Hack Your Hunger
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When it comes to dealing with hunger, a common-sense way of dealing with it is “eat something”. However, many people find that they then eat the wrong things, in the wrong quantities, and end up in a cycle of overeating and being hungry.
If this gets to the extreme, it can turn into a full-blown eating disorder:
Eating Disorders: More Varied (And Prevalent) Than People Think
…and even in more moderate presentations, the cycle of hunger and overeating is not great for the health. So, how to avoid that?
Listen to your body (but: actually listen)
Your body says: we’re running a little low on glycogen reserves so our energy’s going to start suffering in a few hours if we don’t eat some fruit, kill something and eat its fatty organs, or perhaps find some oily nuts.
You hear: eat something bright and sugary, shout at the dog, eat some fried food, got it!
Your body says: our water balance is a little off, we could do with some sodium, potassium, and perhaps some phosphorus to correct it.
You hear: eat something salty, got it, potato chips coming right up!
…and so on. Now, we know 10almonds readers are quite a health-conscious readership, so perhaps your responses are not quite like that. But the take-away point is still important: we need to listen to the whole message, and give the body what it actually needs, not what will just shut the message off the most quickly.
Here’s how: Intuitive Eating Might Not Be What You Think
Bonus: Interoception: Improving Our Awareness Of Body Cues
About those cravings…
As illustrated a little above, a lot of cravings might not be what they first appear, and in evolutionary terms, our body is centuries behind industrialization, in terms of adaptations, which means that even if we try to take the above into account, our responses can sometimes be inappropriate in the age of supermarkets.
See also: The Science of Hunger, And How To Sate Cravings
Natural appetite suppressants
Eating more is not always the answer, not even if it’s more healthy food. And hunger pangs can be especially inconvenient if, for example, we are fasting at present, which is by the way a very healthful thing for most people:
Learn more: Intermittent Fasting: What’s the truth?
One way to suppress hunger is simply to trigger the stomach into sending “full” signals, which involves filling it. Since you do not want to overeat, the trick here is imply to use high-volume food.
Consider for example: 30 grapes and 30 raisins have approximately the same calorie count (what with raisins being dried grapes, and the calories didn’t evaporate), but the bowl of fresh fruit is going to physically fill your stomach a lot more quickly than the tiny amount of dried fruit.
More on this: Some Surprising Truths About Hunger And Satiety
Protein is of course also an appetite suppressant, but it takes about 20 minutes for the signal to kick in. So a “hack” here is to snack on something proteinous at least 15 minutes before your main meal (for example, a portion of nuts while cooking, unless you’re allergic, or some dried fish unless you’re vegetarian/vegan; you get it, pick something high in protein and good for snacking, and have a small portion before your main meal).
Nor is protein the only option!
See also: 3 Natural Appetite Suppressants Better Than Ozempic
Scale it down
Related to the above, there is a feedback loop that occurs here. The more you eat, the more your stomach slowly grows to accommodate it; the less you eat, the more your stomach slowly shrinks because the body tries hard to be an efficient organism, and will not maintain something that isn’t being used.
So, there’s a bit of a catch-22; sate your hunger by filling your stomach with high volume foods, but filling it will cause it to grow?
The trick is: do the “eat until 80% full” thing. That’s full enough that you have had a nice meal and are not suffering, without stretching the stomach.
Enjoy your food
Seriously! Actually enjoy it. Which means paying full attention to it. Eating can and should be a wonderful experience, so it’s best savored rather than inhaling a bowl of something in 30 seconds.
Have you seen those dog bowls that have obstructions to slow down how quickly a dog eats? We can leverage that kind of trick too! While you might not want to eat from a dog bowl, how about having a little bowl of pistachio nuts rather than ready-to-eat peanuts? Or any shelled nuts that we must shell as we go. If you’re allergic to nuts, there are plenty of other foods with a high work-to-food ratio. Take some time and enjoy that pomegranate, for instance!
Not that we necessarily have to make things difficult for ourselves either; we can just take appropriate care to ensure a good dining experience. Life is for living, so why not enjoy it?
See also: Mindful Eating: How To Get More Out Of What’s On Your Plate
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Parents are increasingly saying their child is ‘dysregulated’. What does that actually mean?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Welcome aboard the roller coaster of parenthood, where emotions run wild, tantrums reign supreme and love flows deep.
As children reach toddlerhood and beyond, parents adapt to manage their child’s big emotions and meltdowns. Parenting terminology has adapted too, with more parents describing their child as “dysregulated”.
But what does this actually mean?

ShUStudio/Shutterstock More than an emotion
Emotional dysregulation refers to challenges a child faces in recognising and expressing emotions, and managing emotional reactions in social settings.
This may involve either suppressing emotions or displaying exaggerated and intense emotional responses that get in the way of the child doing what they want or need to do.
“Dysregulation” is more than just feeling an emotion. An emotion is a signal, or cue, that can give us important insights to ourselves and our preferences, desires and goals.
An emotionally dysregulated brain is overwhelmed and overloaded (often, with distressing emotions like frustration, disappointment and fear) and is ready to fight, flight or freeze.
Developing emotional regulation
Emotion regulation is a skill that develops across childhood and is influenced by factors such as the child’s temperament and the emotional environment in which they are raised.
In the stage of emotional development where emotion regulation is a primary goal (around 3–5 years old), children begin exploring their surroundings and asserting their desires more actively.
A child’s temperament and upbringing affect how they regulate emotions. bluedog studio/Shutterstock It’s typical for them to experience emotional dysregulation when their initiatives are thwarted or criticised, leading to occasional tantrums or outbursts.
A typically developing child will see these types of outbursts reduce as their cognitive abilities become more sophisticated, usually around the age they start school.
Express, don’t suppress
Expressing emotions in childhood is crucial for social and emotional development. It involves the ability to convey feelings verbally and through facial expressions and body language.
When children struggle with emotional expression, it can manifest in various ways, such as difficulty in being understood, flat facial expressions even in emotionally charged situations, challenges in forming close relationships, and indecisiveness.
Several factors, including anxiety, attention-deficit hyperactivity disorder (ADHD), autism, giftedness, rigidity and both mild and significant trauma experiences, can contribute to these issues.
Common mistakes parents can make is dismissing emotions, or distracting children away from how they feel.
These strategies don’t work and increase feelings of overwhelm. In the long term, they fail to equip children with the skills to identify, express and communicate their emotions, making them vulnerable to future emotional difficulties.
We need to help children move compassionately towards their difficulties, rather than away from them. Parents need to do this for themselves too.
Caregiving and skill modelling
Parents are responsible for creating an emotional climate that facilitates the development of emotion regulation skills.
Parents’ own modelling of emotion regulation when they feel distressed. The way they respond to the expression of emotions in their children, contributes to how children understand and regulate their own emotions.
Children are hardwired to be attuned to their caregivers’ emotions, moods, and coping as this is integral to their survival. In fact, their biggest threat to a child is their caregiver not being OK.
Unsafe, unpredictable, or chaotic home environments rarely give children exposure to healthy emotion expression and regulation. Children who go through maltreatment have a harder time controlling their emotions, needing more brainpower for tasks that involve managing feelings. This struggle could lead to more problems with emotions later on, like feeling anxious and hypervigilant to potential threats.
Recognising and addressing these challenges early on is essential for supporting children’s emotional wellbeing and development.
A dysregulated brain and body
When kids enter “fight or flight” mode, they often struggle to cope or listen to reason. When children experience acute stress, they may respond instinctively without pausing to consider strategies or logic.
If your child is in fight mode, you might observe behaviours such as crying , clenching fists or jaw, kicking, punching, biting, swearing, spitting or screaming.
In flight mode, they may appear restless, have darting eyes, exhibit excessive fidgeting, breathe rapidly, or try to run away.
A shut-down response may look like fainting or a panic attack.
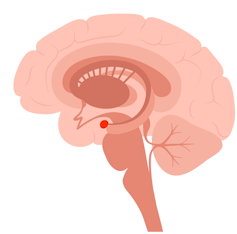
When a child feels threatened, their brain’s frontal lobe, responsible for rational thinking and problem-solving, essentially goes offline.
The amygdala, shown here in red, triggers survival mode. pikovit/Shutterstock This happens when the amygdala, the brain’s alarm system, sends out a false alarm, triggering the survival instinct.
In this state, a child may not be able to access higher functions like reasoning or decision-making.
While our instinct might be to immediately fix the problem, staying present with our child during these moments is more effective. It’s about providing support and understanding until they feel safe enough to engage their higher brain functions again.
Reframe your thinking so you see your child as having a problem – not being the problem.
Tips for parents
Take turns discussing the highs and lows of the day at meal times. This is a chance for you to be curious, acknowledge and label feelings, and model that you, too, experience a range of emotions that require you to put into practice skills to cope and has shown evidence in numerous physical, social-emotional, academic and behavioural benefits.
Talk about your day over dinner. Monkey Business Images/Shutterstock Spending even small amounts (five minutes a day!) of quality one-on-one time with your child is an investment in your child’s emotional wellbeing. Let them pick the activity, do your best to follow their lead, and try to notice and comment on the things they do well, like creative ideas, persevering when things are difficult, and being gentle or kind.
Take a tip from parents of children with neurodiversity: learn about your unique child. Approaching your child’s emotions, temperament, and behaviours with curiosity can help you to help them develop emotion regulation skills.
When to get help
If emotion dysregulation is a persistent issue that is getting in the way of your child feeling happy, calm, or confident – or interfering with learning or important relationships with family members or peers – talk to their GP about engaging with a mental health professional.
Many families have found parenting programs helpful in creating a climate where emotions can be safely expressed and shared.
Remember, you can’t pour from an empty cup. Parenting requires you to be your best self and tend to your needs first to see your child flourish.
Cher McGillivray, Assistant Professor Psychology Department, Bond University and Shawna Mastro Campbell, Assistant Professor Psychology, Bond University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

The Circadian Diabetes Code – by Dr. Satchin Panda
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We have previously reviewed Dr. Panda’s “The Circadian Code” which pertains to the circadian rhythms (yes, plural) in general; this one uses much of the same research, but with a strong focus on the implications for blood sugar management.
It’s first a primer in diabetes (and prediabetes, and, in contrast, what things should look like if healthy). You’ll understand about glucose metabolism and glycogen and insulin and more; you’ll understand what blood sugar readings mean, and you’ll know what an Hb1AC count actually is and what it should look like too, things like that.
After that, it’s indeed about what the subtitle promises: the right times to eat (and what to eat), when to exercise (and how, at which time), and how to optimize your sleep in the context of circadian rhythm and blood sugar management.
You may be wondering: why does circadian rhythm matter for blood sugars? And the answer is explained at some length in the first part of the book, but to oversimplify greatly: your body needs energy all the time, no matter when it was that you last ate. Thus, it has to organize its energy reserves to that at all times you can 1) function, on a cellular level 2) maintain a steady balance of sugar in your blood despite using it at slightly higher or lower levels at different times of day. Because the basal metabolic rate accounts for most of our energy use, the body has to plan for a base rate of so much energy per day, and to do that, it needs to know what a day is. Dr. Panda explains this in detail (the marvels of PER proteins and all that), but basically, that’s the relevance of circadian rhythm.
However, it’s not all theory and biochemistry; there is also a 12-week program to reverse prediabetes and type 2 diabetes (it will not, of course, reverse Type 1 Diabetes, sorry—but the program will still be beneficial even in that case, since more even blood sugars means fewer woes).
They style is friendly and clear, explaining the science simply, yet without patronizing the reader. References are given, with claims sourced in an extensive bibliography.
Bottom line: if you or a loved one have diabetes or prediabetes, or just have a strong desire to avoid getting such and generally keep your metabolic health in good order, this book will definitely help.
Click here to check out The Diabetes Code, and enjoy better blood sugar health than ever!
Share This Post
-

Vodka vs Beer – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing vodka to beer, we picked the vodka.
Why?
As you might have guessed, neither are exactly healthy. But one of them is relatively, and we stress relatively, less bad than the other.
In the category of nutrients, vodka is devoid of nutrients, and beer has small amounts of some vitamins and minerals—but the amounts are so small, that you would need to drink yourself to death before benefiting from them meaningfully. And while beer gets touted as “liquid bread”, it really isn’t. A thousand years ago it will have been a lot less alcoholic and more carby, but even then, it wasn’t a health product aside from that it provided a way of making potentially contaminated water safer to drink.
In the category of carbohydrates, vodka nominally has none, due to the distillation process, and beer has some. Glycemic index websites often advise that the GI of beers, wines, and spirits can’t be measured as their carb content is not sufficient to get a meaningful sample, but diabetes research tells a more useful story:
Any alcoholic drink will generally cause a brief drop in blood sugars, followed by a spike. This happens because the liver prioritises metabolizing alcohol over producing glycogen, so it hits pause on the sugar metabolism and then has a backlog to catch up on. In the case of alcoholic drinks that have alcohol and carbs, this will be more pronounced—so this means that the functional glycemic load of beer is higher.
That’s a point in favor of vodka.
Additionally, in terms of the alcohol content, correctly-distilled vodka’s alcohol is pure ethanol, while beer will contain an amount of methanol that will vary per beer, but an illustrative nominal figure could be about 16mg/L. Methanol is more harmful than ethanol.
So that’s another point in favor of vodka.
Once again, neither drink is healthy; both are distinctly unhealthy. But unit for unit, beer is the least healthy of the two, making vodka the lesser of two evils.
Want to learn more?
You might like to read:
- Can We Drink To Good Health? (answer: we cannot, but this was about alcohol’s proposed heart-healthy benefits)
- Guinness Is Good For You* (it isn’t, but this was the long-time slogan and marketing campaign that fooled many)
- How To Reduce Or Quit Alcohol
- How To Unfatty A Fatty Liver
Take care!
Share This Post




-

Sesame Oil vs Almond Oil – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing sesame oil to almond oil, we picked the almond.
Why?
We were curious about this one! Were you, or were you confident? You see, almonds tend to blow away all the other nuts with their nutritional density, but they’re far from the oiliest of nuts, and their greatest strengths include their big dose of protein and fiber (which don’t make it into the oil), vitamins (most of which don’t make it into the oil) and minerals (which don’t make it into the oil). So, a lot will come down to the fat profile!
On which note, looking at the macros first, it’s 100% fat in both cases, but sesame oil has more saturated fat and polyunsaturated fat, while almond oil has more monounsaturated fat. Since the mono- and poly-unsaturated fats are both healthy and each oil has more of one or the other, the deciding factor here is which has the least saturated fat—and that’s the almond oil, which has close to half the saturated fat of sesame oil. As an aside, neither of them are a source of omega-3 fatty acids.
In terms of vitamins, there’s not a lot to say here, but “not a lot” is not nothing: sesame oil has nearly 2x the vitamin K, while almond oil has 28x the vitamin E*, and 2x the choline. So, another win for almond oil.
*which is worth noting, not least of all because seeds are more widely associated with vitamin E in popular culture, but it’s the almond oil that provide much more here. Not to get too distracted into looking at the values of the actual seeds and nuts, almonds themselves do have over 102x the vitamin E compared to sesame seeds.
Now, back to the oils:
In the category of minerals, there actually is nothing to say here, except you can’t get more than the barest trace of any mineral from either of these two oils. So it’s a tie on this one.
Adding up the categories makes for a clear win for almond oil!
Want to learn more?
You might like to read:
Avocado Oil vs Olive Oil – Which is Healthier?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Hazelnuts vs Almonds – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing hazelnuts to almonds, we picked the almonds.
Why?
It’s closer than you might think! But we say almonds do come out on top.
In terms of macronutrients, almonds have notably more protein, while hazelnuts have notably more fat (healthy fats, though). Almonds are also higher in both carbs and fiber. Looking at Glycemic Index, hazelnuts’ GI is low and almonds’ GI is zero. We could call the macros category a tie, but ultimately if we need to prioritize any of these things, it’s protein and fiber, so we’ll call this a nominal win for almonds.
When it comes to vitamins, hazelnuts have more of vitamins B1, B5, B6, B9 C, and K. Meanwhile, almonds have more of vitamins B2, B3, E, and choline. So, a moderate win for hazelnuts.
In the category of minerals, almonds retake the lead with more calcium, magnesium, phosphorus, potassium, selenium, and zinc, while hazelnuts boast more copper and manganese. A clear win for almonds.
Adding up the categories, this makes for a marginal win for almonds. Of course, both of these nuts are very healthy (assuming you are not allergic), and best is to enjoy both if possible.
Want to learn more?
You might like to read:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

We created a VR tool to test brain function. It could one day help diagnose dementia
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
If you or a loved one have noticed changes in your memory or thinking as you’ve grown older, this could reflect typical changes that occur with ageing. In some cases though, it might suggest something more, such as the onset of dementia.
The best thing to do if you have concerns is to make an appointment with your GP, who will probably run some tests. Assessment is important because if there is something more going on, early diagnosis can enable prompt access to the right interventions, supports and care.
But current methods of dementia screening have limitations, and testing can be daunting for patients.
Our research suggests virtual reality (VR) could be a useful cognitive screening tool, and mitigate some of the challenges associated with current testing methods, opening up the possibility it may one day play a role in dementia diagnosis.
Where current testing is falling short
If someone is worried about their memory and thinking, their GP might ask them to complete a series of quick tasks that check things like the ability to follow simple instructions, basic arithmetic, memory and orientation.
These sorts of screening tools are really good at confirming cognitive problems that may already be very apparent. But commonly used screening tests are not always so good at detecting early and more subtle difficulties with memory and thinking, meaning such changes could be missed until they get worse.
A clinical neuropsychological assessment is better equipped to detect early changes. This involves a comprehensive review of a patient’s personal and medical history, and detailed assessment of cognitive functions, including attention, language, memory, executive functioning, mood factors and more. However, this can be costly and the testing can take several hours.
Testing is also somewhat removed from everyday experience, not directly tapping into activities of daily living.
Enter virtual reality
VR technology uses computer-generated environments to create immersive experiences that feel like real life. While VR is often used for entertainment, it has increasingly found applications in health care, including in rehabilitation and falls prevention.
Using VR for cognitive screening is still a new area. VR-based cognitive tests generally create a scenario such as shopping at a supermarket or driving around a city to ascertain how a person would perform in these situations.
Notably, they engage various senses and cognitive processes such as sight, sound and spatial awareness in immersive ways. All this may reveal subtle impairments which can be missed by standard methods.
VR assessments are also often more engaging and enjoyable, potentially reducing anxiety for those who may feel uneasy in traditional testing environments, and improving compliance compared to standard assessments.
Millions of people around the world have dementia.
pikselstock/ShutterstockMost studies of VR-based cognitive tests have explored their capacity to pick up impairments in spatial memory (the ability to remember where something is located and how to get there), and the results have been promising.
Given VR’s potential for assisting with diagnosis of cognitive impairment and dementia remains largely untapped, our team developed an online computerised game (referred to as semi-immersive VR) to see how well a person can remember, recall and complete everyday tasks. In our VR game, which lasts about 20 minutes, the user role plays a waiter in a cafe and receives a score on their performance.
To assess its potential, we enlisted more than 140 people to play the game and provide feedback. The results of this research are published across three recent papers.
Testing our VR tool
In our most recently published study, we wanted to verify the accuracy and sensitivity of our VR game to assess cognitive abilities.
We compared our test to an existing screening tool (called the TICS-M) in more than 130 adults. We found our VR task was able to capture meaningful aspects of cognitive function, including recalling food items and spatial memory.
We also found younger adults performed better in the game than older adults, which echoes the pattern commonly seen in regular memory tests.
Adults of a range of ages tried our computerised game.
pikselstock/ShutterstockIn a separate study, we followed ten adults aged over 65 while they completed the game, and interviewed them afterwards. We wanted to understand how this group – who the tool would target – perceived the task.
These seniors told us they found the game user-friendly and believed it was a promising tool for screening memory. They described the game as engaging and immersive, expressing enthusiasm to continue playing. They didn’t find the task created anxiety.
For a third study, we spoke to seven health-care professionals about the tool. Overall they gave positive feedback, and noted its dynamic approach to age-old diagnostic challenges.
However, they did flag some concerns and potential barriers to implementing this sort of tool. These included resource constraints in clinical practice (such as time and space to carry out the assessment) and whether it would be accessible for people with limited technological skills. There was also some scepticism about whether the tool would be an accurate method to assist with dementia diagnosis.
While our initial research suggests this tool could be a promising way to assess cognitive performance, this is not the same as diagnosing dementia. To improve the test’s ability to accurately detect those who likely have dementia, we’ll need to make it more specific for that purpose, and carry out further research to validate its effectiveness.
We’ll be conducting more testing of the game soon. Anyone interested in giving it a go to help with our research can register on our team’s website.

Joyce Siette, Research Theme Fellow in Health and Wellbeing, Western Sydney University and Paul Strutt, Senior Lecturer in Psychology, Western Sydney University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: