Mediterranean Diet… In A Pill?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Does It Come In A Pill?
For any as yet unfamiliar with the Mediterranean diet, you may be wondering what it involves, beyond a general expectation that it’s a diet popularly enjoyed in the Mediterranean. What image comes to mind?
We’re willing to bet that tomatoes feature (great source of lycopene, by the way, and if you’re not getting lycopene, you’re missing out), but what else?
- Salads, perhaps? Vegetables, olives? Olive oil, yea or nay?
- Bread? Pasta? Prosciutto, salami? Cheese?
- Pizza but only if it’s Romana style, not Chicago?
- Pan-seared liver, with some fava beans and a nice Chianti?
In fact, the Mediterranean diet is quite clear on all these questions, so to read about these and more (including a “this yes, that no” list), see:
What Is The Mediterranean Diet, And What Is It Good For?
So, how do we get that in a pill?
A plucky band of researchers, Dr. Chiara de Lucia et al. (quite a lot of “et al.”; nine listed authors on the study), wondered to what extent the benefits of the Mediterranean diet come from the fact that the Mediterranean diet is very rich in polyphenols, and set about testing that, by putting the same polyphenols in capsule form, and running a randomized, double-blind, placebo-controlled, crossover clinical intervention trial.
Now, polyphenols are not the only reason the Mediterranean diet is great; there are also other considerations, such as:
- a great macronutrient balance with lots of fiber, healthy fats, moderate carbs, and protein from select sources
- the absence or at least very low presence of a lot of harmful substances such as refined seed oils, added sugars, refined carbohydrates, and the like (“but pasta” yes pasta; in moderation and wholegrain and served with extra sources of fiber and healthy fats, all of which slow down the absorption of the carbs)
…but polyphenols are admittedly very important too; we wrote about some common aspects of them here:
Tasty Polyphenols: Enjoy Bitter Foods For Your Heart & Brain
As for what Dr. de Lucia et al. put into the capsule, behold…
The ingredients:
- Apple Extract 10.0%
- Pomegranate Extract 10.0%
- Tomato Powder 2.5%
- Beet, Spray Dried 2.5%
- Olive Extract 7.5%
- Rosemary Extract 7.5%
- Green Coffee Bean Extract (CA) 7.5%
- Kale, Freeze Dried 2.5%
- Onion Extract 10.0%
- Ginger Extract 10.0%
- Grapefruit Extract 2.5%
- Carrot, Air Dried 2.5%
- Grape Skin Extract 17.5%
- Blueberry Extract 2.5%
- Currant, Freeze Dried 2.5%
- Elderberry, Freeze Dried 2.5%
And the relevant phytochemicals they contain:
- Quercetin
- Luteolin
- Catechins
- Punicalagins
- Phloretin
- Ellagic Acid
- Naringin
- Apigenin
- Isorhamnetin
- Chlorogenic Acids
- Rosmarinic Acid
- Anthocyanins
- Kaempferol
- Proanthocyanidins
- Myricetin
- Betanin
And what, you may wonder, did they find? Well, first let’s briefly summarise the setup of the study:
They took volunteers (n=30), average age 67, BMI >25, without serious health complaints, not taking other supplements, not vegetarian or vegan, not consuming >5 cups of coffee per day, and various other stipulations like that, to create a fairly homogenous study group who were expected to respond well to the intervention. In contrast, someone who takes antioxidant supplements, already eats many different color plants per day, and drinks 10 cups of coffee, probably already has a lot of antioxidant activity going on, and someone with a lower BMI will generally have lower resting levels of inflammatory markers, so it’s harder to see a change, proportionally.
About those inflammatory markers: that’s what they were testing, to see whether the intervention “worked”; essentially, did the levels of inflammatory markers go up or down (up is bad; down is good).
For more on inflammation, by the way, see:
How to Prevent (or Reduce) Inflammation
…which also explains what it actually is, and some important nuances about it.
Back to the study…
They gave half the participants the supplement for a week and the other half placebo; had a week’s gap as a “washout”, then repeated it, switching the groups, taking blood samples before and after each stage.
What they found:
The group taking the supplement had lower inflammatory markers after a week of taking it, while the group taking the placebo had relatively higher inflammatory markers after a week of taking it; this trend was preserved across both groups (i.e., when they switched roles for the second half).
The results were very significant (p=0.01 or thereabouts), and yet at the same time, quite modest (i.e. the supplement made a very reliable, very small difference), probably because of the small dose (150mg) and small intervention period (1 week).
What the researchers concluded from this
The researchers concluded that this was a success; the study had been primarily to provide proof of principle, not to rock the world. Now they want the experiment to be repeated with larger sample sizes, greater heterogeneity, larger doses, and longer intervention periods.
This is all very reasonable and good science.
What we conclude from this
That ingredients list makes for a good shopping list!
Well, not the extracts they listed, necessarily, but rather those actual fruits, vegetables, etc.
If nine top scientists (anti-aging specialists, neurobiologists, pharmacologists, and at least one professor of applied statistics) came to the conclusion that to get the absolute most bang-for-buck possible, those are the plants to get the phytochemicals from, then we’re not going to ignore that.
So, take another list above and ask yourself: how many of those 16 foods do you eat regularly, and could you work the others in?
Want to make your Mediterranean diet even better?
While the Mediterranean diet is a top-tier catch-all, it can be tweaked for specific areas of health, for example giving it an extra focus on heart health, or brain health, or being anti-inflammatory, or being especially gut healthy:
Four Ways To Upgrade The Mediterranean
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Brain Wash – by Dr. David Perlmutter, Dr. Austin Perlmutter, and Kristen Loberg

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You may be familiar with the lead author of this book, Dr. David Perlmutter, as a big name in the world of preventative healthcare. A lot of his work has focused specifically on carbohydrate metabolism, and he is as associated with grains and he is with brains. This book focuses on the latter.
Dr. Perlmutter et al. take a methodical look at all that is ailing our brains in this modern world, and systematically lay out a plan for improving each aspect.
The advice is far from just dietary, though the chapter on diet takes a clear stance:
❝The food you eat and the beverages you drink change your emotions, your thoughts, and the way you perceive the world❞
The style is explanatory, and the book can be read comfortably as a “sit down and read it cover to cover” book; it’s an enjoyable, informative, and useful read.
Bottom line: if you’d like to give your brain a gentle overhaul, this is the one-stop-shop book to give you the tools to do just that.
Share This Post
-

When Did You Last Have a Cognitive Health Check-Up?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When Did You Last Have a Cognitive Health Check-Up?
Regular health check-ups are an important part of a good health regime, especially as we get older. But after you’ve been prodded, probed, sampled and so forth… When did you last have a cognitive health check-up?
Keeping on top of things
In our recent Monday Research Review main feature about citicoline, we noted that it has beneficial effects for a lot of measures of cognitive health.
And that brought us to realize: just how on top of this are we?
Your writer here today could tell you what her sleep was like on any night in the past year, what her heart rate was like, her weight, and all that. Moods too! There’s an app for that. But cognitive health? My last IQ test was in 2001, and I forget when my last memory test was.
It’s important to know how we’re doing, or else how to we know if there has been some decline? We’ve talked previously about the benefits of brain-training of various kinds to improve cognition, so in some parts we’ll draw on the same resources today, but this time the focus is on getting quick measurements that we can retest regularly (mark the calendar!)
Some quick-fire tests
These tests are all free, quick, and accessible. Some of them will try to upsell you on other (i.e. paid) services; we leave that to your own discretion, but the things we’ll be using today are free.
Test your verbal memory
This one’s a random word list generator. It defaults to 12 words, but you can change that if you like. Memorize the words, and then test yourself by seeing how many you can write down from memory. If it gets too easy, crank up the numbers.
Test your visual memory
This one’s a series of images; the test is to click to say whether you’ve seen this exact image previously in the series or not.
Test your IQ
This one’s intended to be general purpose intelligence; in reality, IQ tests have their flaws too, but it’s not a bad metric to keep track of. Just don’t get too hung up on the outcome, and remember, your only competition is yourself!
Test your attention / focus
This writer opened this and this three other attention tests (to get you the best one) before getting distracted, noting the irony, and finally taking the test. Hopefully you can do better!
Test your creativity
This one’s a random object generator. Give yourself a set period of time (per your preference, but make a note of the time you allow yourself, so that you can use the same time period when you retest yourself at a later date) in which to list as many different possible uses for the item.
Test your musical sense
This one’s a pitch recognition test. So, with the caveat that it is partially testing your hearing as well as your cognition, it’s a good one to take and regularly retest in any case.
How often should you retest?
There’s not really any “should” here, but to offer some advice:
- If you take them too often, you might find you get bored of doing so and stop, essentially burning out.
- If you don’t take them regularly, you may forget, lose this list of tests, etc.
- Likely a good “sweet spot” is quarterly or six-monthly, but there’s nothing wrong with testing annually either.
It’s all about the big picture, after all.
Share This Post
-

What happens in my brain when I get a migraine? And what medications can I use to treat it?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Migraine is many things, but one thing it’s not is “just a headache”.
“Migraine” comes from the Greek word “hemicrania”, referring to the common experience of migraine being predominantly one-sided.
Some people experience an “aura” preceding the headache phase – usually a visual or sensory experience that evolves over five to 60 minutes. Auras can also involve other domains such as language, smell and limb function.
Migraine is a disease with a huge personal and societal impact. Most people cannot function at their usual level during a migraine, and anticipation of the next attack can affect productivity, relationships and a person’s mental health.

Francisco Gonzelez/Unsplash What’s happening in my brain?
The biological basis of migraine is complex, and varies according to the phase of the migraine. Put simply:
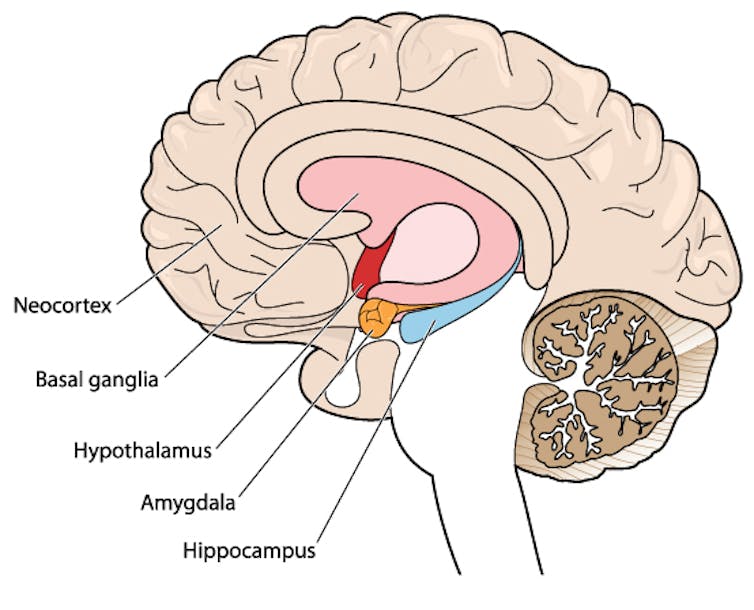
The earliest phase is called the prodrome. This is associated with activation of a part of the brain called the hypothalamus which is thought to contribute to many symptoms such as nausea, changes in appetite and blurred vision.
The hypothalamus is shown here in red. Blamb/Shutterstock Next is the aura phase, when a wave of neurochemical changes occur across the surface of the brain (the cortex) at a rate of 3–4 millimetres per minute. This explains how usually a person’s aura progresses over time. People often experience sensory disturbances such as flashes of light or tingling in their face or hands.
In the headache phase, the trigeminal nerve system is activated. This gives sensation to one side of the face, head and upper neck, leading to release of proteins such as CGRP (calcitonin gene-related peptide). This causes inflammation and dilation of blood vessels, which is the basis for the severe throbbing pain associated with the headache.
Finally, the postdromal phase occurs after the headache resolves and commonly involves changes in mood and energy.
What can you do about the acute attack?
A useful way to conceive of migraine treatment is to compare putting out campfires with bushfires. Medications are much more successful when applied at the earliest opportunity (the campfire). When the attack is fully evolved (into a bushfire), medications have a much more modest effect.
Aspirin
For people with mild migraine, non-specific anti-inflammatory medications such as high-dose aspirin, or standard dose non-steroidal medications (NSAIDS) can be very helpful. Their effectiveness is often enhanced with the use of an anti-nausea medication.
Triptans
For moderate to severe attacks, the mainstay of treatment is a class of medications called “triptans”. These act by reducing blood vessel dilation and reducing the release of inflammatory chemicals.
Triptans vary by their route of administration (tablets, wafers, injections, nasal sprays) and by their time to onset and duration of action.
The choice of a triptan depends on many factors including whether nausea and vomiting is prominent (consider a dissolving wafer or an injection) or patient tolerability (consider choosing one with a slower onset and offset of action).
As triptans constrict blood vessels, they should be used with caution (or not used) in patients with known heart disease or previous stroke.
Triptans should be used cautiously in patients with heart disease. CDC/Unsplash Gepants
Some medications that block or modulate the release of CGRP, which are used for migraine prevention (which we’ll discuss in more detail below), also have evidence of benefit in treating the acute attack. This class of medication is known as the “gepants”.
Gepants come in the form of injectable proteins (monoclonal antibodies, used for migraine prevention) or as oral medication (for example, rimegepant) for the acute attack when a person has not responded adequately to previous trials of several triptans or is intolerant of them.
They do not cause blood vessel constriction and can be used in patients with heart disease or previous stroke.
Ditans
Another class of medication, the “ditans” (for example, lasmiditan) have been approved overseas for the acute treatment of migraine. Ditans work through changing a form of serotonin receptor involved in the brain chemical changes associated with the acute attack.
However, neither the gepants nor the ditans are available through the Pharmaceutical Benefits Scheme (PBS) for the acute attack, so users must pay out-of-pocket, at a cost of approximately A$300 for eight wafers.
What about preventing migraines?
The first step is to see if lifestyle changes can reduce migraine frequency. This can include improving sleep habits, routine meal schedules, regular exercise, limiting caffeine intake and avoiding triggers such as stress or alcohol.
Despite these efforts, many people continue to have frequent migraines that can’t be managed by acute therapies alone. The choice of when to start preventive treatment varies for each person and how inclined they are to taking regular medication. Those who suffer disabling symptoms or experience more than a few migraines a month benefit the most from starting preventives.
Some people will take medicines to prevent migraines. Tbel Abuseridze/Unsplash Almost all migraine preventives have existing roles in treating other medical conditions, and the physician would commonly recommend drugs that can also help manage any pre-existing conditions. First-line preventives include:
- tablets that lower blood pressure (candesartan, metoprolol, propranolol)
- antidepressants (amitriptyline, venlafaxine)
- anticonvulsants (sodium valproate, topiramate).
Some people have none of these other conditions and can safely start medications for migraine prophylaxis alone.
For all migraine preventives, a key principle is starting at a low dose and increasing gradually. This approach makes them more tolerable and it’s often several weeks or months until an effective dose (usually 2- to 3-times the starting dose) is reached.
It is rare for noticeable benefits to be seen immediately, but with time these drugs typically reduce migraine frequency by 50% or more.
‘Nothing works for me!’
In people who didn’t see any effect of (or couldn’t tolerate) first-line preventives, new medications have been available on the PBS since 2020. These medications block the action of CGRP.
The most common PBS-listed anti-CGRP medications are injectable proteins called monoclonal antibodies (for example, galcanezumab and fremanezumab), and are self-administered by monthly injections.
These drugs have quickly become a game-changer for those with intractable migraines. The convenience of these injectables contrast with botulinum toxin injections (also effective and PBS-listed for chronic migraine) which must be administered by a trained specialist.
Up to half of adolescents and one-third of young adults are needle-phobic. If this includes you, tablet-form CGRP antagonists for migraine prevention are hopefully not far away.
Data over the past five years suggest anti-CGRP medications are safe, effective and at least as well tolerated as traditional preventives.
Nonetheless, these are used only after a number of cheaper and more readily available first-line treatments (all which have decades of safety data) have failed, and this also a criterion for their use under the PBS.
Mark Slee, Associate Professor, Clinical Academic Neurologist, Flinders University and Anthony Khoo, Lecturer, Flinders University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post



Related Posts
-

What Most People Are Missing When Trying To Touch Their Toes
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Touching your toes is considered an important measure of flexibility… And it is!
However…
The unseen parts
It isn’t just about flexibility—it’s also about posture, and strong body mechanics. And that’s the reason that many people fail despite sustained periods of trying. So instead of just stretching and hoping and stretching and hoping, take the necessary extra step of including exercises like these in your routine:
- Seated forward fold with band: sit with your legs straight and toes pointed up; loop a band around your feet, keep your back straight, and gently pull yourself forwards.
- Downward dog heel pedal: start in downward dog with your feet hip-width apart and hips lifted high, and then alternately bend each knee while pressing the opposite heel towards the floor.
- Standing pancake (closed hips): stand with your legs wider than shoulder-width and your toes pointing straight forwards; hinge from your hips to fold your torso downwards, reaching towards the floor or your ankles (while keeping your legs straight and hips square.
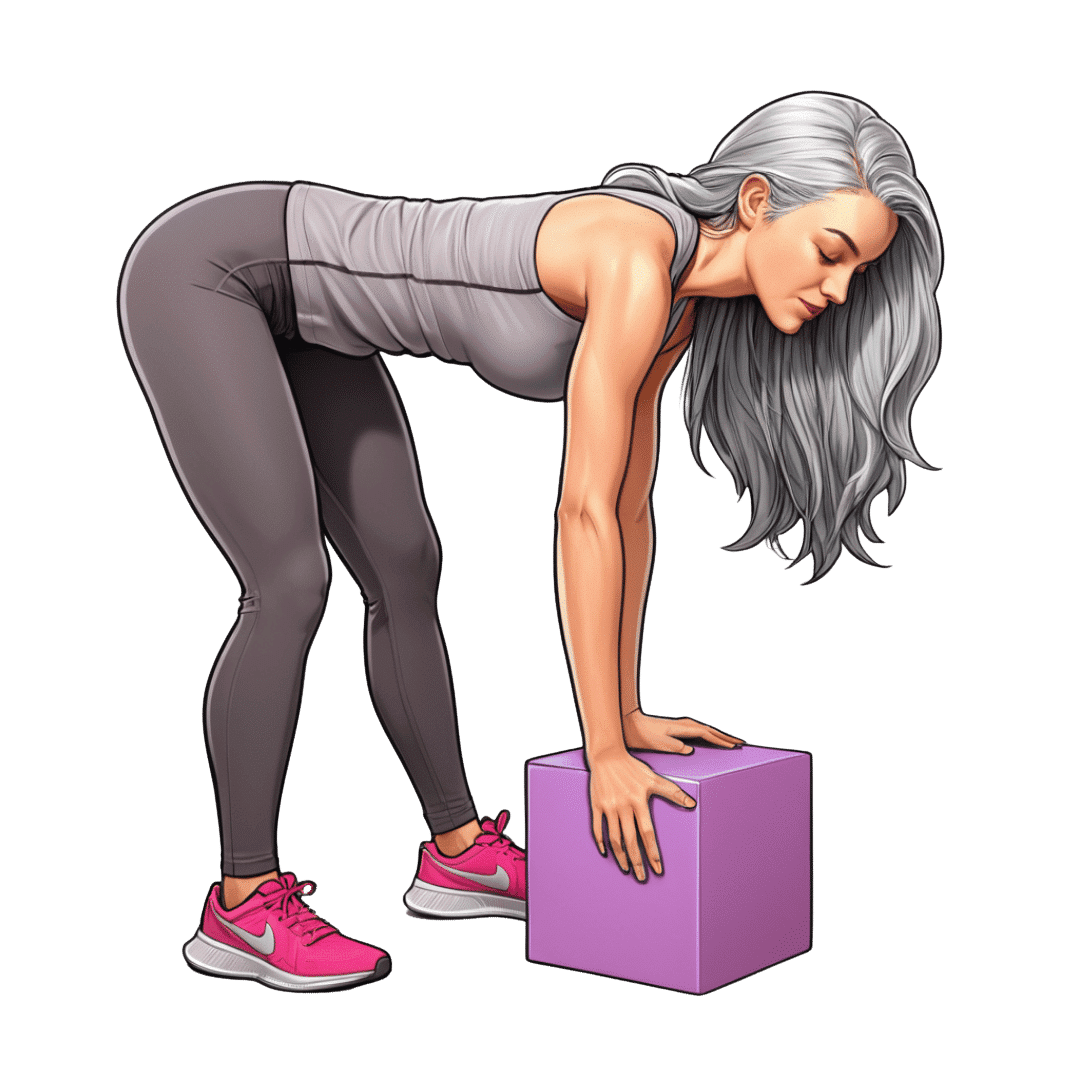
- Jefferson curl: stand on a small box or step with light weights in your hands; tuck your chin to your chest and roll your spine down one vertebra at a time, letting the weights gently pull you deeper. Pause at the bottom, then slowly reverse the movement to return upright—this strengthens spinal control and stretches your entire posterior chain.
For more on all of this plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Can’t Do The Middle Splits? Two Anatomy Tricks To Get You Deeper In Seconds
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Undoing The Damage Of Life’s Hard Knocks
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Sometimes, What Doesn’t Kill Us Makes Us Insecure
We’ve written before about Complex PTSD, which is much more common than the more popularly understood kind:
Given that C-PTSD affects so many people (around 1 in 5, but really, do read the article above! It explains it better than we have room to repeat today), it seems like a good idea to share tips for managing it.
(Last time, we took all the space for explaining it, so we just linked to some external resources at the end)
What happened to you?
PTSD has (as a necessity, as part of its diagnostic criteria) a clear event that caused it, which makes the above question easy to answer.
C-PTSD often takes more examination to figure out what tapestry of circumstances (and likely but not necessarily: treatment by other people) caused it.
Often it will feel like “but it can’t be that; that’s not that bad”, or “everyone has things like that” (in which case, you’re probably one of the one in five).
The deeper questions
Start by asking yourself: what are you most afraid of, and why? What are you most ashamed of? What do you fear that other people might say about you?
Often there is a core pattern of insecurity that can be summed up in a simple, harmful, I-message, e.g:
- I am a bad person
- I am unloveable
- I am a fake
- I am easy to hurt
- I cannot keep my loved ones safe
…and so forth.
For a bigger list of common insecurities to see what resonates, check out:
Basic Fears/Insecurities, And Their Corresponding Needs/Desires
Find where they came from
You probably learned bad beliefs, and consequently bad coping strategies, because of bad circumstances, and/or bad advice.
- When a parent exclaimed in anger about how stupid you are
- When a partner exclaimed in frustration that always mess everything up
- When an employer told you you weren’t good enough
…or maybe they told you one thing, and showed you the opposite. Or maybe it was entirely non-verbal circumstances:
- When you gambled on a good idea and lost everything
- When you tried so hard at some important endeavour and failed
- When you thought someone could be trusted, and learned the hard way that you were wrong
These are “life’s difficult bits”, but when we’ve lived through a whole stack of them, it’s less like a single shattering hammer-blow of PTSD, and more like the consistent non-stop tap tap tap that ends up doing just as much damage in the long run.
Resolve them
That may sound a bit like a “and quickly create world peace” level of task, but we have tools:
Ask yourself: what if…
…it had been different? Take some time and indulge in a full-blown fantasy of a life that was better. Explore it. How would those different life lessons, different messages, have impacted who you are, your personality, your behaviour?
This is useful, because the brain is famously bad at telling real memories from false ones. Consciously, you’ll know that one was an exploratory fantasy, but to your brain, it’s still doing the appropriate rewiring. So, little by little, neuroplasticity will do its thing.
Tell yourself a better lie
We borrowed this one from the title of a very good book which we’ve reviewed previously.
This idea is not about self-delusion, but rather that we already express our own experiences as a sort of narrative, and that narrative tends to contain value judgements that are often not useful, e.g. “I am stupid”, “I am useless”, and all the other insecurities we mentioned earlier. Some simple examples might be:
- “I had a terrible childhood” → “I have come so far”
- “I should have known better” → “I am wiser now”
- “I have lost so much” → “I have experienced so much”
So, replacing that self-talk can go a long way to re-writing how secure we feel, and therefore how much trauma-response (ideally: none!) we have to stimuli that are not really as threatening as we sometimes feel they are (a hallmark of PTSD in general).
Here’s a guide to more ways:
How To Get Your Brain On A More Positive Track (Without Toxic Positivity)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Medications That Shouldn’t Be Taken Long-term (With Natural Alternatives)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Leonid Kim helps us avoid hurting our organs and more:
Swaps to consider
Body
- PPIs (usually prescribed for heartburn): drugs like omeprazole and esomeprazole reduce stomach acid but long-term use is associated with kidney injury, magnesium deficiency (on which note, do be aware of: How’s Your Magnesium Depletion Score?), and a 65% increased odds of vitamin B12 deficiency after 2 or more years. If you are going to supplement B12, by the way, that’s a good idea for a lot of people, but do avoid making a common mistake that many make in this regard: Which B Vitamins? It Makes A Difference ← in short, the most common vitamer of B12, cyanocobalamin, isn’t that effective, and you might want to spring for methylcobalamin, hydroxycobalamin, and/or adenosylcobalamin, all three of which are active vitamers of B12 that the body can use much more efficiently. You may be wondering why, then, cyanocobalamin is the most common: simple, it’s cheaper to produce!
- Heartburn alternatives: reduce visceral fat to lower stomach pressure, practice diaphragmatic breathing to strengthen the lower esophageal sphincter, and improve gastric emptying with walking after meals, and ginger tea. See also: Acid Reflux After Meals? Here’s How To Stop It Naturally
- Z-drugs (sleep medications): drugs like zolpidem act on the GABA system to induce sleep but can lead to dependence within weeks, and are linked to complex sleep behaviors like sleepwalking, cooking, or driving while asleep. Needless to say, those things are not good for the health.
- Sleep alternatives: maintain consistent sleep and wake times and get morning light exposure within 30 minutes of waking to regulate your circadian rhythm. If you do want something to take, though, swing by: Safe Effective Sleep Aids For Seniors
- Anticholinergics: drugs like diphenhydramine, oxybutynin, and amitriptyline are used for allergies, bladder issues, sleep, and depression and are associated with a 46% increased risk of dementia after 3 or more months of use, with risk increasing alongside cumulative exposure.
- Anticholinergic alternatives: switch to second-generation antihistamines when appropriate (see: Antihistamines’ Generation Gap) and use bladder training and pelvic floor muscle training, which can reduce incontinence episodes by 60 to 80% in women. You might also want to take note of: Foods Linked To Urinary Incontinence In Middle-Age (& Foods That Avert It)
- Gabapentin: originally approved for seizures and postherpetic nerve pain but widely used for other conditions, with long-term use associated with cognitive slowing (we wrote about that here: The Painkiller That Increases Cognitive Impairment Risk By 85%), dizziness, impaired balance, and physical dependence.
- Neuropathy alternatives: address underlying causes like blood sugar control, improve insulin resistance with diet and exercise, and correct vitamin deficiencies to reduce nerve damage and pain (learn more: Peripheral Neuropathy: How To Avoid It, Manage It, Treat It).
For less on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Are You Taking PIMs? Getting Off The Overmedication Train ← “PIMs” stands for “potentially inappropriate medications”, be they prescribed in error, or to treat a side effect of some other medication, or to treat something that has now long-since passed.
Also, for that matter:
Before You Reach For That Tylenol… ← Tylenol (paracetamol/acetaminophen) is intended for occasional use only, and can cause severe problems if used chronically (not to mention death, if overused)
And while we’re doing painkillers, you might also want to check out:
The Commonly-Prescribed Painkiller That Barely Works (And Is Dangerous)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
- PPIs (usually prescribed for heartburn): drugs like omeprazole and esomeprazole reduce stomach acid but long-term use is associated with kidney injury, magnesium deficiency (on which note, do be aware of: How’s Your Magnesium Depletion Score?), and a 65% increased odds of vitamin B12 deficiency after 2 or more years. If you are going to supplement B12, by the way, that’s a good idea for a lot of people, but do avoid making a common mistake that many make in this regard: Which B Vitamins? It Makes A Difference ← in short, the most common vitamer of B12, cyanocobalamin, isn’t that effective, and you might want to spring for methylcobalamin, hydroxycobalamin, and/or adenosylcobalamin, all three of which are active vitamers of B12 that the body can use much more efficiently. You may be wondering why, then, cyanocobalamin is the most common: simple, it’s cheaper to produce!