Finding Geriatric Doctors for Seniors
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝[Can you write about] the availability of geriatric doctors Sometimes I feel my primary isn’t really up on my 70 year old health issues. I would love to find a doctor that understands my issues and is able to explain them to me. Ie; my worsening arthritis in regards to food I eat; in regards to meds vs homeopathic solutions.! Thanks!❞
That’s a great topic, worthy of a main feature! Because in many cases, it’s not just about specialization of skills, but also about empathy, and the gap between studying a condition and living with a condition.
About arthritis, we’re going to do a main feature specifically on that quite soon, but meanwhile, you might like our previous article:
Keep Inflammation At Bay (arthritis being an inflammatory condition)
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Beat Food Addictions!

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When It’s More Than “Just” Cravings

This is Dr. Nicole Avena. She’s a research neuroscientist who also teaches at Mount Sinai School of Medicine, as well as at Princeton. She’s done a lot of groundbreaking research in the field of nutrition, diet, and addition, with a special focus on women’s health and sugar intake specifically.
What does she want us to know?
Firstly, that food addictions are real addictions.
We know it can sound silly, like the famous line from Mad Max:
❝Do not, my friends, become addicted to water. It will take hold of you and you will resent its absence!❞
As an aside, it is actually possible to become addicted to water; if one drinks it excessively (we are talking gallons every day) it does change the structure of the brain (no surprise; the brain is not supposed to have that much water!) causing structural damage that then results in dependency, and headaches upon withdrawal. It’s called psychogenic polydipsia:
But back onto today’s more specific topic, and by a different mechanism of addiction…
Food addictions are dopaminergic addictions (as is cocaine)
If you are addicted to a certain food (often sugar, but other refined carbs such as potato products, and also especially refined flour products, are also potential addictive substances), then when you think about the food in question, your brain lights up with more dopamine than it should, and you are strongly motivated to seek and consume the substance in question.
Remember, dopamine functions by expectation, not by result. So until your brain’s dopamine-gremlin is sated, it will keep flooding you with motivational dopamine; that’s why the first bite tastes best, then you wolf down the rest before your brain can change its mind, and afterwards you may be left thinking/feeling “was that worth it?”.
Much like with other addictions (especially alcohol), shame and regret often feature strongly afterwards, even accompanied by notions of “never again”.
But, binge-eating is as difficult to escape as binge-drinking.
You can break free, but you will probably have to take it seriously
Dr. Avena recommends treating a food addiction like any other addiction, which means:
- Know why you want to quit (make a list of the reasons, and this will help you stay on track later!)
- Make a conscious decision to genuinely quit
- Learn about the nature of the specific addiction (know thy enemy!)
- Choose a strategy (e.g. wean off vs cold turkey, and decide what replacements, if any, you will use)
- Get support (especially from those around you, and/but the support of others facing, or who have successfully faced, the same challenge is very helpful too)
- Keep track of your success (build and maintain a streak!)
- Lean into how you will better enjoy life without addiction to the substance (it never really made you happy anyway, so enjoy your newfound freedom and good health!)
Want more from Dr. Avena?
You can check out her column at Psychology Today here:
Psychology Today | Food Junkie ← it has a lot of posts about sugar addiction in particular, and gives a lot of information and practical advice
You can also read her book, which could be a great help if you are thinking of quitting a sugar addiction:
Sugarless: A 7-Step Plan to Uncover Hidden Sugars, Curb Your Cravings, and Conquer Your Addiction
Enjoy!
Share This Post
-

Sun-dried Tomatoes vs Black Olives – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing sun-dried tomatoes to black olives, we picked the sun-dried tomatoes.
Why?
These common snack-salad items may seem similar in consistency, but their macros are very different: the tomatoes, being dried, have proportionally a lot more protein, carbs, and fiber. The olives, meanwhile, have more fat (and/but yes, a very healthy blend of fats). Note that these comments are true for the things themselves; be aware that sun-dried tomatoes are often sold in vegetable oil, which would obviously change the macros considerably and be much less healthy. So, for the sake of statistics, we’re assuming you got sun-dried tomatoes that aren’t soaked in oil. All in all, we’re calling this category a win for the tomatoes, but those fats from the olives are very good too.
In terms of vitamins, the sun-dried tomatoes being dried again means that the loss of water weight means the vitamin content is proportionally much higher; the tomatoes are higher in vitamins A, B1, B2, B3, B5, B6, B9, C, and K, while olives are higher only in vitamin E (but in their defence, olives have 165x more vitamin E than sun-dried tomatoes). Still, a win for sun-dried tomatoes here.
When it comes to minerals, it’s a similar story for the same reason; the loss of water weight in the sun-dried tomatoes makes them much more nutritionally dense; they are higher in calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc, while the olives are higher only in sodium. Note, we’re looking at black olives today; green olives would be even higher in sodium than black ones, as they are “cured” for longer.
Lastly, in terms of polyphenols, they both have a lot of great things to bring, but sun-dried tomatoes are pretty much the richest natural source of lycopene, which itself a very powerful polyphenol even my general polyphenol standards, so we’d call this one a win for the sun-dried tomatoes too.
Want to learn more?
You might like to read:
Lycopene’s Benefits For The Gut, Heart, Brain, & More
Take care!
Share This Post
-

How worried should I be about cryptosporidiosis? Am I safe at the pool?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You might have heard of something called “cryptosporidiosis” recently, closely followed by warnings to stay away from your local swimming pool if you’ve had diarrhoea.
More than 700 cases of this gastrointestinal disease were reported in Queensland in January, which is 13 times more than in January last year. Just under 500 cases have been recorded in New South Wales this year to-date, while other states have similarly reported an increase in the number of cryptosporidiosis infections in recent months.
Cryptosporidiosis has been listed as a national notifiable disease in Australia since 2001.
But what exactly is it, and should we be worried?What causes cryptosporidiosis, and who is affected?
Cryptosporidiosis is the disease caused by the parasite Cryptosporidium, of which there are two types that can make us sick. Cryptosporidum hominis only affects humans and is the major cause of recent outbreaks in Australia, while Cryptosporidium parvum can also affect animals.
The infection is spread by spores called oocysts in the stools of humans and animals. When ingested, these oocysts migrate and mature in the small bowel. They damage the small bowel lining and can lead to diarrhoea, nausea, vomiting, fever and abdominal discomfort.
Most people develop symptoms anywhere from one to 12 days after becoming infected. Usually these symptoms resolve within two weeks, but the illness may last longer and can be severe in those with a weakened immune system.
Children and the elderly tend to be the most commonly affected. Cryptosporidiosis is more prevalent in young children, particularly those under five, but the disease can affect people of any age.

A number of public pools have been closed lately due to cryptosporidiosis outbreaks.
LBeddoe/ShutterstockSo how do we catch it?
Most major outbreaks of cryptosporidiosis have been due to people drinking contaminated water. The largest recorded outbreak occurred in Milwaukee in 1993 where 403,000 people were believed to have been infected.
Cryptosporidium oocysts are very small in size and in Milwaukee they passed through the filtration system of one of the water treatment plants undetected, infecting the city’s water supply. As few as ten oocysts can cause infection, making it possible for contaminated drinking water to affect a very large number of people.
Four days after infection a person with cryptosporidiosis can shed up to ten billion oocysts into their stool a day, with the shedding persisting for about two weeks. This is why one infected person in a swimming pool can infect the entire pool in a single visit.
Cryptosporidium oocysts excreted in the faeces of infected humans and animals can also reach natural bodies of water such as beaches, rivers and lakes directly through sewer pipes or indirectly such as in manure transported with surface runoff after heavy rain.
One study which modelled Cryptosporidium concentrations in rivers around the world estimated there are anywhere from 100 to one million oocysts in a litre of river water.
In Australia, cryptosporidiosis outbreaks tend to occur during the late spring and early summer periods when there’s an increase in recreational water activities such as swimming in natural water holes, water catchments and public pools. We don’t know exactly why cases have seen such a surge this summer compared to other years, but we know Cryptosporidium is very infectious.
Oocysts have been found in foods such as fresh vegetables and seafood but these are not common sources of infection in Australia.
What about chlorine?
Contrary to popular belief, chlorine doesn’t kill off all infectious microbes in a swimming pool. Cryptosporidium oocysts are hardy, thick-walled and resistant to chlorine and acid. They are not destroyed by chlorine at the normal concentrations found in swimming pools.
We also know oocysts can be significantly protected from the effects of chlorine in swimming pools by faecal material, so the presence of even small amounts of faecal matter contaminated with Cryptosporidium in a swimming pool would necessitate closure and a thorough decontamination.
Young children and in particular children in nappies are known to increase the potential for disease transmission in recreational water. Proper nappy changing, frequent bathroom breaks and showering before swimming to remove faecal residue are helpful ways to reduce the risk.
Cryptosporidium can spread in other bodies of water, not just swimming pools.
Yulia Simonova/ShutterstockSome sensible precautions
Other measures you can take to reduce yours and others’ risk of cryptosporidiosis include:
- avoid swimming in natural waters such as rivers and creeks during and for at least three days after heavy rain
- avoid swimming in beaches for at least one day after heavy rain
- avoid drinking untreated water such as water from rivers or springs. If you need to drink untreated water, boiling it first will kill the Cryptosporidium
- avoid swallowing water when swimming if you can
- if you’ve had diarrhoea, avoid swimming for at least two weeks after it has resolved
- avoid sharing towels or linen for at least two weeks after diarrhoea has resolved
- avoid sharing, touching or preparing food that other people may eat for at least 48 hours after diarrhoea has resolved
- wash your hands with soap and water after going to the bathroom or before preparing food (Cryptosporidium is not killed by alcohol gels and sanitisers).
Not all cases of diarrhoea are due to cryptosporidiosis. There are many other causes of infectious gastroenteritis and because the vast majority of the time recovery is uneventful you don’t need to see a doctor unless very unwell. If you do suspect you may have cryptosporidiosis you can ask your doctor to refer you for a stool test.

Vincent Ho, Associate Professor and clinical academic gastroenterologist, Western Sydney University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post



Related Posts
-
Over 50? Do These 3 Stretches Every Morning To Avoid Pain
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
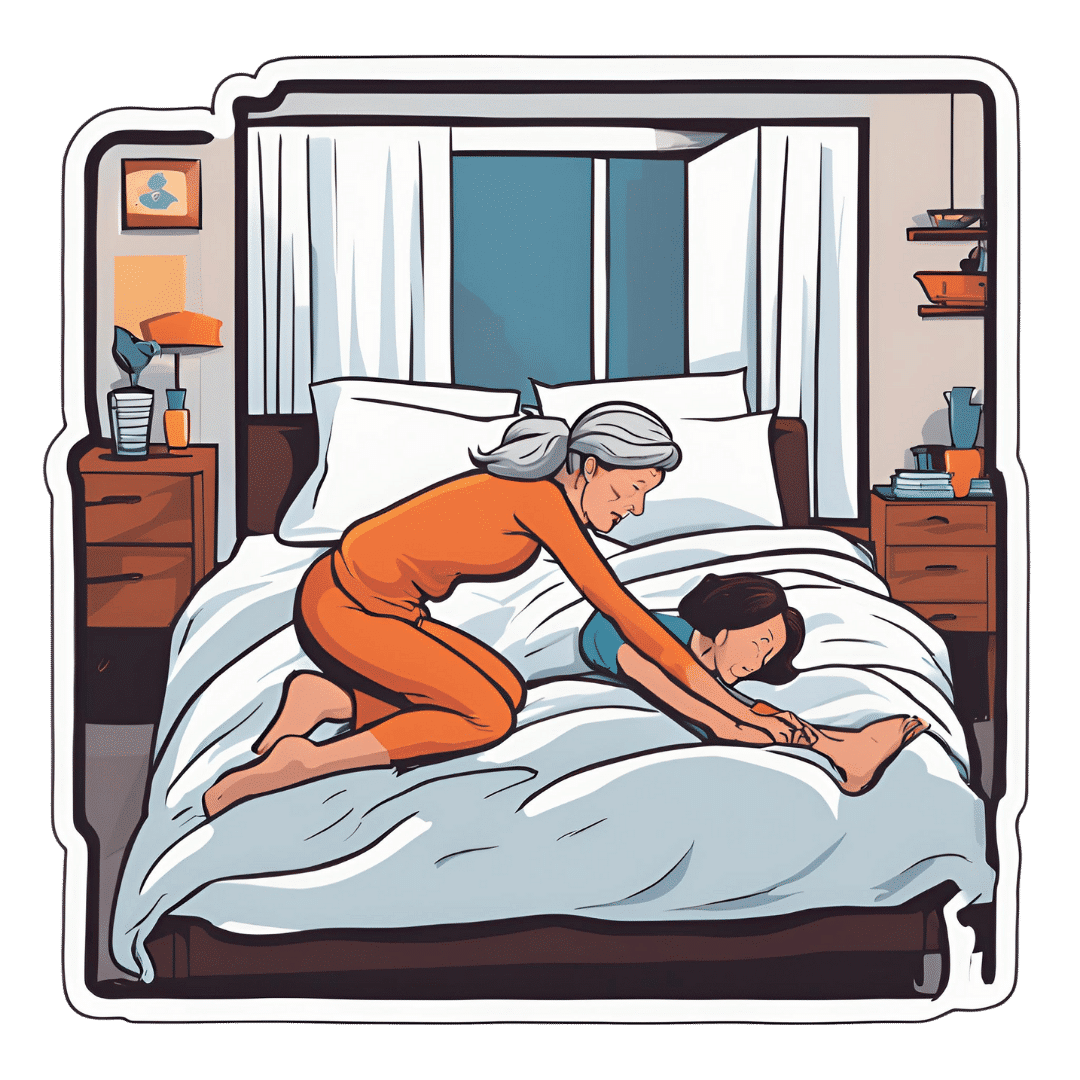
Will Harlow, over-50s specialist physiotherapist, recommends these three stretches be done daily for cumulative benefits over time, especially if you have arthritis, stiff joints, or similar morning pain:
The good-morning routine
These stretches are designed for people with arthritis and stiff joints, but if you experience any extra pain, or are aware of having some musculoskeletal irregularity, do seek professional advice (such as from a local physiotherapist). Otherwise, the three stretches he recommends are:
Quad hip flexor stretch
This one is performed while lying on your side in bed:
- Bring the top leg up toward your body, grab the shin, and pull the leg backward to stretch.
- Feel the stretch in the front of the leg (quadriceps and hip flexor).
- Hold for 30 seconds and repeat on both sides.
- Use a towel or band if you can’t reach your shin.
Book-opener
This one helps improve mobility in the lower and mid-back:
- Lie on your side with arms at a 90-degree angle in front of your body.
- Roll backward, opening the top arm while keeping legs in place.
- Hold for 20–30 seconds or repeat the movement several times.
- Optionally, allow your head to rotate for a neck stretch.
Calf stretch with chest-opener
This one combines a calf and chest stretch:
- Stand in a lunged position, keeping the back leg straight and heel down for the calf stretch.
- Place hands behind your head, open elbows, and lift your head slightly for a chest stretch.
- Hold for 20–30 seconds, then switch legs.
For more on all the above plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Do You Believe In Magic? – by Dr. Paul Offit
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Here at 10almonds, we like to examine and present the science wherever it leads, so this book was an interesting read.
Dr. Offit, himself a much-decorated vaccine research scientist, and longtime enemy of the anti-vax crowd, takes aim at alternative therapies in general, looking at what does work (and how), and what doesn’t (and what harm it can cause).
The style of the book is largely polemic in tone, but there’s lots of well-qualified information and stats in here too. And certainly, if there are alternative therapies you’ve left unquestioned, this book will probably prompt questions, at the very least.
And science, of course, is about asking questions, and shouldn’t be afraid of such! Open-minded skepticism is a key starting point, while being unafraid to actually reach a conclusion of “this is probably [not] so”, when and if that’s where the evidence brings us. Then, question again when and if new evidence comes along.
To that end, Dr. Offit does an enthusiastic job of looking for answers, and presenting what he finds.
If the book has downsides, they are primarily twofold:
- He is a little quick to dismiss the benefits of a good healthy diet, supplemented or otherwise.
- His keenness here seems to step from a desire to ensure people don’t skip life-saving medical treatments in the hope that their diet will cure their cancer (or liver disease, or be it what it may), but in doing so, he throws out a lot of actually good science.
- He—strangely—lumps menopausal HRT in with alternative therapies, and does the exact same kind of anti-science scaremongering that he rails against in the rest of the book.
- In his defence, this book was published ten years ago, and he may have been influenced by a stack of headlines at the time, and a popular celebrity endorsement of HRT, which likely put him off it.
Bottom line: there’s something here to annoy everyone—which makes for stimulating reading.
Click here to check out Do You Believe In Magic, and expand your knowledge!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
- He is a little quick to dismiss the benefits of a good healthy diet, supplemented or otherwise.
-

The New Menopause – by Dr. Mary Claire Haver
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The author is most famous for “The Galveston Diet”, which book is astonishingly similar in its content, chapters, format, etc to Nikki Williams’ “It’s Not You, It’s Your Hormones” which came out a few years previously but didn’t get the same marketing.
Nonetheless, this time Dr. Haver has something new to add, and we think it’s worth a read.
The general theme of this book is a comprehensive overview of the menopause, experientially (subjective to the person going through it) and empirically (by science), from start to finish and beyond. This book’s more about human physiology, and less about diet than the previous.
Dr. Haver also discusses in-depth how estrogen is thought of as a sex hormone (and it is), to the point that people consider it perhaps expendable, and forget (or are simply unaware) that we have estrogen receptors throughout our bodies and estrogen is vital for maintaining many other bodily functions, including your heart, cognitive function, bone integrity, blood sugar balance, and more.
(in case you’re wondering “why don’t men fall to bits, then?”, don’t worry, their testosterone does these things for them. Testosterone is orders of magnitude less potent than estrogen, mg for mg, so they need a lot more of it, but under good conditions they produce plenty so it’s fine)
But, the amount of testosterone available to peri/postmenopausal women is simply not enough to do that job (and it’d also result in a transition of secondary sex characteristics, which for most people would be very unwanted), so, something else needs to be done.
Dr. Haver also discusses in detail the benefits and risks of HRT and how to get/manage them, respectively, with the latest up-to-date research (at time of going to print; the book was published in April 2024).
Bottom line: if you want to know what’s going on with your peri- or post-menopausal body and how it could be better (or if you want to know what’s going on with someone else approaching/experiencing menopause), then this is a top-tier book.
Click here to check out The New Menopause, and know what’s going on and what to do about it!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: