stem responsible for communicating your body’s nutrient status to the hypothalamus.
Its actions here appear to reduce hunger in two different ways. First, it helps you to feel full earlier, making smaller meals more satisfying. Second, it alters your “motivational salience” towards food, meaning it reduces the amount of food you seek out.
Liraglutide’s original formulation, designed to treat type 2 diabetes, was marketed as Victoza. Its ability to cause weight loss was evident soon after it entered the market.
Shortly after, a stronger formulation, called Saxenda, was released, which was intended for weight loss in people with obesity.
How much weight can you lose with liraglutide?
People respond differently and will lose different amounts of weight. But here, we’ll note the average weight loss users can expect. Some will lose more (sometimes much more), others will lose less, and a small proportion won’t respond.
The first GLP-1 mimicking drug was exenatide (Bayetta). It’s still available for treating type 2 diabetes, but there are currently no generics. Exenatide does provide some weight loss, but this is quite modest, typically around 3-5% of body weight.
For liraglutide, those using the drug to treat obesity will use the stronger one (Saxenda), which typically gives about 10% weight loss.
Semaglutide, with the stronger formulation called Wegovy, typically results in 15% weight loss.
The newest GLP-1 mimicking drug on the market, tirzepatide (Mounjaro for type 2 diabetes and Zepbound for weight loss), results in weight loss of around 25% of body weight.
What happens when you stop taking them?
Despite the effectiveness of these medications in helping with weight loss, they do not appear to change people’s weight set-point.
So in many cases, when people stop taking them, they experience a rebound toward their original weight.
What is the dose and how often do you need to take it?
Liraglutide (Victoza) for type 2 diabetes is exactly the same drug as Saxenda for weight loss, but Saxenda is a higher dose.
Although the target for each formulation is the same (the GLP-1 receptor), for glucose control in type 2 diabetes, liraglutide has to (mainly) reach the pancreas.
But to achieve weight loss, it has to reach parts of the brain. This means crossing the blood-brain barrier – and not all of it makes it, meaning more has to be taken.
All the current formulations of GLP-1 mimicking drug are injectables. This won’t change when liraglutide generics hit the market.
However, they differ in how frequently they need to be injected. Liraglutide is a once-daily injection, whereas semaglutide and tirzepatide are once-weekly. (That makes semaglutide and tirzepatide much more attractive, but we won’t see semaglutide as a generic until 2033.)
What are the side effects?
Because all these medicines have the same target in the body, they mostly have the same side effects.
The most common are a range of gastrointestinal upsets including nausea, vomiting, bloating, constipation and diarrhoea. These occur, in part, because these medications slow the movement of food out of the stomach, but are generally managed by increasing the dose slowly.
Recent clinical data suggests the slowing in emptying of the stomach can be problematic for some people, and may increase the risk of of food entering the lungs during operations, so it is important to let your doctor know if you are taking any of these drugs.
Because these are injectables, they can also lead to injection-site reactions.

During clinical trials, there were some reports of thyroid disease and pancreatitis (inflammation of the pancreas). However, it is not clear that these can be attributed to GLP-1 mimicking drugs.
In animals, GLP-1 mimicking drugs drugs have been found to negatively alter the growth of the embryo. There is currently no controlled clinical trial data on their use during pregnancy, but based on animal data, these medicines should not be used during pregnancy.
Who can use them?
The GLP-1 mimicking drugs for weight loss (Wegovy, Saxenda, Zepbound/Mounjaro) are approved for use by people with obesity and are meant to only be used in conjunction with diet and exercise.
These drugs must be prescribed by a doctor and for obesity are not covered by the Pharmaceutical Benefits Scheme, which is one of the reasons why they are expensive. But in time, generic versions of liraglutide are likely to be more affordable.
Sebastian Furness, ARC Future Fellow, School of Biomedical Sciences, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The BAT-pause!

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When Cold Weather & The Menopause Battle It Out
You may know that (moderate, safe) exposure to the cold allows our body to convert our white and yellow fat into the much healthier brown fat—also called brown adipose tissue, or “BAT” to its friends.
If you didn’t already know that, then well, neither did scientists until about 15 years ago:
The Changed Metabolic World with Human Brown Adipose Tissue: Therapeutic Visions
You can read more about it here:
Cool Temperature Alters Human Fat and Metabolism
This is important, especially because the white fat that gets converted is the kind that makes up most visceral fat—the kind most associated with all-cause mortality:
Visceral Belly Fat & How To Lose It ← this is not the same as your subcutaneous fat, the kind that sits directly under your skin and keeps you warm; this is the fat that goes between your organs and of which we should only have a small amount!
The BAT-pause
It’s been known (since before the above discovery) that BAT production slows considerably as we get older. Not too shocking—after all, many metabolic functions slow as we get older, so why should fat regulation be any different?
But! Rodent studies found that this was tied less to age, but to ovarian function: rats who underwent ovariectomies suffered reduced BAT production, regardless of their age.
Naturally, it’s been difficult to recreate such studies in humans, because it’s difficult to find a large sample of young adults willing to have their ovaries whipped out (or even suppressed chemically) to see how badly their metabolism suffers as a result.
Nor can an observational study (for example, of people who incidentally have ovaries removed due to ovarian cancer) usefully be undertaken, because then the cancer itself and any additional cancer treatments would be confounding factors.
Perimenopausal study to the rescue!
A recent (published last month, at time of writing!) study looked at women around the age of menopause, but specifically in cohorts before and after, measuring BAT metabolism.
By dividing the participants into groups based on age and menopausal status, and dividing the post-menopausal group into “takes HRT” and “no HRT” groups, and dividing the pre-menopausal group into “normal ovarian function” and “ovarian production of estrogen suppressed to mimic slightly early menopause” groups (there’s a drug for that), and then having groups exposed to warm and cold temperatures, and measuring BAT metabolism in all cases, they were able to find…
It is about estrogen, not age!
You can read more about the study here:
“Good” fat metabolism changes tied to estrogen loss, not necessarily to aging, shows study
…and the study itself, here:
Brown adipose tissue metabolism in women is dependent on ovarian status
What does this mean for men?
This means nothing directly for (cis) men, sorry.
But to satisfy your likely curiosity: yes, testosterone does at least moderately suppress BAT metabolism—based on rodent studies, anyway, because again it’s difficult to find enough human volunteers willing to have their testicles removed for science (without there being other confounding variables in play, anyway):
Testosterone reduces metabolic brown fat activity in male mice
So, that’s bad per se, but there isn’t much to be done about it, since the rest of your (addressing our male readers here) metabolism runs on testosterone, as do many of your bodily functions, and you would suffer many unwanted effects without it.
However, as men do typically have notably less body fat in general than women (this is regulated by hormones), the effects of changes in BAT metabolism are rather less pronounced in men (per testosterone level changes) than in women (per estrogen level changes), because there’s less overall fat to convert.
In summary…
While menopausal HRT is not necessarily a silver bullet to all metabolic problems, its BAT-maintaining ability is certainly one more thing in its favor.
See also:
Dr. Jen Gunter | What You Should Have Been Told About The Menopause Beforehand
Take care!
Share This Post
-

Fava Beans vs Peas – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing fava beans to peas, we picked the peas.
Why?
Both are great! But…
In terms of macros, the peas have more protein and fiber, winning this category easy-peasy.
In the category of vitamins, fava beans have a little more vitamin C, while peas have rather more of vitamins A, B1, B3, B3, B5, B6, B7, B9, E, and K, sweeping their second category convincingly.
Looking at minerals, fava beans have more sodium, which is not generally considered a plus factor for most of us in industrialized nations most of the time, while peas have more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc—so once again, peas win and it wasn’t close.
Adding up the sections makes for a clear overall win for peas, but by all means do enjoy either both, as fava beans are good too; they just don’t look it when standing next to peas!
Want to learn more?
You might like:
Enjoy!
Share This Post
-
Apple vs Pear – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing apple to pear, we picked the pear.
Why?
Both are great! But there’s a category that puts pears ahead of apples…
Looking at their macros first, pears contain more carbs but also more fiber. Both are low glycemic index foods, though.
In the category of vitamins, things are moderately even: apples contain more of vitamins A, B1, B6, and E, while pears contain more of vitamins B3, B9, K, and choline. That’s a 4:4 split, and the two fruits are about equal in the other vitamins they both contain.
When it comes to minerals, pears contain more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc. A resounding victory for pears, as apples are not higher in any mineral.
In short, if an apple a day keeps the doctor away, a pear should keep the doctor away for about a day and a half, based on the extra nutrients ← this is slightly facetious as medicine doesn’t work like that, but you get the idea: pears simply have more to offer. Apples are still great though! Enjoy both! Diversity is good.
Want to learn more?
You might like to read:
From Apples To Bees, And High-Fructose Cs: Which Sugars Are Healthier, And Which Are Just The Same?
Take care!
Share This Post

-
Apple vs Peach – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing apples to peaches, we picked the peaches.
Why?
Both have their merits, but apples can’t compete with peaches’ micronutrient profile!
In terms of macros, apples have slightly more carbs and fiber, for a comparable glycemic index, so we could either call this a tie, or else give apples a marginal win in the macros category to start with.
In the category of vitamins, apples have more vitamin B6, while peaches have more of vitamins A, B1, B2, B3, B5, B7, B9, C, E, and K—an easy win for peaches.
When it comes to minerals, apples are not higher in any minerals, while peaches have more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc. Another clear win for peaches!
Looking at polyphenols, peaches have a higher total amount (in mg/100g) of polyphenols, as well as more variety thereof. One more round that’s a clear win for peaches.
Adding up the sections makes for an overwhelming overall win for peaches, but by all means enjoy either or both; diversity is best!
Want to learn more?
You might like:
Top 8 Fruits That Prevent & Kill Cancer ← peaches are number 2 on the list! They contain phytochemicals that induce cell death in cancer cells while sparing healthy ones 😎
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Non-Alcohol Mouthwash vs Alcohol Mouthwash – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing non-alcohol mouthwash to alcohol mouthwash, we picked the alcohol.
Why?
Note: this is a contingent choice and is applicable to most, but not all, people.
In short, there has been some concern about alcohol mouthwashes increasing cancer risk, but research has shown this is only the case if you already have an increased risk of oral cancer (for example if you smoke, and/or have had an oral cancer before).
For those for whom this is not the case (for example, if you don’t smoke, and/or have no such cancer history), then best science currently shows that alcohol mouthwash does not cause any increased risk.
What about non-alcohol mouthwashes? Well, they have a different problem; they usually use chlorine-based chemicals like chlorhexidine or cetylpyridinium chloride, which are (exactly as the label promises) exceptionally good at killing oral bacteria.
(They’d kill us too, at higher doses, hence: swill and spit)
Unfortunately, much like the rest of our body, our mouth is supposed to have bacteria there and bad things happen when it doesn’t. In the case of our oral microbiome, cleaning it with such powerful antibacterial agents can kill our “good” bacteria along with the bad, which lowers the pH of our saliva (that’s bad; it means it is more acidic), and thus indirectly erodes tooth enamel.
You can read more about the science of all of the above (with references), here:
Toothpastes & Mouthwashes: Which Help And Which Harm?
Summary:
For most people, alcohol mouthwashes are a good way to avoid the damage that can be done by chlorhexidine in non-alcohol mouthwashes.
Here are some examples, but there will be plenty in your local supermarket:
Non-Alcohol, by Colgate | Alcohol, by Listerine
If you have had oral cancer, or if you smoke, then you may want to seek a third alternative (and also, please, stop smoking if you can).
Or, really, most people could probably skip mouthwashes, if you’ve good oral care already by other means. See also:
Toothpastes & Mouthwashes: Which Help And Which Harm?
(yes, it’s the same link as before, but we’re now drawing your attention to the fact it has information about toothpastes too)
If you do want other options though, might want to check out:
Less Common Oral Hygiene Options ← miswak sticks are especially effective
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Progesterone Menopausal HRT: When, Why, And How To Benefit
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Progesterone doesn’t get talked about as much as other sex hormones, so what’s its deal? Dr. Heather Hirsch explains:
Menopausal progesterone
Dr. Hirsch considers progesterone essential for menopausal women who are taking estrogen and have an intact uterus, to keep conditions at bay such as endometriosis or even uterine cancer.
However, she advises it is not critical in those without a uterus, unless there was a previous case of one of the above conditions.
10almonds addition: on the other hand, progesterone can still be beneficial from a metabolic and body composition standpoint, so do speak with your endocrinologist about it.
As an extra bonus: while not soporific (it won’t make you sleepy), taking progesterone at night will improve the quality of your sleep once you do sleep, so that’s a worthwhile thing for many!
Dr. Hirsch also discusses the merits of continuous vs cyclic use; continuous maintains the above sleep benefits, for example, while cyclic use can help stabilize menstrual patterns in late perimenopause and early menopause.
For more on these things, plus discussion of different types of progesterone, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- What Does “Balance Your Hormones” Even Mean?
- What You Should Have Been Told About The Menopause Beforehand
- HRT: Bioidentical vs Animal – A Tale Of Two Approaches
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:


