Healing After Loss – by Martha Hickman
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Mental health is also just health, and this book’s about an underexamined area of mental health. We say “underexamined”, because for something that affects almost everyone sooner or later, there’s not nearly so much science being done about it as other areas of mental health.
This is not a book of science per se, but it is a very useful one. The format is:
Each calendar day of the year, there’s a daily reflection, consisting of:
- A one-liner insight about grief, quoted from somebody
- A page of thoughts about this
- A one-liner summary, often formulated as a piece of advice
The book is not religious in content, though the author does occasionally make reference to God, only in the most abstract way that shouldn’t be offputting to any but the most stridently anti-religious readers.
Bottom line: if this is a subject near to your heart, then you will almost certainly benefit from this daily reader.
Click here to check out Healing After Loss, and indeed heal after loss
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Red Cabbage vs White Cabbage – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing red cabbage to white cabbage, we picked the red.
Why?
Perhaps you guessed this one, based on the “darker and/or more colorful foods are usually more nutritionally dense” dictum. That’s not always true, by the way, but it is a good rule of thumb and it is correct here. In the case of cabbages, each type is a nutritional powerhouse, but red does beat white:
In terms of macros, they’re quite comparable. They’re both >90% water with just enough other stuff (carbs, fiber, protein) to hold them together, and the “other stuff” in question is quite similarly proportioned in both cases. Within the carbs, even the sugar breakdown is similar. There are slight differences, but the differences are not only tiny, but also they balance out in any case.
When it comes to vitamins, as you might expect, the colorful red cabbage does better with more of vitamins A, B1, B2, B3, B6, C, and choline, while white has more of vitamins B5, B9, E, and K. So, a 7:4 win for red.
In the category of minerals, it’s even more polarized; red cabbage has more calcium, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc. On the other hand, white contains a tiny amount more copper.
In short, both are great (red just makes white look bad by standing next to it, but honestly, white has lots of all those same things too, just not quite as much as red), and this writer will continue to use white when making her favorite shchi, but if you’re looking for the most nutritionally dense option, it’s red.
Want to learn more?
You might like to read:
Enjoy Bitter Foods For Your Heart & Brain
Take care!
Share This Post
-

What You Don’t Know Can Kill You
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Knowledge Is Power!

This is Dr. Simran Malhotra. She’s triple board-certified (in lifestyle medicine, internal medicine, and palliative care), and is also a health and wellness coach.
What does she want us to know?
Three things:
Wellness starts with your mindset
Dr. Malhotra shifted her priorities a lot during the initial and perhaps most chaotic phase of the COVID pandemic:
❝My husband, a critical care physician, was consumed in the trenches of caring for COVID patients in the ICU. I found myself knee-deep in virtual meetings with families whose loved ones were dying of severe COVID-related illnesses. Between the two of us, we saw more trauma, suffering, and death, than we could have imagined.
The COVID-19 pandemic opened my eyes to how quickly life can change our plans and reinforced the importance of being mindful of each day. Harnessing the power to make informed decisions is important, but perhaps even more important is focusing on what is in our control and taking action, even if it is the tiniest step in the direction we want to go!❞
~ Dr. Simran Malhotra
We can only make informed decisions if we have good information. That’s one of the reasons we try to share as much information as we can each day at 10almonds! But a lot will always depend on personalized information.
There are one-off (and sometimes potentially life-saving) things like health genomics:
The Real Benefit Of Genetic Testing
…but also smaller things that are informative on an ongoing basis, such as keeping track of your weight, your blood pressure, your hormones, and other metrics. You can even get fancy:
Track Your Blood Sugars For Better Personalized Health
Lifestyle is medicine
It’s often said that “food is medicine”. But also, movement is medicine. Sleep is medicine. In short, your lifestyle is the most powerful medicine that has ever existed.
Lifestyle encompasses very many things, but fortunately, there’s an “80:20 rule” in play that simplifies it a lot because if you take care of the top few things, the rest will tend to look after themselves:
These Top Few Things Make The Biggest Difference To Overall Health
Gratitude is better than fear
If we receive an unfavorable diagnosis (and let’s face it, most diagnoses are unfavorable), it might not seem like something to be grateful for.
But it is, insofar as it allows us to then take action! The information itself is what gives us our best chance of staying safe. And if that’s not possible e.g. in the worst case scenario, a terminal diagnosis, (bearing in mind that one of Dr. Malhotra’s three board certifications is in palliative care, so she sees this a lot), it at least gives us the information that allows us to make the best use of whatever remains to us.
See also: Managing Your Mortality
Which is very important!
…and/but possibly not the cheeriest note on which to end, so when you’ve read that, let’s finish today’s main feature on a happier kind of gratitude:
How To Get Your Brain On A More Positive Track (Without Toxic Positivity)
Want to hear more from Dr. Malhotra?
Showing how serious she is about how our genes do not determine our destiny and knowledge is power, here she talks about her “previvor’s journey”, as she puts it, with regard to why she decided to have preventative cancer surgery in light of discovering her BRCA1 genetic mutation:
Click Here If The Embedded Video Doesn’t Load Automatically
Take care!
Share This Post
-
Debunking the myth that vaccines cause autism
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The myth that autism is linked to childhood vaccines first appeared in a 1998 study by British physician Dr. Andrew Wakefield. The study was later retracted, and Wakefield was discredited. But nearly three decades after the study’s publication, the myth persists, championed by activists, political leaders, and even potential health officials.
There is overwhelming evidence that there is no link between vaccines and autism. “No one has any real or solid evidence that vaccines cause autism,” says Catherine Lord, a psychologist and autism researcher at the University of California, Los Angeles.
Here are just some of the many reasons that we know vaccines don’t cause autism.
The Wakefield study has been thoroughly discredited
In 1998, the Lancet published a study describing a small group of children who reportedly had bowel inflammation and developed autism within a month of getting the measles, mumps, and rubella (MMR) vaccine. The study proposed that the vaccination triggered bowel inflammation and developmental delays, including autism. Lead author Andrew Wakefield coined the term “autistic enterocolitis” to describe the condition he and his colleagues claimed to have discovered.
The study received significant media attention and immediate criticism from scientists, who pointed out the study’s small size, lack of controls, and insufficient evidence to support its conclusions.
Subsequent research published over the next few years refuted Wakefield’s findings. A 1999 Lancet study found no link between autism and the MMR vaccine, and a 2001 study found no evidence of a link or the existence of so-called autistic enterocolitis.
In 2010, the Lancet finally retracted Wakefield’s fraudulent study, noting that “several elements” of the study were “incorrect” and that the experiments carried out on children had not been approved by an ethics board. The journal’s editor called the paper’s conclusions “utterly false.”
A few months later, Wakefield was stripped of his medical license by the United Kingdom’s General Medical Council. The council deemed Wakefield “dishonest and irresponsible” and concluded that he conducted unethical experiments on children.
The committee’s investigation also revealed that, less than a year before he published his study claiming that the MMR vaccine was linked to bowel inflammation that triggered autism, Wakefield filed a patent for a standalone measles vaccine and inflammatory bowel disease treatment.
Thimerosal was removed from childhood vaccines in 2001—with no effect on autism rates
A 2003 study published by a conservative group known for promoting anti-science myths—including that HIV doesn’t cause AIDS—first proposed that the preservative thimerosal in childhood vaccines is linked to autism. This supposed link was subsequently disproven.
Thimerosal is added in small amounts to some vaccines to prevent dangerous bacterial and fungal contamination. The substance contains ethylmercury, a form of mercury that the body quickly and safely processes in small doses.
Ethylmercury is different from methylmercury, a far more dangerous form of mercury that is toxic at low doses. By contrast, the small amount of thimerosal in some vaccines is harmless to humans and is equal to the amount of mercury in a can of tuna.
The preservative was removed from childhood vaccines as a precautionary measure in 2001. With the exception of some flu shots, no childhood vaccine contains the preservative and hasn’t for more than two decades. Autism rates have not decreased as a result of thimerosal being removed from childhood immunization vaccines. While some types of the annual flu vaccine contain thimerosal, you can get one without it.
Extensive research also shows that neither thimerosal nor methylmercury at any dose is linked to autism. A 2008 study of statewide California data found that autism rates “increased consistently for children born from 1989 through 2003, inclusive of the period when exposure to [thimerosal-containing vaccines] has declined.”
Autism rates are the same in vaccinated and unvaccinated children
Vaccine opponents often falsely claim that vaccinated children are more likely than unvaccinated children to develop autism. Decades of research disprove this false claim.
A 2002 analysis of every child born in Denmark over eight years found that children who received MMR vaccines were no more likely to be diagnosed with autism than unvaccinated children.
A 2015 study of over 95,000 U.S. siblings found that MMR vaccination is not associated with increased autism diagnosis. This was true even among the siblings of children with autism, who are seven times more likely to develop autism than children without an autistic sibling.
And a 2018 study found some evidence that children with autism—and their siblings—were more likely to be unvaccinated or under-vaccinated than children without autism.
Vaccination also has no impact on autism rates at the population level, regardless of the age at which children get vaccinated.
“In comparing countries that have different timing and levels of vaccination … there’s no difference in autism,” says Lord. “You can look at different countries with different rates of autism, and there’s no relationship between the rates of autism and vaccinations.”
Countries such as Taiwan, Tunisia, Turkey, and Morocco, which have some of the world’s lowest autism rates, have childhood immunization rates that are nearly identical to countries with the highest autism rates, including Sweden, Japan, Brunei, and Singapore.
Improved awareness and diagnosis play a role in rising autism rates
Autism was first described in 1911 when it was considered to be a form of severe schizophrenia. Over a century later, our understanding of autism has changed drastically, as have diagnostic standards.
A 2013 scientific article describing how medical and social perceptions of autism have evolved explains that “the diagnoses of schizophrenia, psychosis and autism in children were largely interchangeable during the 1940s and 1950s.” Beginning in the 1960s, methods of diagnosing autism improved, “increasing the number of children who were considered to display autistic traits.”
The autism diagnosis was changed to autism spectrum disorder in 2013. “This category is now very broad, which was an intentional choice to help provide services to the greatest number of people who might need them,” writes Gideon Meyerowitz-Katz, an epidemiologist and creator of the popular Health Nerd blog.
“Rather than the severe intellectual disability of the 1940s and 50s, [autism spectrum disorder] is a group of behaviours that can be any severity as long as they are persistent and impact people’s daily functioning in a significant way.”
For more information about autism, talk to your health care provider.
This article first appeared on Public Good News and is republished here under a Creative Commons license.
Share This Post


Related Posts
-
How Does One Test Acupuncture Against Placebo Anyway?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Pinpointing The Usefulness Of Acupuncture

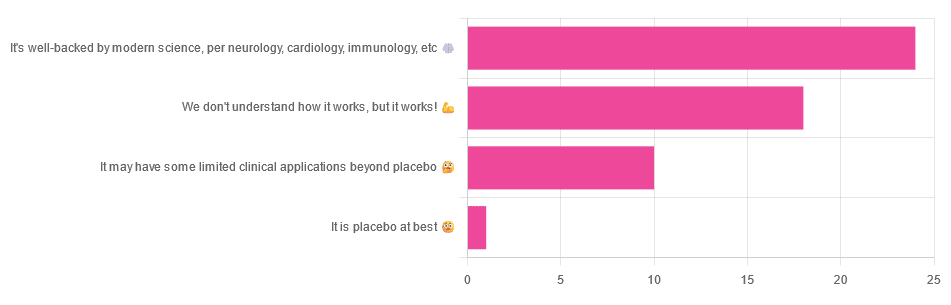
We asked you for your opinions on acupuncture, and got the above-depicted, below-described, set of answers:
- A little under half of all respondents voted for “It’s well-backed by modern science, per neurology, cardiology, immunology, etc”
- Slightly fewer respondents voted for “We don’t understand how it works, but it works!”
- A little under a fifth of respondents voted for “It may have some limited clinical applications beyond placebo”
- One (1) respondent voted for for “It’s placebo at best”
When we did a main feature about homeopathy, a couple of subscribers wrote to say that they were confused as to what homeopathy was, so this time, we’ll start with a quick definition first.
First, what is acupuncture? For the convenience of a quick definition so that we can move on to the science, let’s borrow from Wikipedia:
❝Acupuncture is a form of alternative medicine and a component of traditional Chinese medicine in which thin needles are inserted into the body.
Acupuncture is a pseudoscience; the theories and practices of TCM are not based on scientific knowledge, and it has been characterized as quackery.❞
Now, that’s not a promising start, but we will not be deterred! We will instead examine the science itself, rather than relying on tertiary sources like Wikipedia.
It’s worth noting before we move on, however, that there is vigorous debate behind the scenes of that article. The gist of the argument is:
- On one side: “Acupuncture is not pseudoscience/quackery! This has long been disproved and there are peer-reviewed research papers on the subject.”
- On the other: “Yes, but only in disreputable quack journals created specifically for that purpose”
The latter counterclaim is a) potentially a “no true Scotsman” rhetorical ploy b) potentially true regardless
Some counterclaims exhibit specific sinophobia, per “if the source is Chinese, don’t believe it”. That’s not helpful either.
Well, the waters sure are muddy. Where to begin? Let’s start with a relatively easy one:
It may have some clinical applications beyond placebo: True or False?
True! Admittedly, “may” is doing some of the heavy lifting here, but we’ll take what we can get to get us going.
One of the least controversial uses of acupuncture is to alleviate chronic pain. Dr. Vickers et al, in a study published under the auspices of JAMA (a very respectable journal, and based in the US, not China), found:
❝Acupuncture is effective for the treatment of chronic pain and is therefore a reasonable referral option. Significant differences between true and sham acupuncture indicate that acupuncture is more than a placebo.
However, these differences are relatively modest, suggesting that factors in addition to the specific effects of needling are important contributors to the therapeutic effects of acupuncture❞
Source: Acupuncture for Chronic Pain: Individual Patient Data Meta-analysis
If you’re feeling sharp today, you may be wondering how the differences are described as “significant” and “relatively modest” in the same text. That’s because these words have different meanings in academic literature:
- Significant = p<0.05, where p is the probability of the achieved results occurring randomly
- Modest = the differences between the test group and the control group were small
In other words, “significant modest differences” means “the sample sizes were large, and the test group reliably got slightly better results than placebo”
We don’t understand how it works, but it works: True or False
Broadly False. When it works, we generally have an idea how.
Placebo is, of course, the main explanation. And even in examples such as the above, how is placebo acupuncture given?
By inserting acupuncture needles off-target rather than in accord with established meridians and points (the lines and dots that, per Traditional Chinese Medicine, indicate the flow of qi, our body’s vital energy, and welling-points of such).
So, if a patient feels that needles are being inserted randomly, they may no longer have the same confidence that they aren’t in the control group receiving placebo, which could explain the “modest” difference, without there being anything “to” acupuncture beyond placebo. After all, placebo works less well if you believe you are only receiving placebo!
Indeed, a (Korean, for the record) group of researchers wrote about this—and how this confounding factor cuts both ways:
❝Given the current research evidence that sham acupuncture can exert not only the originally expected non-specific effects but also sham acupuncture-specific effects, it would be misleading to simply regard sham acupuncture as the same as placebo.
Therefore, researchers should be cautious when using the term sham acupuncture in clinical investigations.❞
Source: Sham Acupuncture Is Not Just a Placebo
It’s well-backed by modern science, per neurology, cardiology, immunology, etc: True or False?
False, for the most part.
While yes, the meridians and points of acupuncture charts broadly correspond to nerves and vasculature, there is no evidence that inserting needles into those points does anything for one’s qi, itself a concept that has not made it into Western science—as a unified concept, anyway…
Note that our bodies are indeed full of energy. Electrical energy in our nerves, chemical energy in every living cell, kinetic energy in all our moving parts. Even, to stretch the point a bit, gravitational potential energy based on our mass.
All of these things could broadly be described as qi, if we so wish. Indeed, the ki in the Japanese martial art of aikido is the latter kinds; kinetic energy and gravitational potential energy based on our mass. Same goes, therefore for the ki in kiatsu, a kind of Japanese massage, while the ki in reiki, a Japanese spiritual healing practice, is rather more mystical.
The qi in Chinese qigong is mostly about oxygen, thus indirectly chemical energy, and the electrical energy of the nerves that are receiving oxygenated blood at higher or lower levels.
On the other hand, the efficacy of the use of acupuncture for various kinds of pain is well-enough evidenced. Indeed, even the UK’s famously thrifty NHS (that certainly would not spend money on something it did not find to work) offers it as a complementary therapy for some kinds of pain:
❝Western medical acupuncture (dry needling) is the use of acupuncture following a medical diagnosis. It involves stimulating sensory nerves under the skin and in the muscles.
This results in the body producing natural substances, such as pain-relieving endorphins. It’s likely that these naturally released substances are responsible for the beneficial effects experienced with acupuncture.❞
Source: NHS | Acupuncture
Meanwhile, the NIH’s National Cancer Institute recommends it… But not as a cancer treatment.
Rather, they recommend it as a complementary therapy for pain management, and also against nausea, for which there is also evidence that it can help.
Frustratingly, while they mention that there is lots of evidence for this, they don’t actually link the studies they’re citing, or give enough information to find them. Instead, they say things like “seven randomized clinical trials found that…” and provide links that look reassuring until one finds, upon clicking on them, that it’s just a link to the definition of “randomized clinical trial”:
Source: NIH | Nactional Cancer Institute | Acupuncture (PDQ®)–Patient Version
However, doing our own searches finds many studies (mostly in specialized, potentially biased, journals such as the Journal of Acupuncture and Meridian Studies) finding significant modest outperformance of [what passes for] placebo.
Sometimes, the existence of papers with promising titles, and statements of how acupuncture might work for things other than relief of pain and nausea, hides the fact that the papers themselves do not, in fact, contain any evidence to support the hypothesis. Here’s an example:
❝The underlying mechanisms behind the benefits of acupuncture may be linked with the regulation of the hypothalamic-pituitary-gonadal (adrenal) axis and activation of the Wnt/β-catenin and OPG/RANKL/RANK signaling pathways.
In summary, strong evidence may still come from prospective and well-designed clinical trials to shed light on the potential role of acupuncture in preserving bone loss❞
Source: Acupuncture for Osteoporosis: a Review of Its Clinical and Preclinical Studies
So, here they offered a very sciencey hypothesis, and to support that hypothesis, “strong evidence may still come”.
“We must keep faith” is not usually considered evidence worthy of inclusion in a paper!
PS: the above link is just to the abstract, because the “Full Text” link offered in that abstract leads to a completely unrelated article about HIV/AIDS-related cryptococcosis, in a completely different journal, nothing to do with acupuncture or osteoporosis).
Again, this is not the kind of professionalism we expect from peer-reviewed academic journals.
Bottom line:
Acupuncture reliably performs slightly better than sham acupuncture for the management of pain, and may also help against nausea.
Beyond placebo and the stimulation of endorphin release, there is no consistently reliable evidence that is has any other discernible medical effect by any mechanism known to Western science—though there are plenty of hypotheses.
That said, absence of evidence is not evidence of absence, and the logistical difficulty of testing acupuncture against placebo makes for slow research. Maybe one day we’ll know more.
For now:
- If you find it helps you: great! Enjoy
- If you think it might help you: try it! By a licensed professional with a good reputation, please.
- If you are not inclined to having needles put in you unnecessarily: skip it! Extant science suggests that at worst, you’ll be missing out on slight relief of pain/nausea.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Antioxidant Matcha Snack Bars
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The antioxidants in this come not just from the matcha, but also the cacao nibs and chocolate, as well as lots of nutrients from the hazelnuts and cashews. If you’re allergic to nuts, we’ll give you substitutions that will change the nutritional profile (and flavor), but still work perfectly well and be healthy too.
You will need
For the base:
- ⅔ cup roasted hazelnuts (if allergic, substitute dessicated coconut)
- ⅔ cup chopped dates
For the main part:
- 1 cup raw cashews (if allergic, substitute raw coconut, chopped)
- ½ cup almond milk (or your preferred milk of any kind)
- ½ cup cacao nibs
- 2 tbsp lime juice
- 1 tbsp matcha powder
- 1 tbsp maple syrup (omit if you don’t care for sweetness)
For the topping (optional):
- 2oz dark chocolate, melted (and if you like, tempered—but this isn’t necessary; it’ll just make it glossier if you do)
- Spare cacao nibs, chopped nuts, or anything else you might want on there
Method
(we suggest you read everything at least once before doing anything)
1) Blend the base ingredients in a food processor until it has a coarse sticky texture, but isn’t yet a paste or dough.
2) Line a cake pan with baking paper and spread the base mix on the base; press it down to compact it a little and ensure it is flat. If there’s room, put this in the freezer while you do the next bit. If not, the fridge will suffice.
3) Blend the main part ingredients apart from the cacao nibs, until smooth. Stir in the cacao nibs with a spoon.
4) Spread the main part evenly over the base, and allow everything you’ve built (in this recipe, not in life in general) to chill in the fridge for at least 4 hours.
5) Cut it into blocks of the size and shape you want to eat them, and (if adding the optional topping) separate the blocks slightly from each other, before drizzling with the chocolate topping. Put it back in the fridge to cool this too; an hour should be sufficient.
6) Serve!

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Which Tea Is Best, By Science?
- Which Plant Milk?
- Why You Should Diversify Your Nuts!
- Cashew Nuts vs Coconut – Which is Healthier?
- Cacao vs Carob – Which is Healthier?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How To Do HIIT (Without Wrecking Your Body)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How To Do HIIT (Without Wrecking Your Body)
High-Intensity Interval Training, henceforth “HIIT”, is a well-researched and well-evidenced approach to exercise that gives powerful health benefits.
Specifically, health benefits that we don’t get from moderate exercise (as important as that is too) or endurance training.
Super-quick overview of the benefits first:
- Burns more calories than other forms of exercise
- Boosts your metabolic rate for hours afterwards
- …which means it actually works* for fat loss
- Reduces blood pressure (unless already healthy)
- Can promote muscle growth (depends on other factors)
*remember that most forms of exercise aren’t very good for fat loss, because our metabolism will slow afterwards to compensate. So HIIT flipping this one is quite a big deal.
What actually is it?
HIIT means exercise sessions in which one alternates between high intensity “maximum effort” bursts, and short recovery periods during which more moderate exercise is performed.
An example for runners could be switching between sprinting or jogging, changing mode each time one passes a street light.
❝A total of only two minutes of sprint interval exercise was sufficient to elicit similar responses as 30 minutes of continuous moderate intensity aerobic exercise❞
What did you mean about not wrecking your body? Is that… Likely?
Hopefully not, but it’s a barrier to some! We are not all twenty-something college athletes, after all, and our bodies aren’t always as durable as they used to be.
HIIT relies on intense exercise and short recovery periods, but what if our bodies are not accustomed to intense exercise, and need longer recovery periods? Can we still get the same benefits?
The trick is not to change the intensity or the recovery periods, but the exercise itself.
For HIIT to work the “intense” part has to be best-effort or approaching such. That part’s not negotiable. The recovery periods can be stretched a bit if you need to, but with the right tweaks, you ideally won’t have to do that.
Great! How?
First, note that you can do resistance interval training without impact. For example, if you crank up the resistance on an exercise bike or similar machine, you will be doing resistance training along with your cardio, and you’ll be doing it without the impact on your joints that you would if out pounding the pavement on foot.
(Running is fine if your body is used to it, but please don’t make HIIT your first running exercise in a decade)
Second, consider your environment. That exercise bike? You can get off it any time and you’re already at home (or perhaps your gym, with your car outside). Not so if you took up mountain biking or road racing.
Third, go for what is gentle in motion, even if it’s not resistance work per se. Swimming is a fabulous option for most people, and can absolutely be done with HIIT principles. Since vision is often obscured while swimming, counting strokes can be a good way to do HIIT. For example, ten strokes max effort, ten strokes normal, repeat. Do make sure you are aware of where the end of the pool is, though!
Fourth, make it fun! Ok, this one’s not about the safety quite so much, but it is about sustainability, and that’s critical for practical purposes too. You will only continue an exercise routine that you enjoy, after all.
- Could you curate a musical playlist that shifts tempo to cue your exercise mode intervals?
- Could you train with an exercise partner? Extra fun if this has a “relay race” feel to it, i.e. when one person completes a high intensity interval, the other person must now begin theirs.
Need some pointers getting started?
There are a lot of HIIT apps out there, so you can just search for that on your device of choice.
But!
We at 10almonds have recommended 7-Minute Workout before, which is available for iOS and for Android, and we stand by that as a great starting choice.
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: