Mediterranean Diet Book Suggestions
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝What is Mediterranean diet which book to read?❞
We did a special edition about the Mediterranean Diet! So that’s a great starting point.
As to books, there are so many, and we review books about it from time to time, so keep an eye out for our daily “One-Minute Book Review” section. We do highly recommend “How Not To Die”, which is a science-heavy approach to diet-based longevity, and essentially describes the Mediterranean Diet, with some tweaks.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Ideal Blood Pressure Numbers Explained

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝Maybe I missed it but the study on blood pressure did it say what the 2 numbers should read ideally?❞
We linked it at the top of the article rather than including it inline, as we were short on space (and there was a chart rather than a “these two numbers” quick answer), but we have a little more space today, so:
Category Systolic (mm Hg) Diastolic (mm Hg) Normal < 120 AND < 80 Elevated 120 – 129 AND < 80 Stage 1 – High Blood Pressure 130 – 139 OR 80 – 89 Stage 2 – High Blood Pressure 140 or higher OR 90 or higher Hypertensive Crisis Above 180 AND/OR Above 120 To oversimplify for a “these two numbers” answer, under 120/80 is generally considered good, unless it is under 90/60, in which case that becomes hypotension.
Hypotension, the blood pressure being too low, means your organs may not get enough oxygen and if they don’t, they will start shutting down.
To give you an idea how serious this, this is the closed-circuit equivalent of the hypovolemic shock that occurs when someone is bleeding out onto the floor. Technically, bleeding to death also results in low blood pressure, of course, hence the similarity.
So: just a little under 120/80 is great.
Share This Post
-

Grains: Bread Of Life, Or Cereal Killer?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Going Against The Grain?

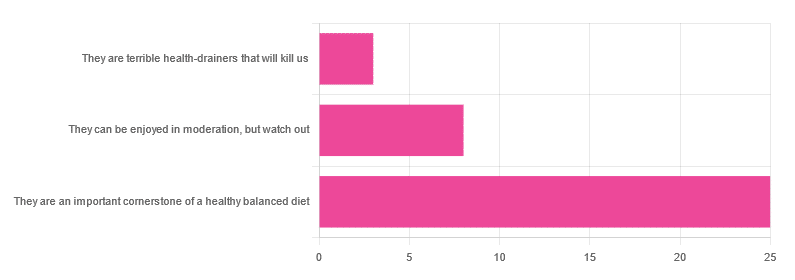
In Wednesday’s newsletter, we asked you for your health-related opinion of grains (aside from any gluten-specific concerns), and got the above-depicted, below-described, set of responses:
- About 69% said “They are an important cornerstone of a healthy balanced diet”
- About 22% said “They can be enjoyed in moderation, but watch out”
- About 8% said “They are terrible health-drainers that will kill us”
So, what does the science say?
They are terrible health-drainers that will kill us: True or False?
True or False depending on the manner of their consumption!
There is a big difference between the average pizza base and a bowl of oats, for instance. Or rather, there are a lot of differences, but what’s most critical here?
The key is: refined and ultraprocessed grains are so inferior to whole grains as to be actively negative for health in most cases for most people most of the time.
But! It’s not because processing is ontologically evil (in reality: some processed foods are healthy, and some unprocessed foods are poisonous). although it is a very good general rule of thumb.
So, we need to understand the “why” behind the “key” that we just gave above, and that’s mostly about the resultant glycemic index and associated metrics (glycemic load, insulin index, etc).
In the case of refined and ultraprocessed grains, our body gains sugar faster than it can process it, and stores it wherever and however it can, like someone who has just realised that they will be entertaining a houseguest in 10 minutes and must tidy up super-rapidly by hiding things wherever they’ll fit.
And when the body tries to do this with sugar from refined grains, the result is very bad for multiple organs (most notably the liver, but the pancreas takes quite a hit too) which in turn causes damage elsewhere in the body, not to mention that we now have urgently-produced fat stored in unfortunate places like our liver and abdominal cavity when it should have gone to subcutaneous fat stores instead.
In contrast, whole grains come with fiber that slows down the absorption of the sugars, such that the body can deal with them in an ideal fashion, which usually means:
- using them immediately, or
- storing them as muscle glycogen, or
- storing them as subcutaneous fat
👆 that’s an oversimplification, but we only have so much room here.
For more on this, see:
Glycemic Index vs Glycemic Load vs Insulin Index
And for why this matters, see:
Which Sugars Are Healthier, And Which Are Just The Same?
And for fixing it, see:
They can be enjoyed in moderation, but watch out: True or False?
Technically True but functionally False:
- Technically true: “in moderation” is doing a lot of heavy lifting here. One person’s “moderation” may be another person’s “abstemiousness” or “gluttony”.
- Functionally false: while of course extreme consumption of pretty much anything is going to be bad, unless you are Cereals Georg eating 10,000 cereals each day and being a statistical outlier, the issue is not the quantity so much as the quality.
Quality, we discussed above—and that is, as we say, paramount. As for quantity however, you might want to know a baseline for “getting enough”, so…
They are an important cornerstone of a healthy balanced diet: True or False?
True! This one’s quite straightforward.
3 servings (each being 90g, or about ½ cup) of whole grains per day is associated with a 22% reduction in risk of heart disease, 5% reduction in all-cause mortality, and a lot of benefits across a lot of disease risks:
❝This meta-analysis provides further evidence that whole grain intake is associated with a reduced risk of coronary heart disease, cardiovascular disease, and total cancer, and mortality from all causes, respiratory diseases, infectious diseases, diabetes, and all non-cardiovascular, non-cancer causes.
These findings support dietary guidelines that recommend increased intake of whole grain to reduce the risk of chronic diseases and premature mortality.❞
~ Dr. Dagfinn Aune et al.
We’d like to give a lot more sources for the same findings, as well as papers for all the individual claims, but frankly, there are so many that there isn’t room. Suffice it to say, this is neither controversial nor uncertain; these benefits are well-established.
Here’s a very informative pop-science article, that also covers some of the things we discussed earlier (it shows what happens during refinement of grains) before getting on to recommendations and more citations for claims than we can fit here:
Harvard School Of Public Health | Whole Grains
“That’s all great, but what if I am concerned about gluten?”
There certainly are reasons you might be, be it because of a sensitivity, allergy, or just because perhaps you’d like to know more.
Let’s first mention: not all grains contain gluten, so it’s perfectly possible to enjoy naturally gluten-free grains (such as oats and rice) as well as gluten-free pseudocereals, which are not actually grains but do the same job in culinary and nutritional terms (such as quinoa and buckwheat, despite the latter’s name).
Finally, if you’d like to know more about gluten’s health considerations, then check out our previous mythbusting special:
Enjoy!
Share This Post
-
Five Supplements That Actually Work Vs Arthritis
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.

This is Dr. Diana Girnita, a double board-certified physician (internal medicine & rheumatology) who, in addition to her MD, also has a PhD in immunology—bearing in mind that rheumatoid arthritis is an autoimmune condition.
Her mission is to help people with any form of arthritis (rheumatoid or otherwise) and those with many non-arthritic autoimmune conditions (ranging from tendonitis to lupus) to live better.
Today, we’ll be looking at her recommendations of 5 supplements that actually help alleviate arthritis:
Collagen
Collagen famously supports skin, nails, bones, and joint cartilage; Dr. Girnita advises that it’s particularly beneficial for osteoarthritis.
Specifically, she recommends either collagen peptides or hydrolyzed collagen, as they are most absorbable. However, collagen can also be sourced from foods like bone broth, fish with skin and bones, and gelatin-based foods.
If you’re vegetarian/vegan, then it becomes important to simply consume the ingredients for collagen, because like most animals, we can synthesize it ourselves provided we get the necessary nutrients. For more on that, see:
We Are Such Stuff As Fish Are Made Of
Glucosamine & chondroitin
Technically two things, but almost always sold/taken together. Naturally found in joint cartilage, it can slow cartilage breakdown and reduce pain in osteoarthritis.
Studies show pain relief, especially in moderate-to-severe cases; best taken long-term. Additionally, it’s a better option than NSAIDs for patients with heart or gastrointestinal issues.
10almonds tip: something that’s tricker to find as a supplement than glucosamine and chondroitin, but you might want to check it out:
Cucumber Extract Beats Glucosamine & Chondroitin… At 1/135th Of The Dose?!
Omega-3 fatty acids
Dr. Girnita recommends this one because unlike the above recommendations that mainly help reduce/reverse the joint damage itself, omega-3 reduces inflammation, pain, and stiffness, and can decrease or eliminate the need for NSAIDs in rheumatoid arthritis and psoriatic arthritis.
She recommends 2-4g EPA/DHA daily; ideally taken with a meal for better absorption.
She also recommends to look for mercury-free options—algae-derived are usually better than fish-derived, but check for certification either way! See also:
What Omega-3 Fatty Acids Really Do For Us
Boswellia serrata (frankincense)
Popularly enjoyed as an incense but also available in supplement form, it contains boswellic acid, which reduces inflammation and cartilage damage.
Dr. Girnita recommends 100 mg daily, but advises that it may interact with some antidepressants, anti-anxiety medications, and NSAIDs—so speak with your pharmacist/doctor if unsure.
We also wrote about this one here:
Science-Based Alternative Pain Relief
Curcumin (turmeric)
Well-known for its potent anti-inflammatory properties, it’s comparable to NSAIDs in pain relief for most common forms of arthritis.
Dr. Girnita recommends 1–1.5g of curcumin daily, ideally combined with black pepper for better absorption:
Why Curcumin (Turmeric) Is Worth Its Weight In Gold
Lastly…
Dr. Girnita advises to not blindly trust supplements, but rather, to test them for 2–3 months while keeping a journal of your symptoms. If it improves things for you, keep it up, if not, discontinue. Humans can be complicated and not everything will work exactly the same way for everyone!
For more on dealing with chronic pain specifically, by the way, check out:
Managing Chronic Pain (Realistically!)
Take care!
Share This Post

Related Posts
-
Ruminating vs Processing
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When it comes to traumatic experiences, there are two common pieces of advice for being able to move forwards functionally:
- Process whatever thoughts and feelings you need to process
- Do not ruminate
The latter can seem, at first glance, a lot like the former. So, how to tell them apart, and how to do one without the other?
Getting tense
One major difference between the two is the tense in which our mental activity takes place:
- processing starts with the traumatic event (or perhaps even the events leading up to the traumatic event), analyses what happened and if possible why, and then asks the question “ok, what now?” and begins work on laying out a path for the future.
- rumination starts with the traumatic event (or perhaps even the events leading up to the traumatic event), analyses what happened and if why, oh why oh why, “I was such an idiot, if only I had…” and gets trapped in a fairly tight (and destructive*) cycle of blame and shame/anger, never straying far from the events in question.
*this may be directly self-destructive, but it can also sometimes be only indirectly self-destructive, for example if the blame and anger is consciously placed with someone else.
This idea fits in, by the way, with Dr. Elisabeth Kübler-Ross’s “five stages of grief” model; rumination here represents the stages “bargaining”, “despair”, and “anger”, while emotional processing here represents the stage “acceptance”. Thus, it may be that rumination does have a place in the overall process—just don’t get stuck there!
For more on healthily processing grief specifically:
What Grief Does To The Body (And How To Manage It)
Grief, by the way, can be about more than the loss of a loved one; a very similar process can play out with many other kinds of unwanted life changes too.
What are the results?
Another way to tell them apart is to look at the results of each. If you come out of a long rumination session feeling worse than when you started, it’s highly unlikely that you just stopped too soon and were on the verge of some great breakthrough. It’s possible! But not likely.
- Processing may be uncomfortable at first, and if it’s something you’ve ignored for a long time, that could be very uncomfortable at first, but there should quite soon be some “light at the end of the tunnel”. Perhaps not even because a solution seems near, but because your mind and body recognize “aha, we are doing something about it now, and thus may find a better way forward”.
- Rumination tends to intensify and prolong uncomfortable emotions, increases stress and anxiety, and likely disrupts sleep. At best, it may serve as a tipping point to seek therapy or even just recognize “I should figure out a way to deal with this, because this isn’t doing me any good”. At worst, it may serve as a tipping point to depression, and/or substance abuse, and/or suicidality.
See also: How To Stay Alive (When You Really Don’t Want To) ← which also has a link back to our article on managing depression, by the way!
Did you choose it, really?
A third way to tell them apart is the level of conscious decision that went into doing it.
- Processing is almost always something that one decides “ok, let’s figure this out”, and sits down to figure it out.
- Rumination tends to be about as voluntary as social media doomscrolling. Technically we may have decided to begin it (we also might not have made any conscious decision, and just acted on impulse), but let’s face it, our hands weren’t at the wheel for long, at all.
A good way to make sure that it is a conscious process, is to schedule time for it in advance, and then do it only during that time. If thoughts about it come up at other times, tell yourself “no, leave that for later”, and then deal with it when (and only when) the planned timeslot arrives.
It’s up to you and your schedule what time you pick, but if you’re unsure, consider an hour in the early evening. That means that the business of the day is behind you, but it’s also not right before bed, so you should have some decompression time as a buffer. So for example, perhaps after dinner you might set a timer* for an hour, and sit down to journal, brainstorm, or just plain think, about the matter that needs processing.
*electronic timers can be quite jarring, and may distract you while waiting for the beeps. So, consider investing in a relaxing sand timer like this one instead.
Is there any way to make rumination less bad?
As we mentioned up top, there’s a case to be made for “rumination is an early part of the process that gets us where we need to go, and may not be skippable, or may not be advisable to skip”.
So, if you are going to ruminate, then firstly, we recommend again bordering it timewise (with a timer as above) and having a plan to pull yourself out when you’re done rather than getting stuck there (such as: The Off-Button For Your Brain: How To Stop Negative Thought Spirals).
And secondly, you might want to consider the following technique, which allows one to let one’s brain know that the thing we’re thinking about / imagining is now to be filed away safely; not lost or erased, but sent to the same place that nightmares go after we wake up:
A Surprisingly Powerful Tool: Eye Movement Desensitization & Reprocessing (EMDR)
What if I actually do want to forget?
That’s not usually recommendable; consider talking it through with a therapist first. However, for your interest, there is a way:
The Dark Side Of Memory (And How To Forget)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Pomegranate vs Cranberries – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing pomegranate to cranberries, we picked the pomegranate.
Why?
Starting with the macros: pomegranate has nearly 4x the protein (actually quite a lot for a fruit, but this is not too surprising—it’s because we are eating the seeds!), and slightly more carbs and fiber. Their glycemic indices are comparable, both being low GI foods. While both of these fruits have excellent macro profiles, we say the pomegranate is slightly better, because of the protein, and when it comes to the carbs and fiber, since they balance each other out, we’ll go with the option that’s more nutritionally dense. We like foods that add more nutrients!
In the category of vitamins, pomegranate is higher in vitamins B1, B2, B3, B5, B6, B9, K, and choline, while cranberry is higher in vitamins A, C, and E. Both are very respectable profiles, but pomegranate wins on strength of numbers (and also some higher margins of difference).
When it comes to minerals, it is not close; pomegranate is higher in calcium, copper, iron, magnesium, phosphorus, potassium, selenium, and zinc, while cranberry is higher in manganese. An easy win for pomegranate here.
Both of these fruits have additional “special” properties, though it’s worth noting that:
- pomegranate’s bonus properties, which are too many to list here, but we link to an article below, are mostly in its peel (so dry it, and grind it into a powder supplement, that can be worked into foods, or used like an instant fruit tea, just without the sugar)
- cranberries’ bonus properties (including: famously very good at reducing UTI risk) come with some warnings, including that they may increase the risk of kidney stones if you are prone to such, and also that cranberries have anti-clotting effects, which are great for heart health but can be a risk of you’re on blood thinners or have a bleeding disorder.
You can read about both of these fruits’ special properties in more detail below:
Want to learn more?
You might like to read:
- Health Benefits Of Cranberries (But: You’d Better Watch Out)
- Pomegranate’s Health Gifts Are Mostly In Its Peel
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Ouch. That ‘Free’ Annual Checkup Might Cost You. Here’s Why.
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When Kristy Uddin, 49, went in for her annual mammogram in Washington state last year, she assumed she would not incur a bill because the test is one of the many preventive measures guaranteed to be free to patients under the 2010 Affordable Care Act. The ACA’s provision made medical and economic sense, encouraging Americans to use screening tools that could nip medical problems in the bud and keep patients healthy.
So when a bill for $236 arrived, Uddin — an occupational therapist familiar with the health care industry’s workings — complained to her insurer and the hospital. She even requested an independent review.
“I’m like, ‘Tell me why am I getting this bill?’” Uddin recalled in an interview. The unsatisfying explanation: The mammogram itself was covered, per the ACA’s rules, but the fee for the equipment and the facility was not.
That answer was particularly galling, she said, because, a year earlier, her “free” mammogram at the same health system had generated a bill of about $1,000 for the radiologist’s reading. Though she fought that charge (and won), this time she threw in the towel and wrote the $236 check. But then she dashed off a submission to the KFF Health News-NPR “Bill of the Month” project:
“I was really mad — it’s ridiculous,” she later recalled. “This is not how the law is supposed to work.”
The ACA’s designers might have assumed that they had spelled out with sufficient clarity that millions of Americans would no longer have to pay for certain types of preventive care, including mammograms, colonoscopies, and recommended vaccines, in addition to doctor visits to screen for disease. But the law’s authors didn’t reckon with America’s ever-creative medical billing juggernaut.
Over the past several years, the medical industry has eroded the ACA’s guarantees, finding ways to bill patients in gray zones of the law. Patients going in for preventive care, expecting that it will be fully covered by insurance, are being blindsided by bills, big and small.
The problem comes down to deciding exactly what components of a medical encounter are covered by the ACA guarantee. For example, when do conversations between doctor and patient during an annual visit for preventive services veer into the treatment sphere? What screenings are needed for a patient’s annual visit?
A healthy 30-year-old visiting a primary care provider might get a few basic blood tests, while a 50-year-old who is overweight would merit additional screening for Type 2 diabetes.
Making matters more confusing, the annual checkup itself is guaranteed to be “no cost” for women and people age 65 and older, but the guarantee doesn’t apply for men in the 18-64 age range — though many preventive services that require a medical visit (such as checks of blood pressure or cholesterol and screens for substance abuse) are covered.
No wonder what’s covered under the umbrella of prevention can look very different to medical providers (trying to be thorough) and billers (intent on squeezing more dollars out of every medical encounter) than it does to insurers (who profit from narrower definitions).
For patients, the gray zone has become a billing minefield. Here are a few more examples, gleaned from the Bill of the Month project in just the past six months:
Peter Opaskar, 46, of Texas, went to his primary care doctor last year for his preventive care visit — as he’d done before, at no cost. This time, his insurer paid $130.81 for the visit, but he also received a perplexing bill for $111.81. Opaskar learned that he had incurred the additional charge because when his doctor asked if he had any health concerns, he mentioned that he was having digestive problems but had already made an appointment with his gastroenterologist. So, the office explained, his visit was billed as both a preventive physical and a consultation. “Next year,” Opasker said in an interview, if he’s asked about health concerns, “I’ll say ‘no,’ even if I have a gunshot wound.”
Kevin Lin, a technology specialist in Virginia in his 30s, went to a new primary care provider to take advantage of the preventive care benefit when he got insurance; he had no physical complaints. He said he was assured at check-in that he wouldn’t be charged. His insurer paid $174 for the checkup, but he was billed an additional $132.29 for a “new patient visit.” He said he has made many calls to fight the bill, so far with no luck.
Finally, there’s Yoori Lee, 46, of Minnesota, herself a colorectal surgeon, who was shocked when her first screening colonoscopy yielded a bill for $450 for a biopsy of a polyp — a bill she knew was illegal. Federal regulations issued in 2022 to clarify the matter are very clear that biopsies during screening colonoscopies are included in the no-cost promise. “I mean, the whole point of screening is to find things,” she said, stating, perhaps, the obvious.
Though these patient bills defy common sense, room for creative exploitation has been provided by the complex regulatory language surrounding the ACA. Consider this from Ellen Montz, deputy administrator and director of the Center for Consumer Information and Insurance Oversight at the Centers for Medicare & Medicaid Services, in an emailed response to queries and an interview request on this subject: “If a preventive service is not billed separately or is not tracked as individual encounter data separately from an office visit and the primary purpose of the office visit is not the delivery of the preventive item or service, then the plan issuer may impose cost sharing for the office visit.”
So, if the doctor decides that a patient’s mention of stomach pain does not fall under the umbrella of preventive care, then that aspect of the visit can be billed separately, and the patient must pay?
And then there’s this, also from Montz: “Whether a facility fee is permitted to be charged to a consumer would depend on whether the facility usage is an integral part of performing the mammogram or an integral part of any other preventive service that is required to be covered without cost sharing under federal law.”
But wait, how can you do a mammogram or colonoscopy without a facility?
Unfortunately, there is no federal enforcement mechanism to catch individual billing abuses. And agencies’ remedies are weak — simply directing insurers to reprocess claims or notifying patients they can resubmit them.
In the absence of stronger enforcement or remedies, CMS could likely curtail these practices and give patients the tools to fight back by offering the sort of clarity the agency provided a few years ago regarding polyp biopsies — spelling out more clearly what comes under the rubric of preventive care, what can be billed, and what cannot.
The stories KFF Health News and NPR receive are likely just the tip of an iceberg. And while each bill might be relatively small compared with the stunning $10,000 hospital bills that have become all too familiar in the United States, the sorry consequences are manifold. Patients pay bills they do not owe, depriving them of cash they could use elsewhere. If they can’t pay, those bills might end up with debt-collection agencies and, ultimately, harm their credit score.
Perhaps most disturbing: These unexpected bills might discourage people from seeking preventive screenings that could be lifesaving, which is why the ACA deemed them “essential health benefits” that should be free.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: