How To Stay A Step Ahead Of Peripheral Artery Disease
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Far less well-known than Coronary Artery Disease, it can still result in loss of life and limb (not in that order). Fortunately, there are ways to be on your guard:
What it is
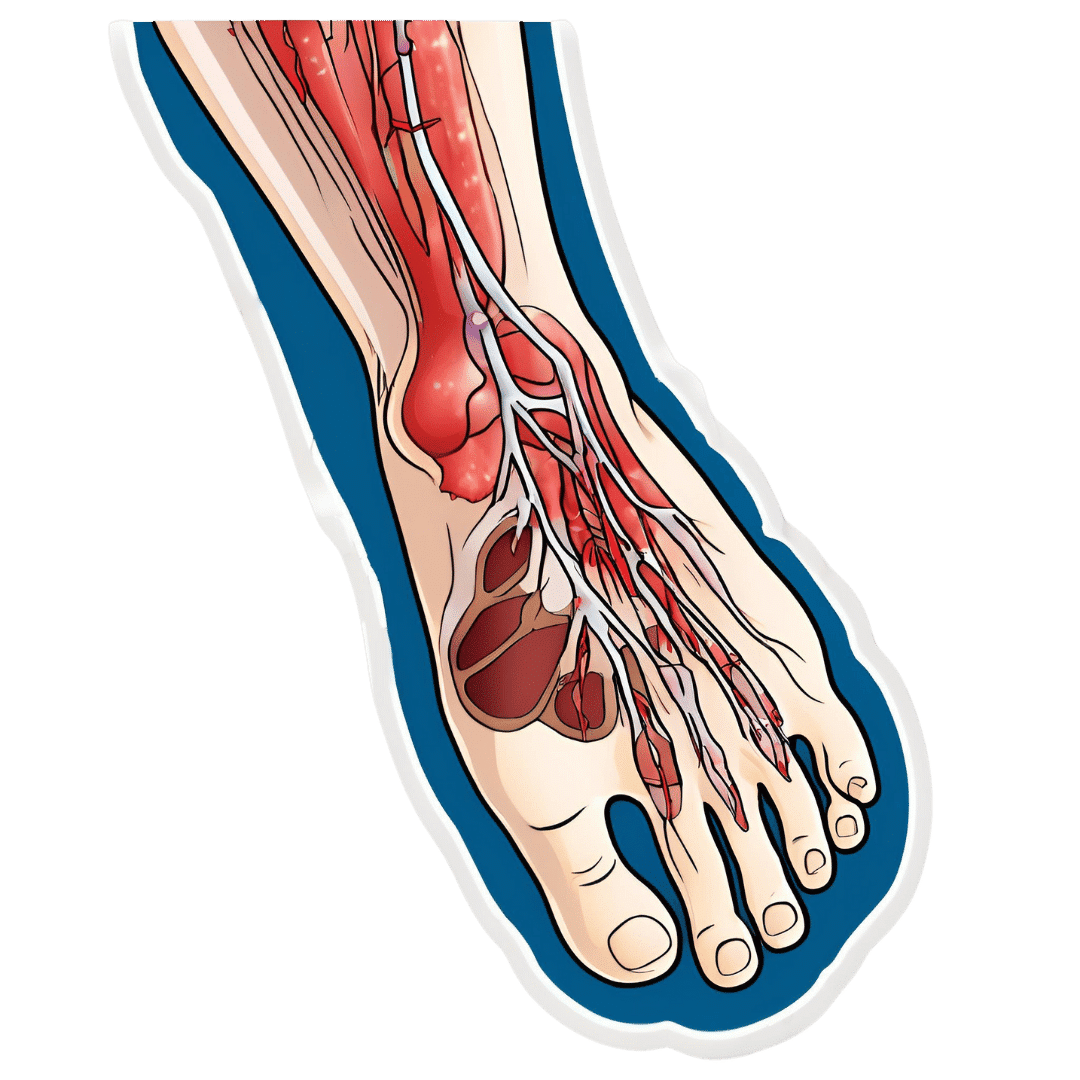
Peripheral Artery Disease (PAD) is the same thing as Coronary Artery Disease (CAD), just, in the periphery—which by definition means “outside of the heart and brain”, but in practice, it starts with the extremities. And of the extremities, it tends to start with the feet and legs, for the simple reason that if someone’s circulation is sluggish, then because of gravity, that’s where’s going to get blocked first.
In both CAD and PAD, the usual root cause is atherosclerosis, that is to say, the build-up of fatty material inside the arteries, usually commensurate to LDL (“bad”) cholesterol, especially in men (high LDL is still a predictor of cardiovascular disease in women though, just more modestly so, at least pre-menopause or in cases of treated menopause whereby HRT has returned hormones to pre-menopause levels).
See also: Demystifying Cholesterol
And for that about sex differences: His & Hers: The Hidden Complexities of Statins and Cardiovascular Disease (CVD)
Why it is
This one’s straightforward, as it’s the same things as any kind of cardiovascular disease: high blood pressure, high cholesterol, older age, obesity, smoking, drinking, diabetes, and genetic factors (so, a risk factor is: family history of heart disease).
However, while those are the main causes and/or risk factors, it absolutely can still strike other people, so it’s as well to be watch out for…
What to look out for
Many people first notice signs and symptoms that turn out to be PAD when they experience pain or numbness in the foot or feet, and/or a discoloration of the feet (especially toes), and slow wound healing.
At that stage, chances are you will need to go urgently to a specialist, and surgery is a likely necessity. With a little luck, it’ll be a minimally-invasive surgery to unblock an artery; failing that, an amputation will be in order.
At that stage, under 50% will be alive 5 years from diagnosis:
You probably want to avoid those. Good news is, you can, by catching it earlier!
What to look out for before that
The most common test for PAD is one you can do at home, but enlisting a nurse to do it for you will help ensure accurate readings. It’s called the Ankle-Brachial Index (ABI) test, and it involves comparing the blood pressure in your ankle with the blood pressure in your arm, and expressing them as a ratio.
Here’s how to do it (instructions and a video demonstration if you want it):
Do Try This At Home: ABI Test For Clogged Arteries
If you need a blood pressure monitor, by the way, here’s an example product on Amazon.
- A healthy ABI score is between 1.0 and 1.4; anything outside this range may indicate arterial problems.
- Low ABI scores (below 0.8) suggest plaque is likely obstructing blood flow
- High ABI scores (above 1.4) may indicate artery hardening
Do note also that yes, if you have plaque obstructing blood flow and hardened arteries, your scores may cancel out and give you a “healthy” score, despite your arteries being very much not healthy.
For this reason, this test can be used to raise the alarm, but not to give the “all clear”.
There are other tests that clinicians can do for you, but you can’t do at home unless you have an MRI machine, a CT scanner, an x-ray machine, a doppler-and-ultrasound machine, etc. We’ll not go into those in detail here, but ask your doctor about them if you’re concerned.
What to do about it
In the mid-to-late stages of the disease, the options are medication and surgery, respectively, but your doctor will advise about those in that eventuality.
In the early stages of the disease, the first-line recommend treatment is exercise, of which, especially walking:
Lower Extremity Peripheral Artery Disease: Diagnosis and Treatment
Given that this more often happens when someone hasn’t been walking so much, it can be a walk-rest-walk approach at first (a treadmill on a low setting can be very useful for this):
See also: Exercise Comparison Head-to-Head: Treadmill vs Road
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

An Important Way That Love Gets Eroded

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It is unusual for a honeymoon period to last forever, but some relationships fair a lot better than others. Not just in terms of staying together vs separating, but in terms of happiness and satisfaction in the relationship. What’s the secret? There are many, but here’s one of them…
Communication
In this video, the case is made for a specific aspect of communication: airing grievances.
Superficially, this doesn’t seem like a recipe for happiness, but it is one important ingredient—that it’s dangerously easy to let small grievances add up and eat away at one’s love and patience, until one day resentment outweighs attachment, and at that point, it often becomes a case of “checking out before you leave”, remaining in the relationship more due to inertia than volition.
Which, in turn, will likely start to cause resentment on the other side, and eventually things will crumble and/or explode.
In contrast, if we make sure to speak our feelings clearly (10almonds note, not in the video: we think that doing so compassionately is also important), the bad as well as the good, then it means that:
- things don’t stack up and fester (there will less likely be a “final straw” if we are regularly removing straws)
- there is an opportunity for change (in contrast, our partner would be unlikely to adjust anything to correct a problem they don’t know about)
- all but the most inclined-to-anxiety partners can rest easy, because they know that if we had a problem, we’d tell them
This is definitely only one critical aspect of communication; this video for example says nothing about actually being affectionate with one’s partner, or making sure to accept emotional bids for connection (per that story that goes “I knew my marriage was over when he wouldn’t come look at the tomatoes I grew”), but it is one worth considering—even if we at 10almonds would advise being gentle yet honest, and where possible balancing, in aggregate if not in the moment, with positive things (per Gottman’s ratio of 5:1 good moments to bad, being the magic number for marriages that “work”).
For more on why it’s so important to be able to safely air grievances, see:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Seriously Useful Communication Skills! ← this deals with some of the important gaps left by the video
Take care!
Share This Post
-

Grapes vs Strawberries – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing strawberries to grapes, we picked the strawberries.
Why?
In terms of macros, grapes have more than 2x the carbs while strawberries have more than 2x the fiber, making this category an easy win for strawberries.
In the category of vitamins, grapes have more of vitamins A, B1, B2, B6, and K, while strawberries have more of vitamins B3, B5, B9, C, and E, making for a 5:5 tie with comparable margins of difference.
Looking at minerals, grapes have more potassium and manganese, while strawberries have more calcium, copper, iron, magnesium, phosphorus, selenium, and zinc. A clear win for strawberries here.
When it comes to polyphenols, both of these fruits are abundant in many polyphenols, but it might interest you to know that strawberries have slightly more resveratrol than red/black grapes! Still, it’s close, and there are many other polyphenols in both, and honestly we’re calling this category a tie.
Adding up the sections makes for a compelling overall win for strawberries, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
Can We Drink To Good Health? ← while there are polyphenols such as resveratrol in red wine that per se would boost heart health, there’s so little per glass that you may need 100–1000 glasses per day to get the dosage that provides benefits in mouse studies.
If you’re not a mouse, you might even need more than that!
To this end, many people prefer resveratrol supplementation ← link is to an example product on Amazon, but there are plenty more so feel free to shop around 😎
Enjoy!
Share This Post
-

Feel Great, Lose Weight – by Dr. Rangan Chatterjee
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We all know that losing weight sustainably tends to be harder than simply losing weight. We know that weight loss needs to come with lifestyle change. But how to get there?
One of the biggest problems that we might face while trying to lose weight is that our “metabolic thermostat” has got stuck at the wrong place. Trying to move it just makes our bodies think we are starving, and everything gets even worse. We can’t even “mind over matter” our way through it with willpower, because our bodies will do impressive things on a cellular level in an attempt to save us… Things that are as extraordinary as they are extraordinarily unhelpful.
Dr. Rangan Chatterjee is here to help us cut through that.
In this book, he covers how our metabolic thermostat got stuck in the wrong place, and how to gently tease it back into a better position.
Some advices won’t be big surprises—go for a whole foods diet, avoiding processed food, for example. Probably not a shocker.
Others are counterintuitive, but he explains how they work—exercising less while moving more, for instance. Sounds crazy, but we assure you there’s a metabolic explanation for it that’s beyond the scope of this review. And there’s plenty more where that came from, too.
Bottom line: if your weight has been either slowly rising, or else very stable but at a higher point than you’d like, Dr. Chatterjee can help you move the bar back to where you want it—and keep it there.
Share This Post
-

Cognitive Enhancement Without Drugs
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cognitive Enhancement Without Drugs

This is Elizabeth Ricker. She’s a Harvard-and-MIT-trained neuroscientist and researcher, who now runs the “Citizen Science” DIY-neurohacking organization, NeuroEducate.
Sounds fun! What’s it about?
The philosophy that spurs on her research and practice can be summed up as follows:
❝I’m not going to leave my brain up to my doctor or [anyone else]… My brain is my own responsibility, and I’m going to do the best that I can to optimize it❞
Her goal is not just to optimize her own brain though; she wants to make the science accessible to everyone.
What’s this about Citizen Science?
“Citizen Science” is the idea that while there’s definitely an important role in society for career academics, science itself should be accessible to all. And, not just the conclusions, but the process too.
This can take the form of huge experiments, often facilitated these days by apps where we opt-in to allow our health metrics (for example) to be collated with many thousands of others, for science. It can also involve such things as we talked about recently, getting our own raw genetic data and “running the numbers” at home to get far more comprehensive and direct information than the genetic testing company would ever provide us.
For Ricker, her focus is on the neuroscience side of biohacking, thus, neurohacking.
I’m ready to hack my brain! Do I need a drill?
Happily not! Although… Bone drills for the skull are very convenient instruments that make it quite hard to go wrong even with minimal training. The drill bit has a little step/ledge partway down, which means you can only drill through the thickness of the skull itself, before the bone meeting the wider part of the bit stops you from accidentally drilling into the brain. Still, please don’t do this at home.
What you can do at home is a different kind of self-experimentation…
If you want to consider which things are genuinely resulting in cognitive enhancement and which things are not, you need to approach the matter like a scientist. That means going about it in an organized fashion, and recording results.
There are several ways cognitive enhancement can be measured, including:
- Learning and memory
- Executive function
- Emotional regulation
- Creative intelligence
Let’s look at each of them, and what can be done. We don’t have a lot of room here; we’re a newsletter not a book, but we’ll cover one of Ricker’s approaches for each:
Learning and memory
This one’s easy. We’re going to leverage neuroplasticity (neurons that fire together, wire together!) by simple practice, and introduce an extra element to go alongside your recall. Perhaps a scent, or a certain item of clothing. Tell yourself that clinical studies have shown that this will boost your recall. It’s true, but that’s not what’s important; what’s important is that you believe it, and bring the placebo effect to bear on your endeavors.
You can test your memory with word lists, generated randomly by AI, such as this one:
You’ll soon find your memory improving—but don’t take our word for it!
Executive function
Executive function is the aspect of your brain that tells the other parts how to work, when to work, and when to stop working. If you’ve ever spent 30 minutes thinking “I need to get up” but you were stuck in scrolling social media, that was executive dysfunction.
This can be trained using the Stroop Color and Word Test, which shows you words, specifically the names of colors, which will themselves be colored, but not necessarily in the color the word pertains to. So for example, you might be shown the word “red”, colored green. Your task is to declare either the color of the word only, ignoring the word itself, or the meaning of the word only, ignoring its appearance. It can be quite challenging, but you’ll get better quite quickly:
The Stroop Test: Online Version
Emotional Regulation
This is the ability to not blow up angrily at the person with whom you need to be diplomatic, or to refrain from laughing when you thought of something funny in a sombre situation.
It’s an important part of cognitive function, and success or failure can have quite far-reaching consequences in life. And, it can be trained too.
There’s no online widget for this one, but: when and if you’re in a position to safely* do so, think about something that normally triggers a strong unwanted emotional reaction. It doesn’t have to be something life-shattering, but just something that you feel in some way bad about. Hold this in your mind, sit with it, and practice mindfulness. The idea is to be able to hold the unpleasant idea in your mind, without becoming reactive to it, or escaping to more pleasant distractions. Build this up.
*if you perchance have PTSD, C-PTSD, or an emotional regulation disorder, you might want to talk this one through with a qualified professional first.
Creative Intelligence
Another important cognitive skill, and again, one that can be cultivated and grown.
The trick here is volume. A good, repeatable test is to think of a common object (e.g. a rock, a towel, a banana) and, within a time constraint (such as 15 minutes) list how many uses you can think of for that item.
Writer’s storytime: once upon a time, I was sorting through an inventory of medical equipment with a colleague, and suggested throwing out our old arterial clamps, as we had newer, better ones—in abundance. My colleague didn’t want to part with them, so I challenged him “Give me one use for these, something we could in some possible world use them for that the new clamps don’t do better, and we’ll keep them”. He said “Thumbscrews”, and I threw my hands up in defeat, saying “Fine!”, as he had technically fulfilled my condition.
What’s the hack to improve this one? Just more volume. Creativity, as it turns out, isn’t something we can expend—like a muscle, it grows the more we use it. And because the above test is repeatable (with different objects), you can track your progress.
And if you feel like using your grown creative muscle to write/paint/compose/etc your magnum opus, great! Or if you just want to apply it to the problem-solving of everyday life, also great!
In summary…
Our brain is a wonderful organ with many functions. Society expects us to lose these as we get older, but the simple, scientific truth is that we can not only maintain our cognitive function, but also enhance and grow it as we go.
Want to know more from today’s featured expert?
You might enjoy her book, “Smarter Tomorrow”, which we reviewed back in March
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
The High-Protein, High-Fiber Superfood Salad You’ll Want To Enjoy Daily
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This salad from Nisha Vora at Rainbow Plant Life has 30g protein and takes minutes to prepare, while being tasty enough to look forward to eating each day:
Easy preparation
Prepare the toppings first; you can do a week’s in advance at once:
- Roasted chickpeas:
- Drain, rinse, and dry two cans of chickpeas.
- Toss with olive oil, salt, and pepper.
- Roast at 425°F for 30–35 minutes.
- Roasted walnuts:
- Chop and toss with olive oil, salt, and pepper.
- Roast at 350°F for 12 minutes after chickpeas finish.
As for the salad base:
- Kale:
- Remove tough stems, slice thinly.
- Wash and massage with lemon juice and salt to soften.
- Cabbage:
- Slice thinly with a knife or mandolin.
- Store in a sealed bag in the fridge for up to a week.
Red wine vinaigrette dressing:
- Key ingredients: red wine vinegar, lemon juice, red pepper flakes, garlic, olive oil.
- Can be stored in the fridge for up to 10 days.
Putting it all together:
- Toss kale and cabbage with vinaigrette by hand.
- Add roasted chickpeas and walnuts for crunch.
- Include a protein source like tofu (store-bought curry tofu recommended).
- Mix in fresh vegetables like grated carrots, sliced bell peppers, or beets.
- Add extras like sauerkraut, avocado, pickled onions, and such.
- Top with fresh herbs (she recommends parsley, basil, or dill).
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
21 Most Beneficial Polyphenols & What Foods Have Them
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
- Roasted chickpeas:
-
Here’s how to help protect your family from norovirus
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What you need to know
- Norovirus is a very contagious infection that causes vomiting and diarrhea.
- The best way to help protect against norovirus is to wash your hands often with soap and warm water, since hand sanitizer may not be effective at killing the virus.
- If someone in your household has symptoms of norovirus, isolate them away from others, watch for signs of dehydration, and take steps to help prevent it from spreading.
If you feel like everyone is sick right now, you’re not alone. Levels of respiratory illnesses like COVID-19, flu, and RSV remain remain high in many states, and the U.S. is also battling a wave of norovirus, one of several viruses that cause a very contagious infection of the stomach and intestines.
Although norovirus infections are more common during the colder months—it’s also called the “winter vomiting disease”—the virus can spread at any time. Right now, however, cases have more than doubled since last year’s peak.
Read on to learn about the symptoms of norovirus, how it spreads, and what to do if someone in your household gets sick.
What are the symptoms of norovirus?
Norovirus is a very contagious infection that causes vomiting and diarrhea, which typically begins 12 to 48 hours after exposure to the virus. Additional symptoms may include stomach pain, body aches, headaches, and a fever. Norovirus typically resolves within three days, but people who are infected may still be contagious for up to two days after symptoms resolve.
Norovirus may cause dehydration, or a dangerous loss of fluids, especially in young children and older adults. See a health care provider if you or someone in your household shows signs of dehydration, which may include decreased urination, dizziness, a dry mouth and throat, sleepiness, and crying without tears.
How can you help protect against norovirus?
You can get norovirus if you have close contact with someone who is infected, touch a contaminated surface and then touch your mouth or nose, or consume contaminated food or beverages.
The best way to help protect yourself and others against norovirus is to wash your hands often with soap and warm water, since hand sanitizer may not be effective at killing the virus. Other ways to help protect yourself may include cooking food thoroughly and washing fruits and vegetables before eating them.
You can get sick with norovirus even if you’ve had it before, since there are many different strains.
How can families help protect against the spread of norovirus at home?
If someone in your household has symptoms of norovirus, isolate them away from others and watch for signs of dehydration. If you are sick with norovirus, do not prepare food for others in your household and use a separate bathroom, if possible.
When cleaning up after someone who has norovirus, wear rubber, latex, or nitrile gloves. Then wash your hands thoroughly.
Clean surfaces using a solution containing five to 25 tablespoons of bleach (that’s 12.5 fluid ounces, or just over ¾ cup), per gallon of water. Leave the bleach-water mix on surfaces for at least five minutes before wiping it off.
For more information, talk to your health care provider.
This article first appeared on Public Good News and is republished here under a Creative Commons license.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: