Shrimp vs Caviar – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing shrimp to caviar, we picked the caviar.
Why?
Both of these seafoods share a common history (also shared with lobster, by the way) of “nutrient-dense peasant-food that got gentrified and now it’s more expensive despite being easier to source”. But, cost and social quirks aside, what are their strengths and weaknesses?
In terms of macros, both are high in protein, but caviar is much higher in fat. You may be wondering: are the fats healthy? And the answer is that it’s a fairly even mix between monounsaturated (healthy), polyunsaturated (healthy), and saturated (unhealthy). The fact that caviar is generally enjoyed in very small portions is its saving grace here, but quantity for quantity, shrimp is the natural winner on macros.
…unless we take into account the omega-3 and omega-6 balance, in which case, it’s worthy of note that caviar has more omega-3 (which most people could do with consuming more of) while shrimp has more omega-6 (which most people could do with consuming less of).
When it comes to vitamins, caviar has more of vitamins A, B1, B2, B5, B6, B9, B12, D, K, and choline; nor are the margins small in most cases, being multiples (or sometimes, tens of multiples) higher. Shrimp, meanwhile, boasts only more vitamin B3.
In the category of minerals, caviar leads with more calcium, iron, magnesium, manganese, phosphorus, potassium, and selenium, while shrimp has more copper and zinc.
All in all, while shrimp has its benefits for being lower in fat (and thus also, for those whom that may interest, lower in calories), caviar wins the day by virtue of its overwhelming nutritional density.
Want to learn more?
You might like to read:
What Omega-3 Fatty Acids Really Do For Us
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Nutrition To Combat Lymphedema & Lipedema

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Kelly Sturm is a rehab specialist (Doctor of Physical Therapy), and also a certified lymphedema therapist. Here’s what helps her patients with lymphedema and lipedema:
Don’t fan the flames
Lymphedema and lipedema are inflammatory lymphatic diseases affecting mostly women. As such, an anti-inflammatory diet will be important, but there are other factors too:
- Anti-inflammatory diet: this is to reduce the chronic inflammation associated with lymphatic diseases. This means eating plenty of fruit and vegetables, especially berries and leafy greens, and avoiding things like sugar, alcohol, caffeine, and processed foods. And of course, don’t smoke.
- Intermittent fasting: this also helps by giving the body a chance to correct itself; when the body isn’t digesting food, it has a lot more resources to devote to its favorite activity: maintenance. This results in lower inflammation, and better fat redistribution.
- Weight loss: not a bandwagon we often get on at 10almonds as it’s rarely the most important thing, but in this case it is of high importance (second only to dealing with the inflammation), as excess weight around the lymph nodes and vessels can lead to dysfunction and swelling. Thus, reducing the weight can ease that and allow the body to heal.
For more details on all of the above, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- Eat To Beat Inflammation ← also some non-dietary advice in there too
- Ask Not What Your Lymphatic System Can Do For You…
- Lose Weight, But Healthily ← more useful than just trying to run a calorie deficit
Take care!
Share This Post
-

Women and Minorities Bear the Brunt of Medical Misdiagnosis
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Charity Watkins sensed something was deeply wrong when she experienced exhaustion after her daughter was born.
At times, Watkins, then 30, had to stop on the stairway to catch her breath. Her obstetrician said postpartum depression likely caused the weakness and fatigue. When Watkins, who is Black, complained of a cough, her doctor blamed the flu.
About eight weeks after delivery, Watkins thought she was having a heart attack, and her husband took her to the emergency room. After a 5½-hour wait in a North Carolina hospital, she returned home to nurse her baby without seeing a doctor.
When a physician finally examined Watkins three days later, he immediately noticed her legs and stomach were swollen, a sign that her body was retaining fluid. After a chest X-ray, the doctor diagnosed her with heart failure, a serious condition in which the heart becomes too weak to adequately pump oxygen-rich blood to organs throughout the body. Watkins spent two weeks in intensive care.
She said a cardiologist later told her, “We almost lost you.”
Watkins is among 12 million adults misdiagnosed every year in the U.S.
In a study published Jan. 8 in JAMA Internal Medicine, researchers found that nearly 1 in 4 hospital patients who died or were transferred to intensive care had experienced a diagnostic error. Nearly 18% of misdiagnosed patients were harmed or died.
In all, an estimated 795,000 patients a year die or are permanently disabled because of misdiagnosis, according to a study published in July in the BMJ Quality & Safety periodical.
Some patients are at higher risk than others.
Women and racial and ethnic minorities are 20% to 30% more likely than white men to experience a misdiagnosis, said David Newman-Toker, a professor of neurology at Johns Hopkins School of Medicine and the lead author of the BMJ study. “That’s significant and inexcusable,” he said.
Researchers call misdiagnosis an urgent public health problem. The study found that rates of misdiagnosis range from 1.5% of heart attacks to 17.5% of strokes and 22.5% of lung cancers.
Weakening of the heart muscle — which led to Watkins’ heart failure — is the most common cause of maternal death one week to one year after delivery, and is more common among Black women.
Heart failure “should have been No. 1 on the list of possible causes” for Watkins’ symptoms, said Ronald Wyatt, chief science and chief medical officer at the Society to Improve Diagnosis in Medicine, a nonprofit research and advocacy group.
Maternal mortality for Black mothers has increased dramatically in recent years. The United States has the highest maternal mortality rate among developed countries. According to the Centers for Disease Control and Prevention, non-Hispanic Black mothers are 2.6 times as likely to die as non-Hispanic white moms. More than half of these deaths take place within a year after delivery.
Research shows that Black women with childbirth-related heart failure are typically diagnosed later than white women, said Jennifer Lewey, co-director of the pregnancy and heart disease program at Penn Medicine. That can allow patients to further deteriorate, making Black women less likely to fully recover and more likely to suffer from weakened hearts for the rest of their lives.
Watkins said the diagnosis changed her life. Doctors advised her “not to have another baby, or I might need a heart transplant,” she said. Being deprived of the chance to have another child, she said, “was devastating.”
Racial and gender disparities are widespread.
Women and minority patients suffering from heart attacks are more likely than others to be discharged without diagnosis or treatment.
Black people with depression are more likely than others to be misdiagnosed with schizophrenia.
Minorities are less likely than whites to be diagnosed early with dementia, depriving them of the opportunities to receive treatments that work best in the early stages of the disease.
Misdiagnosis isn’t new. Doctors have used autopsy studies to estimate the percentage of patients who died with undiagnosed diseases for more than a century. Although those studies show some improvement over time, life-threatening mistakes remain all too common, despite an array of sophisticated diagnostic tools, said Hardeep Singh, a professor at Baylor College of Medicine who studies ways to improve diagnosis.
“The vast majority of diagnoses can be made by getting to know the patient’s story really well, asking follow-up questions, examining the patient, and ordering basic tests,” said Singh, who is also a researcher at Houston’s Michael E. DeBakey VA Medical Center. When talking to people who’ve been misdiagnosed, “one of the things we hear over and over is, ‘The doctor didn’t listen to me.’”
Racial disparities in misdiagnosis are sometimes explained by noting that minority patients are less likely to be insured than white patients and often lack access to high-quality hospitals. But the picture is more complicated, said Monika Goyal, an emergency physician at Children’s National Hospital in Washington, D.C., who has documented racial bias in children’s health care.
In a 2020 study, Goyal and her colleagues found that Black kids with appendicitis were less likely than their white peers to be correctly diagnosed, even when both groups of patients visited the same hospital.
Although few doctors deliberately discriminate against women or minorities, Goyal said, many are biased without realizing it.
“Racial bias is baked into our culture,” Goyal said. “It’s important for all of us to start recognizing that.”
Demanding schedules, which prevent doctors from spending as much time with patients as they’d like, can contribute to diagnostic errors, said Karen Lutfey Spencer, a professor of health and behavioral sciences at the University of Colorado-Denver. “Doctors are more likely to make biased decisions when they are busy and overworked,” Spencer said. “There are some really smart, well-intentioned providers who are getting chewed up in a system that’s very unforgiving.”
Doctors make better treatment decisions when they’re more confident of a diagnosis, Spencer said.
In an experiment, researchers asked doctors to view videos of actors pretending to be patients with heart disease or depression, make a diagnosis, and recommend follow-up actions. Doctors felt far more certain diagnosing white men than Black patients or younger women.
“If they were less certain, they were less likely to take action, such as ordering tests,” Spencer said. “If they were less certain, they might just wait to prescribe treatment.”
It’s easy to see why doctors are more confident when diagnosing white men, Spencer said. For more than a century, medical textbooks have illustrated diseases with stereotypical images of white men. Only 4.5% of images in general medical textbooks feature patients with dark skin.
That may help explain why patients with darker complexions are less likely to receive a timely diagnosis with conditions that affect the skin, from cancer to Lyme disease, which causes a red or pink rash in the earliest stage of infection. Black patients with Lyme disease are more likely to be diagnosed with more advanced disease, which can cause arthritis and damage the heart. Black people with melanoma are about three times as likely as whites to die within five years.
The covid-19 pandemic helped raise awareness that pulse oximeters — the fingertip devices used to measure a patient’s pulse and oxygen levels — are less accurate for people with dark skin. The devices work by shining light through the skin; their failures have delayed critical care for many Black patients.
Seven years after her misdiagnosis, Watkins is an assistant professor of social work at North Carolina Central University in Durham, where she studies the psychosocial effects experienced by Black mothers who survive severe childbirth complications.
“Sharing my story is part of my healing,” said Watkins, who speaks to medical groups to help doctors improve their care. “It has helped me reclaim power in my life, just to be able to help others.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Share This Post
-
Over-50s Physio: What My 5 Oldest Patients (Average Age 92) Do Right
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Oftentimes, people of particularly advanced years will be asked their secret to longevity, and sometimes the answers aren’t that helpful because they don’t actually know, and ascribe it to some random thing. Will Harlow, the over-50s specialist physio, talks about the top 5 science-based things that his 5 oldest patients do, that enhances the healthy longevity that they are enjoying:
The Top 5’s Top 5
Here’s what they’re doing right:
Daily physical activity: all five patients maintain a consistent habit of daily exercise, which includes activities like exercise classes, home workouts, playing golf, or taking daily walks. They prioritize movement even when it’s difficult, rarely skipping a day unless something serious happened. A major motivator was the fear of losing mobility, as they had seen spouses, friends, or family members stop exercising and never start again.
Prioritize sleep (but not too much): the patients each average seven hours of sleep per night, aligning with research suggesting that 7–9 hours of sleep is ideal for health. They maintain consistent sleep and wake-up times, which contributes to their well-being. While they allow themselves short naps when needed, they avoid long afternoon naps to avoid disrupting their sleep patterns.
Spend time in nature: spending time outdoors is a priority for all five individuals. Whether through walking, gardening, or simply sitting on a park bench, they make it a habit to connect with nature. This aligns with studies showing that time spent in natural environments, especially near water, significantly reduces stress. When water isn’t accessible, green spaces still provide a beneficial boost to mental health.
Stick to a routine: the patients all value simple daily routines, such as enjoying an evening cup of tea, taking a daily walk, or committing to small gardening tasks. These routines offer mental and physical grounding, providing stability even when life becomes difficult sometimes. They emphasized the importance of keeping routines simple and manageable to ensure they could stick to them regardless of life’s challenges.
Stay curious: a shared trait among the patients was their curiosity and eagerness to learn. They enjoy meeting new people, exploring new experiences, and taking on new challenges. Two of them attended the University of the Third Age to learn new skills, while another started playing bridge as a new hobby. The remaining two have recently made new friends. They all maintain a playful attitude, a good sense of humor, and aren’t afraid to fail or laugh at themselves.
For more on each of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Top 8 Habits Of The Top 1% Healthiest Over-50s ← another approach to the same question, this time with a larger sample size, and/but many younger (than 90s) respondents.
Take care!
Share This Post

Related Posts
-

Migraine Mythbusting
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Migraine: When Headaches Are The Tip Of The Neurological Iceberg

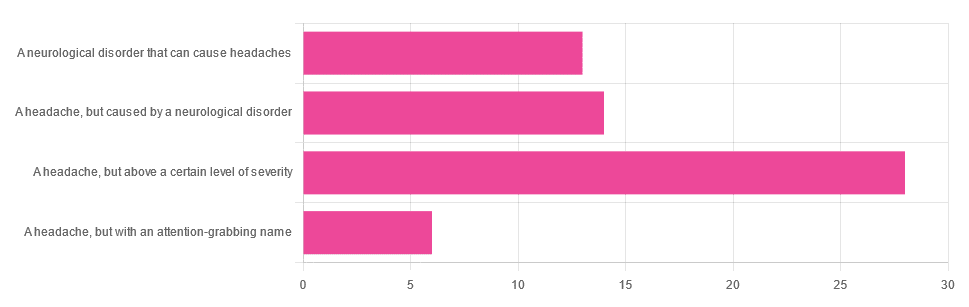
Yesterday, we asked you “What is a migraine?” and got the above-depicted, below-described spread of responses:
- Just under 46% said “a headache, but above a certain level of severity”
- Just under 23% said “a headache, but caused by a neurological disorder”
- Just over 21% said “a neurological disorder that can cause headaches”
- Just under 10% said “a headache, but with an attention-grabbing name”
So… What does the science say?
A migraine is a headache, but above a certain level of severity: True or False?
While that’s usually a very noticeable part of it… That’s only one part of it, and not a required diagnostic criterion. So, in terms of defining what a migraine is, False.
Indeed, migraine may occur without any headache, let alone a severe one, for example: Abdominal Migraine—though this is much less well-researched than the more common with-headache varieties.
Here are the defining characteristics of a migraine, with the handy mnemonic 5-4-3-2-1:
- 5 or more attacks
- 4 hours to 3 days in duration
- 2 or more of the following:
- Unilateral (affects only one side of the head)
- Pulsating
- Moderate or severe pain intensity
- Worsened by or causing avoidance of routine physical activity
- 1 or more of the following:
- Nausea and/or vomiting
- Sensitivity to both light and sound
Source: Cephalalgia | ICHD-II Classification: Parts 1–3: Primary, Secondary and Other
As one of our subscribers wrote:
❝I have chronic migraine, and it is NOT fun. It takes away from my enjoyment of family activities, time with friends, and even enjoying alone time. Anyone who says a migraine is just a bad headache has not had to deal with vertigo, nausea, loss of balance, photophobia, light sensitivity, or a host of other symptoms.❞
Migraine is a neurological disorder: True or False?
True! While the underlying causes aren’t known, what is known is that there are genetic and neurological factors at play.
❝Migraine is a recurrent, disabling neurological disorder. The World Health Organization ranks migraine as the most prevalent, disabling, long-term neurological condition when taking into account years lost due to disability.
Considerable progress has been made in elucidating the pathophysiological mechanisms of migraine, associated genetic factors that may influence susceptibility to the disease❞
Source: JHP | Mechanisms of migraine as a chronic evolutive condition
Migraine is just a headache with a more attention-grabbing name: True or False?
Clearly, False.
As we’ve already covered why above, we’ll just close today with a nod to an old joke amongst people with chronic illnesses in general:
“Are you just saying that because you want attention?”
“Yes… Medical attention!”
Want to learn more?
You can find a lot of resources at…
NIH | National Institute of Neurological Disorders & Stroke | Migraine
and…
The Migraine Trust ← helpfully, this one has a “Calm mode” to tone down the colorscheme of the website!
Particularly useful from the above site are its pages:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Avoid This Food To Avoid IBS
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
If you have inflammatory bowel syndrome (IBS), including ulcerative colitis, Crohn’s disease, or similar, then suddenly a lot of common dietary advice gets flipped on its head:
While resistant starches and the like (so, doing the job of fiber; see: When Is A Fiber Not A Fiber? When It’s A Resistant Starch) making it to the end parts of our digestive tract is good for our bacteria there, in the case of people with IBS or similar, it can be a bit too good for our bacteria there.
As a result, a common understanding is “if you have IBS, you mustn’t eat fiber” which is understandable—but incorrect—advice. More on that in the “Learn more” bit at the bottom, but for now…
What’s the actual biggest driver of IBS?
Another reason to skip red meat
Researchers (Dr. Chunbao Li et al.) noted that relevant epidemiological studies (of which, The China Study is the most famous, but there are countless others) have long shown a strong association between red meat consumption and the development of IBS, and wanted to ascertain how exactly this happened.
This is critical, because while epidemiological studies can present an overwhelming amount of evidence for association/correlation, they cannot outright prove causality.
So, they did a mouse study (mice are opportunistic omnivores like us, indeed often eating our* food, and as a result, have very similar gut microbiota), experimenting with dietary modifications, and then measuring colonic inflammation.
*The mice may disagree, and contest that it is we who are eating their food. But they are free to argue that in their own publication.
What they (the researchers, not the mice) did: they fed the mice red meat diets (beef, pork, lamb) or control for 2 weeks, followed by an induction of colitis.
What they found: red meat diets (all of them) worsened colonic inflammation, increased pro-inflammatory cytokines, and caused neutrophil and macrophage infiltration.
Specifically: red meat intake (any) decreased beneficial bacteria (Streptococcus, Akkermansia, Faecalibacterium, Lactococcus) and increased harmful ones (Clostridium, Mucispirillum).
There were some differences between the three red meats (beef, pork, lamb), but the differences pertained more to variations within:
- which beneficial bacteria were decreased the most
- which harmful bacteria were increased the most
You can see the exact results (including: per meat type and per bacterial strain) in the paper, here: Red Meat Diet Exacerbates Colitis by Promoting the Accumulation of Myeloid Cells and Disrupting Gut Microbiota
This dysbiosis (that is to say: disruption of the gut microbiome) then led to an overproduction of pro-inflammatory cytokines and infiltration of immune cells in the colon.
In other words, it inflamed the bowel—that is to say, promoted inflammatory bowel syndrome.
Want to learn more?
Check out:
Fruit, Fiber, & Leafy Greens… On A Low-FODMAP Diet!
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What does it mean to be transgender?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Transgender media coverage has surged in recent years for a wide range of reasons. While there are more transgender television characters than ever before, hundreds of bills are targeting transgender people’s access to medical care, sports teams, gender-specific public spaces, and other institutions.
Despite the increase in conversation about the transgender community, public confusion around transgender identity remains.
Read on to learn more about what it means to be transgender and understand challenges transgender people may face.
What does it mean to be transgender?
Transgender—or “trans”—is an umbrella term for people whose gender identity or gender expression does not conform to their sex assigned at birth. People can discover they are trans at any age.
Gender identity refers to a person’s inner sense of being a woman, a man, neither, both, or something else entirely. Trans people who don’t feel like women or men might describe themselves as nonbinary, agender, genderqueer, or two-spirit, among other terms.
Gender expression describes the way a person communicates their gender through their appearance—such as their clothing or hairstyle—and behavior.
A person whose gender expression doesn’t conform to the expectations of their assigned sex may not identify as trans. The only way to know for sure if someone is trans is if they tell you.
Cisgender—or “cis”—describes people whose gender identities match the sex they were assigned at birth.
How long have transgender people existed?
Being trans isn’t new. Although the word “transgender” only dates back to the 1960s, people whose identities defy traditional gender expectations have existed across cultures throughout recorded history.
How many people are transgender?
A 2022 Williams Institute study estimates that 1.6 million people over the age of 13 identify as transgender in the United States.
Is being transgender a mental health condition?
No. Conveying and communicating about your gender in a way that feels authentic to you is a normal and necessary part of self-expression.
Social and legal stigma, bullying, discrimination, harassment, negative media messages, and barriers to gender-affirming medical care can cause psychological distress for trans people. This is especially true for trans people of color, who face significantly higher rates of violence, poverty, housing instability, and incarceration—but trans identity itself is not a mental health condition.
What is gender dysphoria?
Gender dysphoria describes a feeling of unease that some trans people experience when their perceived gender doesn’t match their gender identity, or their internal sense of gender. A 2021 study of trans adults pursuing gender-affirming medical care found that most participants started experiencing gender dysphoria by the time they were 7.
When trans people don’t receive the support they need to manage gender dysphoria, they may experience depression, anxiety, social isolation, suicidal ideation, substance use disorder, eating disorders, and self-injury.
How do trans people manage gender dysphoria?
Every trans person’s experience with gender dysphoria is unique. Some trans people may alleviate dysphoria by wearing gender-affirming clothing or by asking others to refer to them by a new name and use pronouns that accurately reflect their gender identity. The 2022 U.S. Trans Survey found that nearly all trans participants who lived as a different gender than the sex they were assigned at birth reported that they were more satisfied with their lives.
Some trans people may also manage dysphoria by pursuing medical transition, which may involve taking hormones and getting gender-affirming surgery.
Access to gender-affirming medical care has been shown to reduce the risk of depression and suicide among trans youth and adults.
To learn more about the trans community, visit resources from the National Center for Transgender Equality, the Trevor Project, PFLAG, and Planned Parenthood.
If you or anyone you know is considering suicide or self-harm or is anxious, depressed, upset, or needs to talk, call the Suicide & Crisis Lifeline at 988 or text the Crisis Text Line at 741-741. For international resources, here is a good place to begin.
This article first appeared on Public Good News and is republished here under a Creative Commons license.

Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: