For migrants, dementia can mean losing a language – and a whole world
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You may have lived in Australia for most of your adult life, speaking English every day. But if you acquired the language later in life and then develop dementia – a brain condition that affects thinking, memory and everyday function – you may lose fluency and find the language you spoke as a child takes over again.
For many migrants, this is the confronting reality. Language loss affects not only how they communicate with doctors and carers, but also how they connect with family, friends and the world around them.
More than one in four (28%) people living with dementia in Australia is from a culturally and linguistically diverse background.
This means language changes in dementia aren’t a niche issue – they affect thousands of families. It is estimated that 411,100 Australians were living with dementia in 2023.
How does dementia affect language?
Dementia can cause changes to speech and language, and these are often early symptoms. People may repeat themselves, have trouble finding the right word, switch topics unexpectedly or use words in unusual ways.
But these language changes can affect bi- or multilingual people differently.
Dementia usually affects the parts of the brain that store more recently acquired skills, including languages.
Languages learned during childhood are more deeply embedded in long-term memory than recently acquired skills.
This means someone who moved to Australia in their 20s and then learned English may lose their ability to speak it when they develop dementia later in life. But they may retain the ability to communicate in a first language – such as Italian, Arabic, Greek or Vietnamese – and revert to using only this.
Losing a second language means more than losing a skill. Migrants with dementia may be losing part of the life they’ve built, returning to a version of themselves from decades ago, which family and carers might not recognise.
The language gap in dementia care
While interpreters are widely available in aged care and to assist people with dementia, most lack specialised training.
Without this knowledge of dementia-specific communication, even skilled interpreters can struggle to communicate tone and meaning and recognise dementia symptoms.
Trained health interpreters are scarce outside major cities, and in regional areas family members are often heavily relied on.
But interpreting for a loved one with dementia is no easy task. Research shows family carers from culturally and linguistically diverse backgrounds face added stress thanks to language and cultural barriers. Many provide unpaid care and feel isolated.
For instance, a daughter caring for her mother with dementia might struggle to understand medical terms, while at the same time dealing with her own grief and exhaustion.
Some elderly people may also not want to discuss personal health details in front of their children or other relatives.
Burnout is a huge issue for family members and can sometimes lead to errors in care.
So, what works?
Evidence shows dementia-aware language services and culturally responsive care can help reduce stress for carers and improve quality of life for people living with dementia.
In a 2023 clinical trial, Australian researchers co-designed and evaluated specialist online training for interpreters. These included modules on dementia, aged care and cross-cultural communication.
The study found the training significantly improved the quality of interpreters’ communication during cognitive assessments of people with dementia, which are used to work out what supports someone might need.
This training has since been made available for free to all interpreters in Australia. At least 13% of the active interpreter workforce has completed it so far.
Dementia Support Australia also provides language support for people with dementia and their carers, arranging interpreters, translated materials, and Auslan services when needed.
There are also various initiatives in different states and territories, such as the “language buddies” program in Victoria which help people with dementia reconnect with community.
But we still need to do more
Despite these positive developments, there is still more to do to ensure diagnosis and support for people with dementia are not delayed due to cultural and language barriers.
We need to continue expanding supports, including:
- Specialist dementia training for interpreters: to handle repetitive speech, non-linear conversation and culturally specific expressions.
- Language and dementia awareness training for health workers: to understand why language loss happens and how to adapt care to address cognitive decline and also consider overall wellbeing.
- Better matching of interpreters: including age, dialect and cultural familiarity, especially in dementia-related contexts.
- Expanding the bilingual workforce: hiring more health-care workers who share the languages and cultures of local communities, particularly in rural, regional and remote areas.
- Culturally tailored dementia resources: booklets, videos, and support groups in multiple languages, co-designed with community members.
Fahad Hanna, Associate Professor in Public Health, Torrens University Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Cows’ Milk, Bird Flu, & You

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When it comes to dairy products, generally speaking, fermented ones (such as most cheeses and yogurts) are considered healthy in moderation, and unfermented ones have their pros and cons that can be argued and quibbled “until the cows come home”. We gave a broad overview, here:
Furthermore, you may recall that there’s some controversy/dissent about when human babies can have cows’ milk:
When can my baby drink cow’s milk? It’s sooner than you think
So, what about bird flu now?
Earlier this year, the information from the dairy industry was that it was nothing to be worried about for the time being:
Bird Flu Is Bad for Poultry and Dairy Cows. It’s Not a Dire Threat for Most of Us — Yet.
More recently, the latest science has found:
❝We found a first-order decay rate constant of −2.05 day–1 equivalent to a T99 of 2.3 days. Viral RNA remained detectable for at least 57 days with no degradation. Pasteurization (63 °C for 30 min) reduced infectious virus to undetectable levels and reduced viral RNA concentrations, but reduction was less than 1 log10.
The prolonged persistence of viral RNA in both raw and pasteurized milk has implications for food safety assessments and environmental surveillance❞
You can find the study here:
Infectivity and Persistence of Influenza A Virus in Raw Milk
In short: raw milk keeps the infectious virus; pasteurization appears to render it uninfectious, though viral RNA remains present.
This is relevant, because of the bird flu virus being found in milk:
World Health Organization | H5N1 strain of bird flu found in milk
To this end, a moratorium has been placed on the sale of raw milk, first by the California Dept of Public Health (following an outbreak in California):
California halts sales of raw milk due to bird flu virus contamination
And then, functionally, by the USDA, though rather than an outright ban, it’s requiring testing for the virus:
USDA orders testing of milk supply for presence of bird flu virus
So, is pasteurized milk safe?
The official answer to this, per the FDA, is… Honestly, a lot of hand-wringing and shrugging. What we do know is:
- the bird flu virus has been found in pasteurized milk too
- the test for this is very sensitive, and has the extra strength/weakness that viral fragments will flag it as a positive
- it is assumed that the virus was inactivated by the pasteurization process
- it could, however, have been the entire virus, the test simply does not tell us which
In the FDA’s own words:
❝The pasteurization process has served public health well for more than 100 years. Even if the virus is detected in raw milk, pasteurization is generally expected to eliminate pathogens to a level that does not pose a risk to consumer health❞
So, there we have it: the FDA does not have a reassurance exactly, but it does have a general expectation.
Source: US Officials: Bird flu viral fragments found in pasteurized milk
Want to know more?
You might like this mythbusting edition we did a little while back:
Pasteurization: What It Does And Doesn’t Do ← this is about its effect on risks and nutrients
Take care!
Share This Post
-

Resistance Is Useful! (Especially As We Get Older)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Resistance Is Useful!
At 10almonds we talk a lot about the importance of regular moderate exercise (e.g. walking, gardening, housework, etc), and with good reason: getting in those minutes (at least 150 minutes per week, so, a little over 20 minutes per day, or 25 minutes per day with one day off) is the exericise most consistently linked to better general health outcomes and reduced mortality risk.
We also often come back to mobility, because at the end of the day, being able to reach for something from a kitchen cabinet without doing oneself an injury is generally more important in life than being able to leg-press a car.
Today though, we’re going to talk about resistance training.
What is resistance training?
It can be weight-lifting, or it can be bodyweight exercises. In those cases, what you’re resisting is gravity. It can also be exercises with resistance bands or machines. In all cases, it’s about building and/or maintaining strength.
Why does it matter?
Let’s say you’re not an athlete, soldier, or laborer, and the heaviest thing you have to pick up is a bag of groceries. Strength still matters, for two main reasons:
- Muscle strength correlates to bone strength. You can’t build (or maintain) strong muscles on weak bones, so if you take care of your muscles, then your body will keep your bones strong too.
- That’s assuming you have a good diet as well—but today’s not about that. If you’d like to know more about eating for bone health though, do check out this previous article about that!
- Muscle strength correlates to balance and stability. You can’t keep yourself from falling over if you are physically frail.
Both of those things matter, because falls and fractures often have terrible health outcomes (e.g., slower recovery and more complications) the older we get. So, we want to:
- Ideally, not fall in the first place
- If we do fall, have robust bones
See also: Effects of Resistance Exercise on Bone Health
How much should we do?
Let’s go to the Journal of Strength and Conditioning Research on this one:
❝There is strong evidence to support the benefits of resistance exercise for countering many age-related processes of sarcopenia, muscle weakness, mobility loss, chronic disease, disability, and even premature mortality.
In addition, this Position Statement provides specific evidence-based practice recommendations to aid in the implementation of resistance exercise programs for healthy older adults and those with special considerations.
While there are instances where low-intensity, low-volume programs are appropriate (i.e., beginning programs for individuals with frailty or CVDs), the greatest benefits are possible with progression to moderate to higher intensity programs.❞
~ Fragala et al
Read the statement in full:
There’s a lot of science there and it’s well worth reading if you have the time. It’s particularly good at delineating how much is not enough vs how much is too much, and the extent to which we should (or shouldn’t) train to exhaustion.
If you don’t fancy that, though, and/or just want to start with something accessible and work your way up, the below is a very good (and also evidence-based) start-up plan:
Healthline’s Exercise Plan For Seniors—For Strength, Balance, & Flexibility
(it has a weekly planner, step-by-step guides to the exercises, and very clear illustrative animations of each)
Share This Post
- Muscle strength correlates to bone strength. You can’t build (or maintain) strong muscles on weak bones, so if you take care of your muscles, then your body will keep your bones strong too.
-
Make It Count: The Best Three Morning Stretches
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When you’ve just woken up, do you open your eyes, do a flip out of bed, land in a superhero pose, and do an hour of physical training? No?
The good news is, you don’t have to! Because even very short daily stretching sessions are more effective than occasional long ones:
Just do literally a few minutes (in total) each day!
Even just 20–30 seconds of each (each side) per day is enough for progress:
- Camel pose sweeps: dynamically stretch the hip flexors, abdominals, chest, and shoulders by sweeping one arm up while lifting your hips; this stimulates the nervous system by exposing vital organs, increasing adrenaline and energy*
- Lunge and hamstring sequence: start in a low lunge to open your hips and chest, then shift backwards into a hamstring stretch; alternate these movements to increase your flexibility and energy
- Twisting side body lift: seated with one leg bent, twist towards your bent leg, lift your hips and sweep your arm overhead, then lower into a side bend; this stretches the side of your body and boosts endorphin levels too, which is good at any time, but especially first thing in the morning
*The reason this works this way is because it counteracts fetal-like sleeping posture; mild activation of the nervous system mimics the body’s natural survival response, promoting alertness without real danger—basically, it’s the gentle yoga asana equivalent of a cold shower!
For more on all of these plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Stiff Joints? Do These 3 Stretches Every Morning To Avoid Pain ← an alternative set, if your goal for now is more restorative than progressive
Take care!
Share This Post

-

What are ‘collarium’ sunbeds? Here’s why you should stay away
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Reports have recently emerged that solariums, or sunbeds – largely banned in Australia because they increase the risk of skin cancer – are being rebranded as “collarium” sunbeds (“coll” being short for collagen).
Commercial tanning and beauty salons in Queensland, New South Wales and Victoria are marketing collariums, with manufacturers and operators claiming they provide a longer lasting tan and stimulate collagen production, among other purported benefits.
A collarium sunbed emits both UV radiation and a mix of visible wavelength colours to produce a pink or red light. Like an old-school sunbed, the user lies in it for ten to 20 minute sessions to quickly develop a tan.
But as several experts have argued, the providers’ claims about safety and effectiveness don’t stack up.
Why were sunbeds banned?
Commercial sunbeds have been illegal across Australia since 2016 (except for in the Northern Territory) under state-based radiation safety laws. It’s still legal to sell and own a sunbed for private use.
Their dangers were highlighted by young Australians including Clare Oliver who developed melanoma after using sunbeds. Oliver featured in the No Tan Is Worth Dying For campaign and died from her melanoma at age 26 in 2007.
Sunbeds lead to tanning by emitting UV radiation – as much as six times the amount of UV we’re exposed to from the summer sun. When the skin detects enough DNA damage, it boosts the production of melanin, the brown pigment that gives you the tanned look, to try to filter some UV out before it hits the DNA. This is only partially successful, providing the equivalent of two to four SPF.
Essentially, if your body is producing a tan, it has detected a significant amount of DNA damage in your skin.
Research shows people who have used sunbeds at least once have a 41% increased risk of developing melanoma, while ten or more sunbed sessions led to a 100% increased risk.
In 2008, Australian researchers estimated that each year, sunbeds caused 281 cases of melanoma, 2,572 cases of squamous cell carcinoma (another common type of skin cancer), and $3 million in heath-care costs, mostly to Medicare.
How are collarium sunbeds supposed to be different?
Australian sellers of collarium sunbeds imply they are safe, but their machine descriptions note the use of UV radiation, particularly UVA.
UVA is one part of the spectrum of UV radiation. It penetrates deeper into the skin than UVB. While UVB promotes cancer-causing mutations by discharging energy straight into the DNA strand, UVA sets off damage by creating reactive oxygen species, which are unstable compounds that react easily with many types of cell structures and molecules. These damage cell membranes, protein structures and DNA.
Evidence shows all types of sunbeds increase the risk of melanoma, including those that use only UVA.
Some manufacturers and clinics suggest the machine’s light spectrum increases UV compatibility, but it’s not clear what this means. Adding red or pink light to the mix won’t negate the harm from the UV. If you’re getting a tan, you have a significant amount of DNA damage.
Collagen claims
One particularly odd claim about collarium sunbeds is that they stimulate collagen.
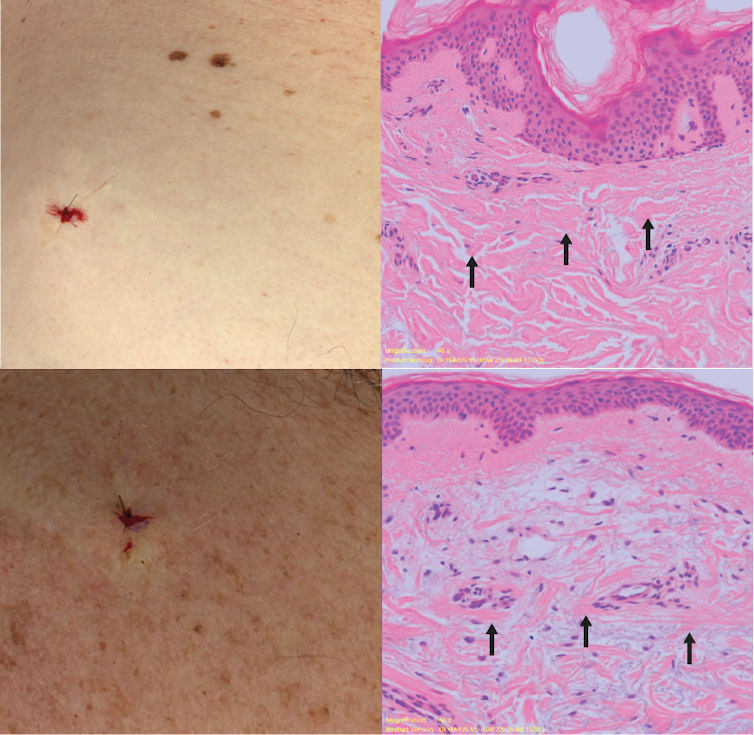
Collagen is the main supportive tissue in our skin. It provides elasticity and strength, and a youthful appearance. Collagen is constantly synthesised and broken down, and when the balance between production and recycling is lost, the skin loses strength and develops wrinkles. The collagen bundles become thin and fragmented. This is a natural part of ageing, but is accelerated by UV exposure.

Sun-protected skin (top) has thick bands of pink collagen (arrows) in the dermis, as seen on microscopic examination. Chronically sun-damaged skin (bottom) has much thinner collagen bands.
Katie Lee/UQThe reactive oxygen species generated by UVA light damage existing collagen structures and kick off a molecular chain of events that downgrades collagen-producing enzymes and increases collagen-destroying enzymes. Over time, a build-up of degraded collagen fragments in the skin promotes even more destruction.
While there is growing evidence red light therapy alone could be useful in wound healing and skin rejuvenation, the UV radiation in collarium sunbeds is likely to undo any benefit from the red light.
What about phototherapy?
There are medical treatments that use controlled UV radiation doses to treat chronic inflammatory skin diseases like psoriasis.
The anti-collagen effects of UVA can also be used to treat thickened scars and keloids. Side-effects of UV phototherapy include tanning, itchiness, dryness, cold sore virus reactivation and, notably, premature skin ageing.
These treatments use the minimum exposure necessary to treat the condition, and are usually restricted to the affected body part to minimise risks of future cancer. They are administered under medical supervision and are not recommended for people already at high risk of skin cancer, such as people with atypical moles.
So what happens now?
It looks like many collariums are just sunbeds rebranded with red light. Queensland Health is currently investigating whether these salons are breaching the state’s Radiation Safety Act, and operators could face large fines.
As the 2024 Australians of the Year – melanoma treatment pioneers Georgina Long and Richard Scolyer – highlighted in their acceptance speech, “there is nothing healthy about a tan”, and we need to stop glamorising tanning.
However, if you’re desperate for the tanned look, there is a safer and easy way to get one – out of a bottle or by visiting a salon for a spray tan.

Katie Lee, PhD Candidate, Dermatology Research Centre, The University of Queensland and Anne Cust, Professor of Cancer Epidemiology, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Older adults need another COVID-19 vaccine
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What you need to know
- The CDC recommends people 65 and older and immunocompromised people receive an additional dose of the updated COVID-19 vaccine this spring—if at least four months have passed since they received a COVID-19 vaccine.
- Updated COVID-19 vaccines are effective at protecting against severe illness, hospitalization, death, and long COVID.
- The CDC also shortened the isolation period for people who are sick with COVID-19.
Last week, the CDC said people 65 and older should receive an additional dose of the updated COVID-19 vaccine this spring. The recommendation also applies to immunocompromised people, who were already eligible for an additional dose.
Older adults made up two-thirds of COVID-19-related hospitalizations between October 2023 and January 2024, so enhancing protection for this group is critical.
The CDC also shortened the isolation period for people who are sick with COVID-19, although the contagiousness of COVID-19 has not changed.
Read on to learn more about the CDC’s updated vaccination and isolation recommendations.
Who is eligible for another COVID-19 vaccine this spring?
The CDC recommends that people ages 65 and older and immunocompromised people receive an additional dose of the updated COVID-19 vaccine this spring—if at least four months have passed since they received a COVID-19 vaccine. It’s safe to receive an updated COVID-19 vaccine from Pfizer, Moderna, or Novavax, regardless of which COVID-19 vaccines you received in the past.
Updated COVID-19 vaccines are available at pharmacies, local clinics, or doctor’s offices. Visit Vaccines.gov to find an appointment near you.
Under- and uninsured adults can get the updated COVID-19 vaccine for free through the CDC’s Bridge Access Program. If you’re over 60 and unable to leave your home, call the Aging Network at 1-800-677-1116 to learn about free at-home vaccination options.
What are the benefits of staying up to date on COVID-19 vaccines?
Staying up to date on COVID-19 vaccines prevents severe illness, hospitalization, death, and long COVID.
Additionally, the CDC says staying up to date on COVID-19 vaccines is a safer and more reliable way to build protection against COVID-19 than getting sick from COVID-19.
What are the new COVID-19 isolation guidelines?
According to the CDC’s general respiratory virus guidance, people who are sick with COVID-19 or another common respiratory illness, like the flu or RSV, should isolate until they’ve been fever-free for at least 24 hours without the use of fever-reducing medication and their symptoms improve.
After that, the CDC recommends taking additional precautions for the next five days: wearing a well-fitting mask, limiting close contact with others, and improving ventilation in your home if you live with others.
If you’re sick with COVID-19, you can infect others for five to 12 days, or longer. Moderately or severely immunocompromised patients may remain infectious beyond 20 days.
For more information, talk to your health care provider.
This article first appeared on Public Good News and is republished here under a Creative Commons license.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
How Many Heartbeats Do You Have Left?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our life is, of course, not literally measured in heartbeats—or at least not usefully so (since there are many other factors). However, there is a strong inverse correlation between resting heartrate and healthy longevity! That is to say, the slower your heart beats, the longer you’ll live.
Caveat: this is a generalization, and applies to a low resting heart rate that is the result of good cardiac health. It does not mean you should, for example, take up the use of heroin for its heartbeat-slowing effects. That will not help you to live longer!
Where’s the science?
Lest our opening claim there sound like popular wisdom rather than something backed by good science, let’s tend to that before moving on to the main thing today. There are, in fact, many papers to back up this claim, but here’s a good one:
It’s a 30-year longitudinal cohort study with 5,070 participants and baseline (as with most longitudinal studies, not everyone survived for the entire duration), and why we particularly like this one is not just its strong statistical significance, but also, because rather than simply looking at average resting heartrate and longevity, it also looked at changes in average resting heartrate and longevity, which makes the case for the link being causal much stronger.
❝In this study, we examined the association between resting heart rate and lifespan using linear regression in the Paris Prospective Study I, the Whitehall I Study, and the Framingham Heart Study. We used Cox proportional hazards regression to relate changes in heart rate over years to mortality risk.
We observed a statistically significant association between increases in resting heart rate over a 5-year period and risk of mortality in the Paris Prospective Study I (HR mortality per 10 bpm increase over time: 1.20; 95% CI: 1.13 to 1.27) and over an 8-year period in the Framingham Heart Study (HR: 1.13; 95% CI: 1.07 to 1.19 for men and HR: 1.09; 95% CI: 1.04 to 1.15 for women), after adjusting for classical risk factors and resting heart rate.
Our study shows that men and women who increase their resting heart rate over time increase their risk of mortality.❞
You may be wondering: why did we say 30 years, if the abstract is citing 5 years and 8 years?
And the answer is: it has to do with the statistical modeling used; the participants were followed for up to 30 years, but the statistical analysis allows us to look at what difference a change in resting heartrate makes over the course of 5 or 8 years, which is more illustrative for most people than “this is what will probably happen when you are [your age plus another 30 years]” statements. Indeed, the very fact that we can see a statistically significant change in mortality risk in just 5 years, makes it clear how big that risk is.
And how big is the risk? Translating the hazard ratios into percentages, we’re looking at, per 10 bpm increase over time, a 20% increase in mortality risk in the 5-year period per the Paris Prospective Study, or a 10%-ish increase in mortality risk in the 8-year period per the Framingham Heart Study. As for why the 5-year period has a bigger risk than the 8-year period, it’s likely down to a slightly different methodology and what other risk factors were controlled for.
One final note: about that “…and resting heart rate”, lest that seem confusing, we will mention that this too was controlled for because the primary input variable being looked at was the change in resting heartrate, not the resting heartrate itself.
In summary: if your resting heartrate increases, so does your mortality risk, at a rate of 10–20% over 5–8 years, for every 10 bpm increase (in other words: that stacks!).
So, what’s this about how many heartbeats we have left?
Based on the above, we can infer that since a change in heartrate is associated with an inverse change in longevity, the total number of heartbeats may often not change much, it’s just that the shorter-lived people squoze more heartbeats into less time.
With that in mind, a “common sense” logic tells us that we should conserve our heartbeats in order to live longer. This is somewhat consistent with the ideas behind some meditative practices.
However, while in a sense that’s not wrong (and such meditative practices can indeed help extend healthy lifespan), this presents an apparent paradox:
Should we avoid exercise, because it accelerates our heartrate while we are exercising?
And the robust answer is no, as some recent science by Dr. Kristel Janssens et al. shows clearly.
How it works: while exercise indeed speeds up the heartrate while exercising, it also lowers one’s resting heartrate by a sufficient amount (per metabolic equivalent of task minutes), that when all’s said and done, the hearts of those who regularly exercise beat fewer times per day than those who do not regularly exercise—and the difference isn’t small:
❝Athletes had an average heart rate of 68 beats per minute (bpm), while non-athletes had 76bpm. That translates to a total of 97,920 beats per day for athletes and 109,440 beats per day for non-athletes – around 10 percent less.❞
Note: that’s average heartrate, not average resting heartrate*. So it’s still counting all the heartbeats that happened during exercise, too. The athletes’ hearts were simply beating slowly enough the rest of the time to more than compensate.
*This is also worth bearing in mind because 68 bpm would be an astonishingly high resting heartrate for a very fit person.
Read the paper in full, here: Balancing Exercise Benefits Against Heartbeat Consumption in Elite Cyclists
Want to do more for your heart?
Check out:
How To Improve Your Heart Rate Variability
…for another thing to bear in mind (and helpfully, it’ll usually lower your resting heartrate, too).
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: