How To Reduce The Harm Of Festive Drinking (Without Abstaining)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How To Reduce The Harm Of Festive Drinking
Not drinking alcohol is—of course—the best way to avoid the harmful effects of alcohol. However, not everyone wants to abstain, especially at this time of year, so today we’re going to be focusing on harm reduction without abstinence.
If you do want to quit (or even reduce) drinking, you might like our previous article about that:
For everyone else, let’s press on with harm reduction:
Before You Drink
A common (reasonable, but often unhelpful) advice is “set yourself a limit”. The problem with this is that when we’re sober, “I will drink no more than n drinks” is easy. After the first drink, we start to feel differently about it.
So: delay your first drink of the day for as long as possible
That’s it, that’s the tip. The later you start drinking, not only will you likely drink less, but also, your liver will have had longer to finish processing whatever you drank last night, so it’s coming at the new drink(s) fresh.
On that note…
Watch your meds! Often, especially if we are taking medications that also tax our liver (acetaminophen / paracetamol / Tylenol is a fine example of this), we are at risk of having a bit of a build-up, like an office printer that still chewing on the last job while you’re trying to print the next.
Additionally: do indeed eat before you drink.
While You Drink
Do your best to drink slowly. While this can hit the same kind of problem as the “set yourself a limit” idea, in that once you start drinking you forget to drink slowly, it’s something to try for.
If your main reason for drinking is the social aspect, then merely having a drink in your hand is generally sufficient. You don’t need to be keeping pace with anyone.
It is further good to alternate your drinks with water. As in, between each alcoholic drink, have a glass of water. This helps in several ways:
- Hydrates you, which is good for your body’s recovery abilities
- Halves the amount of time you spend drinking
- Makes you less thirsty; it’s easy to think “I’m thirsty” and reach for an alcoholic drink that won’t actually help. So, it may slow down your drinking for that reason, too.
At the dinner table especially, it’s very reasonable to have two glasses, one filled with water. Nobody will be paying attention to which glass you drink from more often.
After You Drink
Even if you are not drunk, assume that you are.
Anything you wouldn’t let a drunk person in your care do, don’t do. Now is not the time to drive, have a shower, or do anything you wouldn’t let a child do in the kitchen.
Hospital Emergency Rooms, every year around this time, get filled up with people who thought they were fine and then had some accident.
The biggest risks from alcohol are:
- Accidents
- Heart attacks
- Things actually popularly associated with alcohol, e.g. alcohol poisoning etc
So, avoiding accidents is as important as, if not more important than, avoiding damage to your liver.
Drink some water, and eat something.
Fruit is great, as it restocks you on vitamins, minerals, and water, while being very easy to digest.
Go to bed.
There is a limit to how much trouble you can get into there. Sleep it off.
In the morning, do not do “hair of the dog”; drinking alcohol will temporarily alleviate a hangover, but only because it kicks your liver back into an earlier stage of processing the alcohol—it just prolongs the inevitable.
Have a good breakfast, instead. Remember, fruit is your friend (as explained above).
Want to know more?
Here’s a great service with a lot of further links to a lot more resources:
With You | How to safely detox from alcohol at home
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Is A Visible Six-Pack Obtainable Regardless Of Genetic Predisposition?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small 😎
❝Is it possible for anyone to get 6-pack abs (even if genetics makes it easier or harder) and how much does it matter for health e.g. waist size etc?❞
Let’s break it down into two parts:
Is it possible for anyone to get 6-pack abs (even if genetics makes it easier or harder)?
Short answer: no
First, a quick anatomy lesson: while “abs” (abdominal muscles) are considered in the plural and indeed they are, what we see as a six-pack is actually only one muscle, the rectus abdominis, which is nestled in between other abdominal muscles that are beyond the scope of our answer here.
The reason that the rectus abdominis looks like six muscles is because there are bands of fascia (connective tissue) lying over it, so we see where it bulges between those bands.
The main difference genes make are as follows:
- Number of fascia bands (and thus the reason that some people get a four-, six-, eight-, or rarely, even ten-pack). Obviously, no amount of training can change this number, any more than doing extra bicep curls will grow you additional arms.
- Density of muscle fibers. Some people have what has been called “superathlete muscle type”, which, while prized by Olympians and other athletes, is on bodybuilding forums less glamorously called being a “hard gainer”. What this means is that muscle fibers are denser, so while training will make muscles stronger, you won’t see as much difference in size. This means that size for size, the person with this muscle type will always be stronger than someone the same size without it, but that may be annoying if you’re trying to build visible definition.
- Twitch type of muscle fibers. Some people have more fast-twitch fibers, some have more slow-twitch fibers. Fast-twitch fibers are better suited for visible abs (and, as the name suggests, quick changes between contracting and relaxing). Slow-twitch fibers are better for endurance, but yield less bulky muscles.
- Inclination to subcutaneous fat storage. This is by no means purely genetic; hormones make the biggest difference, followed by diet. But, genes are an influencing factor, and if your body fat percentage is inclined to be higher than someone else’s, then it’ll take more work to see muscle definition under that fat.
The first of those items is why our simple answer is “no”; because some people are destined to, if muscle is visible, have a four-, eight, or (rarely) ten-pack, making a six-pack unobtainable.
It’s worth noting here that while a bigger number is more highly prized aesthetically, there is literally zero difference healthwise or in terms of performance, because it’s nothing to do with the muscle, and is only about the fascia layout.
The density of muscle fibers is again purely genetic, but it only makes things easier or harder; this part’s not impossible for anyone.
The inclination to subcutaneous fat storage is by far the most modifiable factor, and the thus most readily overcome, if you feel so inclined. That doesn’t mean it will necessarily be easy! But it does mean that it’s relatively less difficult than the others.
How much does it matter for health, e.g. waist size etc?
As you may have gathered from the above, having a six-pack (or indeed a differently-numbered “pack”, if that be your genetic lot) makes no important difference to health:
- The fascia layout is completely irrelevant to health
- The muscle fiber types do make a difference to athletic performance, but not general health when at rest
- The subcutaneous fat storage is a health factor, but probably not how most people think
Healthy body fat percentages are (assuming normal hormones) in the range of 20–25% for women and 15–20% for men.
For most people, having clearly visible abs requires going below those healthy levels. For most people, that’s not optimally healthy. And those you see on magazine covers or in bodybuilding competitions are usually acutely dehydrated for the photo, which is of course not good. They will rehydrate after the shoot.
However, waist size (especially as a ratio, compared to hip size) is very important to health. This has less to do with subcutaneous fat, though, and is more to do with visceral belly fat, which goes under the muscles and thus does not obscure them:
Visceral Belly Fat & How To Lose It
One final note: fat notwithstanding, and aesthetics notwithstanding, having a strong core is very good for general health; it helps keeps one’s internal organs in place and well-protected, and improves stability, making falls less likely as we get older. Additionally, having muscle improves our metabolic base rate, which is good for our heart. Abs are just one part of core strength (the back being important too, for example), but should not be neglected.
Top-tier exercises to do include planks, and hanging leg raises (i.e. hang from some support, such as a chin-up bar, and raise your legs, which counterintuitively works your abs a lot more than your legs).
Take care!
Share This Post
-

A person in Texas caught bird flu after mixing with dairy cattle. Should we be worried?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The United States’ Centers for Disease Control and Prevention (CDC) has issued a health alert after the first case of H5N1 avian influenza, or bird flu, seemingly spread from a cow to a human.
A farm worker in Texas contracted the virus amid an outbreak in dairy cattle. This is the second human case in the US; a poultry worker tested positive in Colorado in 2022.
The virus strain identified in the Texan farm worker is not readily transmissible between humans and therefore not a pandemic threat. But it’s a significant development nonetheless.
Some background on bird flu
There are two types of avian influenza: highly pathogenic or low pathogenic, based on the level of disease the strain causes in birds. H5N1 is a highly pathogenic avian influenza.
H5N1 first emerged in 1997 in Hong Kong and then China in 2003, spreading through wild bird migration and poultry trading. It has caused periodic epidemics in poultry farms, with occasional human cases.
Influenza A viruses such as H5N1 are further divided into variants, called clades. The unique variant causing the current epidemic is H5N1 clade 2.3.4.4b, which emerged in late 2020 and is now widespread globally, especially in the Americas.
In the past, outbreaks could be controlled by culling of infected birds, and H5N1 would die down for a while. But this has become increasingly difficult due to escalating outbreaks since 2021.
Wild animals are now in the mix
Waterfowl (ducks, swans and geese) are the main global spreaders of avian flu, as they migrate across the world via specific routes that bypass Australia. The main hub for waterfowl to migrate around the world is Quinghai lake in China.
But there’s been an increasing number of infected non-waterfowl birds, such as true thrushes and raptors, which use different flyways. Worryingly, the infection has spread to Antarctica too, which means Australia is now at risk from different bird species which fly here.
H5N1 has escalated in an unprecedented fashion since 2021, and an increasing number of mammals including sea lions, goats, red foxes, coyotes, even domestic dogs and cats have become infected around the world.
Wild animals like red foxes which live in peri-urban areas are a possible new route of spread to farms, domestic pets and humans.
Dairy cows and goats have now become infected with H5N1 in at least 17 farms across seven US states.
What are the symptoms?
Globally, there have been 14 cases of H5N1 clade 2.3.4.4b virus in humans, and 889 H5N1 human cases overall since 2003.
Previous human cases have presented with a severe respiratory illness, but H5N1 2.3.4.4b is causing illness affecting other organs too, like the brain, eyes and liver.
For example, more recent cases have developed neurological complications including seizures, organ failure and stroke. It’s been estimated that around half of people infected with H5N1 will die.
The case in the Texan farm worker appears to be mild. This person presented with conjunctivitis, which is unusual.
Food safety
Contact with sick poultry is a key risk factor for human infection. Likewise, the farm worker in Texas was likely in close contact with the infected cattle.
The CDC advises pasteurised milk and well cooked eggs are safe. However, handling of infected meat or eggs in the process of cooking, or drinking unpasteurised milk, may pose a risk.
Although there’s no H5N1 in Australian poultry or cattle, hygienic food practices are always a good idea, as raw milk or poorly cooked meat, eggs or poultry can be contaminated with microbes such as salmonella and E Coli.
If it’s not a pandemic, why are we worried?
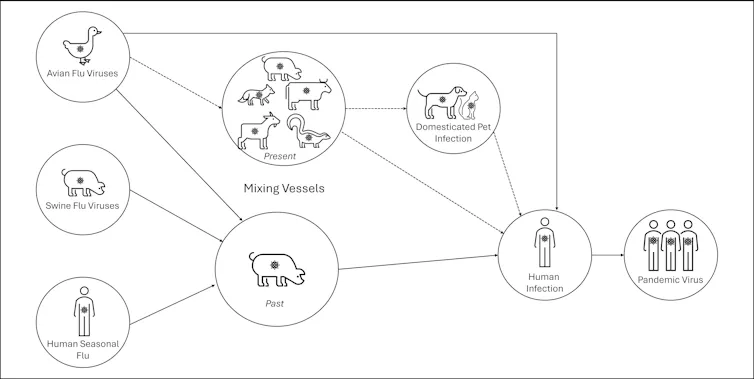
Scientists have feared avian influenza may cause a pandemic since about 2005. Avian flu viruses don’t easily spread in humans. But if an avian virus mutates to spread in humans, it can cause a pandemic.
One concern is if birds were to infect an animal like a pig, this acts as a genetic mixing vessel. In areas where humans and livestock exist in close proximity, for example farms, markets or even in homes with backyard poultry, the probability of bird and human flu strains mixing and mutating to cause a new pandemic strain is higher.

There are a number of potential pathways to a pandemic caused by influenza. Author provided The cows infected in Texas were tested because farmers noticed they were producing less milk. If beef cattle are similarly affected, it may not be as easily identified, and the economic loss to farmers may be a disincentive to test or report infections.
How can we prevent a pandemic?
For now there is no spread of H5N1 between humans, so there’s no immediate risk of a pandemic.
However, we now have unprecedented and persistent infection with H5N1 clade 2.3.4.4b in farms, wild animals and a wider range of wild birds than ever before, creating more chances for H5N1 to mutate and cause a pandemic.
Unlike the previous epidemiology of avian flu, where hot spots were in Asia, the new hot spots (and likely sites of emergence of a pandemic) are in the Americas, Europe or in Africa.
Pandemics grow exponentially, so early warnings for animal and human outbreaks are crucial. We can monitor infections using surveillance tools such as our EPIWATCH platform.
The earlier epidemics can be detected, the better the chance of stamping them out and rapidly developing vaccines.
Although there is a vaccine for birds, it has been largely avoided until recently because it’s only partially effective and can mask outbreaks. But it’s no longer feasible to control an outbreak by culling infected birds, so some countries like France began vaccinating poultry in 2023.
For humans, seasonal flu vaccines may provide a small amount of cross-protection, but for the best protection, vaccines need to be matched exactly to the pandemic strain, and this takes time. The 2009 flu pandemic started in May in Australia, but the vaccines were available in September, after the pandemic peak.
To reduce the risk of a pandemic, we must identify how H5N1 is spreading to so many mammalian species, what new wild bird pathways pose a risk, and monitor for early signs of outbreaks and illness in animals, birds and humans. Economic compensation for farmers is also crucial to ensure we detect all outbreaks and avoid compromising the food supply.
C Raina MacIntyre, Professor of Global Biosecurity, NHMRC L3 Research Fellow, Head, Biosecurity Program, Kirby Institute, UNSW Sydney; Ashley Quigley, Senior Research Associate, Global Biosecurity, UNSW Sydney; Haley Stone, PhD Candidate, Biosecurity Program, Kirby Institute, UNSW Sydney; Matthew Scotch, Associate Dean of Research and Professor of Biomedical Informatics, College of Health Solutions, Arizona State University, and Rebecca Dawson, Research Associate, The Kirby Institute, UNSW Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Mental illness, psychiatric disorder or psychological problem. What should we call mental distress?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We talk about mental health more than ever, but the language we should use remains a vexed issue.
Should we call people who seek help patients, clients or consumers? Should we use “person-first” expressions such as person with autism or “identity-first” expressions like autistic person? Should we apply or avoid diagnostic labels?
These questions often stir up strong feelings. Some people feel that patient implies being passive and subordinate. Others think consumer is too transactional, as if seeking help is like buying a new refrigerator.
Advocates of person-first language argue people shouldn’t be defined by their conditions. Proponents of identity-first language counter that these conditions can be sources of meaning and belonging.
Avid users of diagnostic terms see them as useful descriptors. Critics worry that diagnostic labels can box people in and misrepresent their problems as pathologies.
Underlying many of these disagreements are concerns about stigma and the medicalisation of suffering. Ideally the language we use should not cast people who experience distress as defective or shameful, or frame everyday problems of living in psychiatric terms.
Our new research, published in the journal PLOS Mental Health, examines how the language of distress has evolved over nearly 80 years. Here’s what we found.
Engin Akyurt/Pexels Generic terms for the class of conditions
Generic terms – such as mental illness, psychiatric disorder or psychological problem – have largely escaped attention in debates about the language of mental ill health. These terms refer to mental health conditions as a class.
Many terms are currently in circulation, each an adjective followed by a noun. Popular adjectives include mental, mental health, psychiatric and psychological, and common nouns include condition, disease, disorder, disturbance, illness, and problem. Readers can encounter every combination.
These terms and their components differ in their connotations. Disease and illness sound the most medical, whereas condition, disturbance and problem need not relate to health. Mental implies a direct contrast with physical, whereas psychiatric implicates a medical specialty.
Mental health problem, a recently emerging term, is arguably the least pathologising. It implies that something is to be solved rather than treated, makes no direct reference to medicine, and carries the positive connotations of health rather than the negative connotation of illness or disease.
Is ‘mental health problem’ actually less pathologising? Monkey Business Images/Shutterstock Arguably, this development points to what cognitive scientist Steven Pinker calls the “euphemism treadmill”, the tendency for language to evolve new terms to escape (at least temporarily) the offensive connotations of those they replace.
English linguist Hazel Price argues that mental health has increasingly come to replace mental illness to avoid the stigma associated with that term.
How has usage changed over time?
In the PLOS Mental Health paper, we examine historical changes in the popularity of 24 generic terms: every combination of the nouns and adjectives listed above.
We explore the frequency with which each term appears from 1940 to 2019 in two massive text data sets representing books in English and diverse American English sources, respectively. The findings are very similar in both data sets.
The figure presents the relative popularity of the top ten terms in the larger data set (Google Books). The 14 least popular terms are combined into the remainder.
Relative popularity of alternative generic terms in the Google Books corpus. Haslam et al., 2024, PLOS Mental Health. Several trends appear. Mental has consistently been the most popular adjective component of the generic terms. Mental health has become more popular in recent years but is still rarely used.
Among nouns, disease has become less widely used while illness has become dominant. Although disorder is the official term in psychiatric classifications, it has not been broadly adopted in public discourse.
Since 1940, mental illness has clearly become the preferred generic term. Although an assortment of alternatives have emerged, it has steadily risen in popularity.
Does it matter?
Our study documents striking shifts in the popularity of generic terms, but do these changes matter? The answer may be: not much.
One study found people think mental disorder, mental illness and mental health problem refer to essentially identical phenomena.
Other studies indicate that labelling a person as having a mental disease, mental disorder, mental health problem, mental illness or psychological disorder makes no difference to people’s attitudes toward them.
We don’t yet know if there are other implications of using different generic terms, but the evidence to date suggests they are minimal.
The labels we use may not have a big impact on levels of stigma. Pixabay/Pexels Is ‘distress’ any better?
Recently, some writers have promoted distress as an alternative to traditional generic terms. It lacks medical connotations and emphasises the person’s subjective experience rather than whether they fit an official diagnosis.
Distress appears 65 times in the 2022 Victorian Mental Health and Wellbeing Act, usually in the expression “mental illness or psychological distress”. By implication, distress is a broad concept akin to but not synonymous with mental ill health.
But is distress destigmatising, as it was intended to be? Apparently not. According to one study, it was more stigmatising than its alternatives. The term may turn us away from other people’s suffering by amplifying it.
So what should we call it?
Mental illness is easily the most popular generic term and its popularity has been rising. Research indicates different terms have little or no effect on stigma and some terms intended to destigmatise may backfire.
We suggest that mental illness should be embraced and the proliferation of alternative terms such as mental health problem, which breed confusion, should end.
Critics might argue mental illness imposes a medical frame. Philosopher Zsuzsanna Chappell disagrees. Illness, she argues, refers to subjective first-person experience, not to an objective, third-person pathology, like disease.
Properly understood, the concept of illness centres the individual and their connections. “When I identify my suffering as illness-like,” Chappell writes, “I wish to lay claim to a caring interpersonal relationship.”
As generic terms go, mental illness is a healthy option.
Nick Haslam, Professor of Psychology, The University of Melbourne and Naomi Baes, Researcher – Social Psychology/ Natural Language Processing, The University of Melbourne
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post





Related Posts
-
Get Better Sleep: Beyond The Basics
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First though, for the sake of being methodical, let’s quickly note the basics:
- Aim for 7–9 hours per night
- Set a regular bedtime and (equally important!) regular getting-up time
- Have a 2-hour wind-down period before bed, to decompress from any stresses of the day
- Minimal device/screen usage before bed
- Abstain from stimulants for as long before bed as reasonably possible (caffeine elimination halflife is 4–8 hours depending on your genes, call it 6 hours average to eliminate half (not the whole lot), and you’ll see it’s probably best to put a cap on it earlier rather than later).
- Abstain from alcohol, ideally entirely, but allow at least 1hr/unit before bed. So for example, 1hr for a 1oz single shot of spirits, or 2–3 hours for a glass of wine (depending on size), or 3–4 hours for a martini (depending on recipe). Not that that is not the elimination time, nor even the elimination halflife of alcohol, it’s just a “give your body a chance at least” calculation. If you like to have a drink to relax before bed, then well, only you can decide what you like more: that or actually getting restorative sleep.
- Consider a warm bath/shower before bed, if that suits your schedule.
- Wash and change your bedsheets more often than seems necessary. Or if that’s too onerous, at least change the pillowcases more often, which makes quite a difference already.
- Lower the temperature of your bedroom shortly before bedtime; this will help cue the body to produce melatonin
- Make your bedroom as dark as reasonably possible. Invest in blackout blinds/curtains, and remove any pesky electronics, or at least cover their little LEDs if it’s something that reasonably needs to remain on.
Ok, now, onwards…
Those 7–9 hours? Yes, it goes for you too.
A lot of people mistake getting 6 hours sleep per night for only needing 6 hours sleep per night. Sure, you may still be alive after regularly getting 6 hours, but (unless you have a rare mutation of the ADRB1 gene) it will be causing harm, and yes, that includes later in life; we don’t stop needing so much sleep, even stop getting it:
Why You Probably Need More Sleep
With this in mind, it becomes important to…
Prioritize your sleep—which means planning for it!
When does your bedtime routine start? According to sleep scientist Dr. Lisa Matricciani, it starts before breakfast. This is because the things we do earlier in the day can greatly affect the amount (and quality) of sleep we get later. For example, a morning moderate-to-intense exercise session greatly improves sleep at night:
Planning Ahead For Better Sleep
As for quality, that is as important as quantity, and it’s not just about “soundness” of sleep:
The 6 Dimensions Of Sleep (And Why They Matter)
“What gets measured, gets done” goes for sleep too
Sleep-deprived people usually underestimate how sleep-deprived they are. This is for the same reason as why drunk people usually underestimate how drunk they are—to put it in words that go for both situations: a cognitively impaired person lacks the cognitive function to realize how cognitively impaired they are.
Here’s the science on that, by the way:
How Sleep-Deprived Are You, Really?
For that reason, we recommend using sleep-tracking software (there are many apps for that) on your phone or, ideally, a wearable device (such as a smartwatch or similar).
A benefit of doing so is that we don’t think “well, I slept from 10pm to 6am, so that’s 8 hours”, if our device tells us we slept between 10:43pm and 5:56 am with 74% sleep efficiency because we woke up many times.
As an aside, sleep efficiency should be about 85%, by the way. Why not 100%, you ask? It’s because if your body is truly out like a light for the entire night, something is wrong (either you were very sleep-deprived, or you have been drugged, that kind of thing). See also:
An unbroken night’s sleep is a myth. Here’s what good sleep looks like.
So waking up during the night is normal, and nothing to worry about per se. If you do find trouble getting back to sleep, though:
How to Fall Back Asleep After Waking Up in the Middle of the Night
Be careful about how you try to supplement sleep
This goes both for taking substances of various kinds, and napping. Some sleep aids can help, but many are harmful and/or do not really work as such; here’s a rundown of examples of those:
Safe Effective Sleep Aids For Seniors?
And when it comes to napping, timing is everything:
How To Nap Like A Pro (No More “Sleep Hangovers”!)
Want to know a lot more?
This is the book on sleep:
Why We Sleep – by Dr. Matthew Walker
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Problem With Sweeteners
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The WHO’s view on sugar-free sweeteners
The WHO has released a report offering guidance regards the use of sugar-free sweeteners as part of a weight-loss effort.
In a nutshell, the guidance is: don’t
- Here’s the report itself: Use of non-sugar sweeteners: WHO guideline
- Here’s the WHO’s own press release about it: WHO advises not to use non-sugar sweeteners for weight control in newly released guideline
- And it was based on this huge systematic review: Health effects of the use of non-sugar sweeteners: a systematic review and meta-analysis
They make for interesting reading, so if you don’t have time now, you might want to just quickly open and bookmark them for later!
Some salient bits and pieces:
Besides that some sweeteners can cause gastro-intestinal problems, a big problem is desensitization:
Because many sugar substitutes are many times (in some cases, hundreds of times) sweeter than sugar, this leads to other sweet foods tasting more bland, causing people to crave sweeter and sweeter foods for the same satisfaction level.
You can imagine how that’s not a spiral that’s good for the health!
The WHO recommendation applies to artificial and naturally-occurring non-sugar sweeteners, including:
- Acesulfame K
- Advantame
- Aspartame
- Cyclamates
- Neotame
- Saccharin
- Stevia
Sucralose and erythritol, by the way, technically are sugars, just not “that kind of sugar” so they didn’t make the list of non-sugar sweeteners.
That said, a recent study did find that erythritol was linked to a higher risk of heart attack, stroke, and early death, so it may not be an amazing sweetener either:
Read: The artificial sweetener erythritol and cardiovascular event risk
Want to know a good way of staying healthy in the context of sweeteners?
Just get used to using less. Your taste buds will adapt, and you’ll get just as much pleasure as before, from progressively less sweetening agent.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Cantaloupe vs Lychees – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing cantaloupe to lychees, we picked the cantaloupe.
Why?
Both have their merits and it was close!
In terms of macros, there’s no meaningful difference except that lychees have more carbs, so that could swing this any which way depending on how you feel about that. There’s enough fiber in both that it’s a non-issue metabolically though, so we call this round a tie.
In the category of vitamins, cantaloupe has more of vitamins A, B1, B3, B5, B7, B9, and K, while lychees have more of vitamins B2, B6, C, and E; a 7:4 win for cantaloupe.
Looking at minerals, cantaloupe has more calcium, magnesium, potassium, and zinc, while lychees have more copper, iron, phosphorus, and selenium, for a 4:4 tie in this round.
Adding up the sections makes for a modest overall win for cantaloupe, but by all means enjoy either or both, as diversity is good!
Want to learn more?
You might like:
Some Surprising Truths About Hunger And Satiety ← our main feature in which we examine the science of volumetrics, including a study that shows how water that is part of a food (but not served with a food) decreases caloric intake.
Another reason to enjoy melons!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: