Cupping: How It Works (And How It Doesn’t)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Good Health By The Cup?
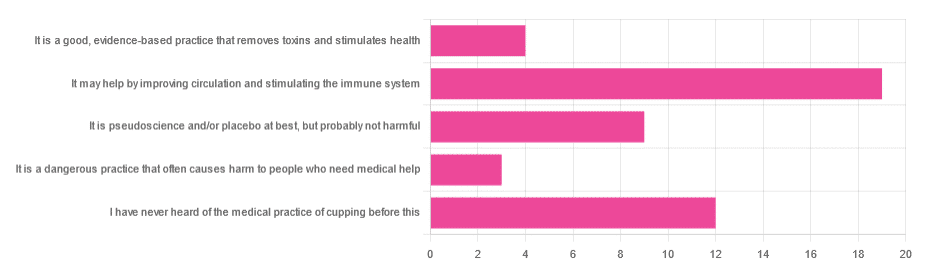
In Tuesday’s newsletter, we asked you for your opinion of cupping (the medical practice), and got the above-depicted, below-described, set of responses:
- About 40% said “It may help by improving circulation and stimulating the immune system”
- About 26% said “I have never heard of the medical practice of cupping before this”
- About 19% said “It is pseudoscience and/or placebo at best, but probably not harmful
- About 9% said “It is a good, evidence-based practice that removes toxins and stimulates health”
- About 6% said “It is a dangerous practice that often causes harm to people who need medical help”
So what does the science say?
First, a quick note for those unfamiliar with cupping: it is the practice of placing a warmed cup on the skin (open side of the cup against the skin). As the warm air inside cools, it reduces the interior air pressure, which means the cup is now (quite literally) a suction cup. This pulls the skin up into the cup a little. The end result is visually, and physiologically, the same process as what happens if someone places the nozzle of a vacuum cleaner against their skin. For that matter, there are alternative versions that simply use a pump-based suction system, instead of heated cups—but the heated cups are most traditional and seem to be most popular. See also:
National Center for Complementary and Integrative Health | Cupping
It is a dangerous practice that often causes harm to people who need medical help: True or False?
False, for any practical purposes.
- Directly, it can (and usually does) cause minor superficial harm, much like many medical treatments, wherein the benefits are considered to outweigh the harm, justifying the treatment. In the case of cupping, the minor harm is usually a little bruising, but there are other risks; see the link we gave just above.
- Indirectly, it could cause harm by emboldening a person to neglect a more impactful treatment for their ailment.
But, there’s nothing for cupping akin to the “the most common cause of death is when someone gets a vertebral artery fatally severed” of chiropractic, for example.
It is a good, evidence-based practice that removes toxins and stimulates health: True or False?
True and False in different parts. This one’s on us; we included four claims in one short line. But let’s look at them individually:
- Is it good? Well, those who like it, like it. It legitimately has some mild health benefits, and its potential for harm is quite small. We’d call this a modest good, but good nonetheless.
- Is it evidence-based? Somewhat, albeit weakly; there are some papers supporting its modest health claims, although the research is mostly only published in journals of alternative medicine, and any we found were in journals that have been described by scientists as pseudoscientific.
- Does it remove toxins? Not directly, at least. There is also a version that involves making a small hole in the skin before applying the cup, the better to draw out the toxins (called “wet cupping”). This might seem a little medieval, but this is because it is from early medieval times (wet cupping’s first recorded use being in the early 7th century). However, the body’s response to being poked, pierced, sucked, etc is to produce antibodies, and they will do their best to remove toxins. So, indirectly, there’s an argument.
- Does it stimulate health? Yes! We’ll come to that shortly. But first…
It is pseudoscience and/or placebo at best, but probably not harmful: True or False?
True in that its traditionally-proposed mechanism of action is a pseudoscience and placebo almost certainly plays a strong part, and also in that it’s generally not harmful.
On it being a pseudoscience: we’ve talked about this before, but it bears repeating; just because something’s proposed mechanism of action is pseudoscience, doesn’t necessarily mean it doesn’t work by some other mechanism of action. If you tell a small child that “eating the rainbow” will improve their health, and they believe this is some sort of magical rainbow power imbuing them with health, then the mechanism of action that they believe in is a pseudoscience, but eating a variety of colorful fruit and vegetables will still be healthy.
In the case of cupping, its proposed mechanism of action has to do withbalancing qi, yin and yang, etc (for which scientific evidence does not exist), in combination with acupuncture lore (for which some limited weak scientific evidence exists). On balancing qi, yin and yang etc, this is a lot like Europe’s historically popular humorism, which was based on the idea of balancing the four humors (blood, yellow bile, black bile, phlegm). Needless to say, humorism was not only a pseudoscience, but also eventually actively disproved with the advent of germ theory and modern medicine. Cupping therapy is not more scientifically based than humorism.
On the placebo side of things, there probably is a little more to it than that; much like with acupuncture, a lot of it may be a combination of placebo and using counter-irritation, a nerve-tricking method to use pain to reduce pain (much like pressing with one’s nail next to an insect bite).
Here’s one of the few studies we found that’s in what looks, at a glance, to be a reputable journal:
Cupping therapy and chronic back pain: systematic review and meta-analysis
It may help by improving circulation and stimulating the immune system: True or False?
True! It will improve local circulation by forcing blood into the area, and stimulate the immune system by giving it a perceived threat to fight.
Again, this can be achieved by many other means; acupuncture (or just “dry needling”, which is similar but without the traditional lore), a cold shower, and/or exercise (and for that matter, sex—which combines exercise, physiological arousal, and usually also foreign bodies to respond to) are all options that can improve circulation and stimulate the immune system.
You can read more about using some of these sorts of tricks for improving health in very well-evidenced, robustly scientific ways here:
The Stress Prescription (Against Aging!)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Egg Noodles vs Soba Noodles – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing egg noodles to soba noodles, we picked the soba.
Why?
First of all, for any unfamiliar, soba noodles are made with buckwheat. Buckwheat, for any unfamiliar, is not wheat and does not contain gluten; it’s just the name of a flowering plant that gets used as though a grain, even though it’s technically not.
In terms of macros, egg noodles have slightly more protein 2x the fat (of which, some cholesterol) while soba noodles have very slightly more carbs and 3x the fiber (and, being plant-based, no cholesterol). Given that the carbs are almost equal, it’s a case of which do we care about more: slightly more protein, or 3x the fiber? We’re going with 3x the fiber, and so are calling this category a win for soba.
In the category of vitamins, egg noodles have more of vitamins A, B12, C, D, E, K, and choline, while soba noodles have more of vitamins B1, B2, B3, B5, B6, and B9. That’s a 6:6 tie. One could argue that egg noodles’ vitamins are the ones more likely to be a deficiency in people, but on the other hand, soba noodles’ vitamins have the greater margins of difference. So, still a tie.
When it comes to minerals, egg noodles have more calcium and selenium, while soba noodles have more copper, iron, magnesium, manganese, phosphorus, potassium, and zinc. So, this one’s not close; it’s an easy win for soba noodles.
Adding up the sections makes for a clear win for soba noodles, but by all means, enjoy moderate portions of either or both (unless you are vegan or allergic to eggs, in which case, skip the egg noodles and just enjoy the soba!).
Want to learn more?
You might like to read:
Egg Noodles vs Rice Noodles – Which is Healthier?
Take care!
Share This Post
-

Natural Remedies and Foods for Osteoarthritis
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝Natural solutions for osteoarthritis. Eg. Rosehip tea, dandelion root tea. Any others??? What foods should I absolutely leave alone?❞
We’ll do a main feature on arthritis (in both its main forms) someday soon, but meanwhile, we recommend eating for good bone/joint health and against inflammation. To that end, you might like these main features we did on those topics:
- We Are Such Stuff As Fish Are Made Of (collagen for bone and joint health)
- The Bare-Bones Truth About Osteoporosis (eating for bone health generally)
- Keep Inflammation At Bay (dietary tips for minimizing inflammation—also, our all-time most popular article to date!)
Of these, probably the last one is the most critical, and also will have the speediest effects if implemented.
Share This Post
-
Dentists Debunk 15 Teeth Myths
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dentists Dr. John Yoo and Dr. Jason Lin leave no gaps in the truth:
The tooth, the whole tooth, and nothing but the tooth
Not only is there no tooth fairy (we are shocked), but also…
- “Baby teeth aren’t important.”
False! Baby teeth act as space holders for permanent teeth, affect speech development, and influence a child’s psychological well-being. - “Acidic fruits will whiten your smile.”
False! In any practical sense, anyway: acidic fruits may temporarily make teeth appear whiter by dispersing stains but cause enamel erosion and weaken teeth over time. - “Fillings last forever.”
False! Fillings can wear down, fail, or develop cavities underneath if oral hygiene isn’t maintained, requiring replacement over time. - “Cavities are irreversible.”
False! Cavities in the enamel can be reversed with fluoride and good oral hygiene, but cavities that reach the dentin are typically irreversible. - “Braces are just for crooked teeth.”
False! Braces also correct functional issues like overbites, underbites, crossbites, and prevent future complications like tooth impaction. - “A knocked-out tooth is gone for good.”
False! A knocked-out tooth can be reimplanted if done quickly (ideally within an hour); storing it in whole milk or saliva helps preserve it. - “Diet sodas won’t give you cavities.”
False! Diet sodas can still cause cavities due to their acidic pH, which erodes enamel, even without sugar. - “Dental cleanings aren’t necessary.”
False! Dental cleanings help remove plaque and tartar that regular brushing can’t, and allow for regular oral health checkups. - “Retainers aren’t for life.”
False! To maintain teeth alignment after braces, retainers should be worn long-term as teeth can shift even years later. - “You should floss before brushing.”
False! The order doesn’t matter, but do floss regularly. - “Everyone has wisdom teeth.”
False! Not everyone is born with wisdom teeth; they are the most commonly missing teeth, and not everyone needs them removed. - “Hydrogen peroxide and baking soda are good toothpaste replacements.”
False! While they are common components in toothpaste, they lack fluoride, which is essential for remineralizing and protecting enamel. - “You’re too old to get braces.”
False! There’s no age limit for braces or aligners; adults often seek them for both aesthetic and functional reasons. - “Teeth that have had root canals can’t feel.”
False! Teeth with root canals can’t feel pain from nerves, but you can still sense pressure due to surrounding ligaments. - “You’ll inevitably lose all your teeth when you’re old.”
False! Good oral hygiene and regular dental care can preserve natural teeth into old age, though genetics also play a role.
For more on each of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Take care!
Share This Post
- “Baby teeth aren’t important.”
Related Posts
-
Who Initiates Sex & Why It Matters
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In an ideal world, it wouldn’t matter any more than who first says “let’s get something to eat” when hungry. But in reality, it can cause serious problems on both sides:
Fear and loathing?
The person who initiates gets the special prize of an n% chance of experiencing rejection, and then what? Try again, and again, and risk seeming pushy? Or leave the ball in the other person’s court, where it may then go untouched for the next few months, because (in the most positive scenario) they were waiting for you to initiate at a better time for them?
The person who does not initiate, and/but does not want sex at that time, gets the special prize of either making their partner feel unwanted, insecure, and perhaps unloved, or else grudgingly consenting to sex that’s going to be no fun while your heart’s not in it, and thus create the same end result plus you had an extra bad experience?
So, that sucks all around:
- Initiating touch (sex or cuddling) can feel like a test of being wanted, whereupon a lack of initiation or response may be misinterpreted as a lack of love or appreciation.
- Meanwhile, non-reciprocation might stem from exhaustion or unrelated issues. For many, it’s a physiological lottery.
10almonds note: not discussed in this video, but for many couples, problems can also arise because one partner or another just isn’t showing up with the expected physical signs of physiological arousal, so even if they say (and mean!) an enthusiastic “yes”, their body’s signs get misread as a “not really, though”, resulting in one partner feeling rejected, and both feeling inadequate—on account of something that was completely unrelated to how the person actually felt about the prospect of sex*.
*Sometimes, physiological arousal will simply not accompany psychological arousal, no matter how sincere the latter. And on the flipside, sometimes the signs of physiological arousal will just show up without psychological arousal. The human body is just like that sometimes. We all must listen to our partners’ words, not their genitals!
The solution to this problem is thus the same as the solution to the rest of the problem that is discussed in the video, and it’s: good communication.
That can be easier said than done, of course—not everyone is at their most eloquent in such situations! Which is why it can be important to have those conversations first outside of the bedroom when the stakes are low/non-existent.
Even with the best communication, a more general, overarching non-reciprocity (real or perceived) of sexual desire can cause bitterness, resentment, and can ultimately be relationship-ending if a resolution that’s acceptable to everyone involved is not found.
Ultimately, the work as a couple must begin from within as individuals—addressing self-worth issues to better navigate love and intimacy.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Relationships: When To Stick It Out & When To Call It Quits
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What’s Keeping the US From Allowing Better Sunscreens?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When dermatologist Adewole “Ade” Adamson sees people spritzing sunscreen as if it’s cologne at the pool where he lives in Austin, Texas, he wants to intervene. “My wife says I shouldn’t,” he said, “even though most people rarely use enough sunscreen.”
At issue is not just whether people are using enough sunscreen, but what ingredients are in it.
The Food and Drug Administration’s ability to approve the chemical filters in sunscreens that are sold in countries such as Japan, South Korea, and France is hamstrung by a 1938 U.S. law that has required sunscreens to be tested on animals and classified as drugs, rather than as cosmetics as they are in much of the world. So Americans are not likely to get those better sunscreens — which block the ultraviolet rays that can cause skin cancer and lead to wrinkles — in time for this summer, or even the next.
Sunscreen makers say that requirement is unfair because companies including BASF Corp. and L’Oréal, which make the newer sunscreen chemicals, submitted safety data on sunscreen chemicals to the European Union authorities some 20 years ago.
Steven Goldberg, a retired vice president of BASF, said companies are wary of the FDA process because of the cost and their fear that additional animal testing could ignite a consumer backlash in the European Union, which bans animal testing of cosmetics, including sunscreen. The companies are asking Congress to change the testing requirements before they take steps to enter the U.S. marketplace.
In a rare example of bipartisanship last summer, Sen. Mike Lee (R-Utah) thanked Rep. Alexandria Ocasio-Cortez (D-N.Y.) for urging the FDA to speed up approvals of new, more effective sunscreen ingredients. Now a bipartisan bill is pending in the House that would require the FDA to allow non-animal testing.
“It goes back to sunscreens being classified as over-the-counter drugs,” said Carl D’Ruiz, a senior manager at DSM-Firmenich, a Switzerland-based maker of sunscreen chemicals. “It’s really about giving the U.S. consumer something that the rest of the world has. People aren’t dying from using sunscreen. They’re dying from melanoma.”
Every hour, at least two people die of skin cancer in the United States. Skin cancer is the most common cancer in America, and 6.1 million adults are treated each year for basal cell and squamous cell carcinomas, according to the Centers for Disease Control and Prevention. The nation’s second-most-common cancer, breast cancer, is diagnosed about 300,000 times annually, though it is far more deadly.
Dermatologists Offer Tips on Keeping Skin Safe and Healthy
– Stay in the shade during peak sunlight hours, 10 a.m. to 4 p.m. daylight time.– Wear hats and sunglasses.– Use UV-blocking sun umbrellas and clothing.– Reapply sunscreen every two hours.You can order overseas versions of sunscreens from online pharmacies such as Cocooncenter in France. Keep in mind that the same brands may have different ingredients if sold in U.S. stores. But importing your sunscreen may not be affordable or practical. “The best sunscreen is the one that you will use over and over again,” said Jane Yoo, a New York City dermatologist.
Though skin cancer treatment success rates are excellent, 1 in 5 Americans will develop skin cancer by age 70. The disease costs the health care system $8.9 billion a year, according to CDC researchers. One study found that the annual cost of treating skin cancer in the United States more than doubled from 2002 to 2011, while the average annual cost for all other cancers increased by just 25%. And unlike many other cancers, most forms of skin cancer can largely be prevented — by using sunscreens and taking other precautions.
But a heavy dose of misinformation has permeated the sunscreen debate, and some people question the safety of sunscreens sold in the United States, which they deride as “chemical” sunscreens. These sunscreen opponents prefer “physical” or “mineral” sunscreens, such as zinc oxide, even though all sunscreen ingredients are chemicals.
“It’s an artificial categorization,” said E. Dennis Bashaw, a retired FDA official who ran the agency’s clinical pharmacology division that studies sunscreens.
Still, such concerns were partly fed by the FDA itself after it published a study that said some sunscreen ingredients had been found in trace amounts in human bloodstreams. When the FDA said in 2019, and then again two years later, that older sunscreen ingredients needed to be studied more to see if they were safe, sunscreen opponents saw an opening, said Nadim Shaath, president of Alpha Research & Development, which imports chemicals used in cosmetics.
“That’s why we have extreme groups and people who aren’t well informed thinking that something penetrating the skin is the end of the world,” Shaath said. “Anything you put on your skin or eat is absorbed.”
Adamson, the Austin dermatologist, said some sunscreen ingredients have been used for 30 years without any population-level evidence that they have harmed anyone. “The issue for me isn’t the safety of the sunscreens we have,” he said. “It’s that some of the chemical sunscreens aren’t as broad spectrum as they could be, meaning they do not block UVA as well. This could be alleviated by the FDA allowing new ingredients.”
Ultraviolet radiation falls between X-rays and visible light on the electromagnetic spectrum. Most of the UV rays that people come in contact with are UVA rays that can penetrate the middle layer of the skin and that cause up to 90% of skin aging, along with a smaller amount of UVB rays that are responsible for sunburns.
The sun protection factor, or SPF, rating on American sunscreen bottles denotes only a sunscreen’s ability to block UVB rays. Although American sunscreens labeled “broad spectrum” should, in theory, block UVA light, some studies have shown they fail to meet the European Union’s higher UVA-blocking standards.
“It looks like a number of these newer chemicals have a better safety profile in addition to better UVA protection,” said David Andrews, deputy director of Environmental Working Group, a nonprofit that researches the ingredients in consumer products. “We have asked the FDA to consider allowing market access.”
The FDA defends its review process and its call for tests of the sunscreens sold in American stores as a way to ensure the safety of products that many people use daily, rather than just a few times a year at the beach.
“Many Americans today rely on sunscreens as a key part of their skin cancer prevention strategy, which makes satisfactory evidence of both safety and effectiveness of these products critical for public health,” Cherie Duvall-Jones, an FDA spokesperson, wrote in an email.
D’Ruiz’s company, DSM-Firmenich, is the only one currently seeking to have a new over-the-counter sunscreen ingredient approved in the United States. The company has spent the past 20 years trying to gain approval for bemotrizinol, a process D’Ruiz said has cost $18 million and has advanced fitfully, despite attempts by Congress in 2014 and 2020 to speed along applications for new UV filters.
Bemotrizinol is the bedrock ingredient in nearly all European and Asian sunscreens, including those by the South Korean brand Beauty of Joseon and Bioré, a Japanese brand.
D’Ruiz said bemotrizinol could secure FDA approval by the end of 2025. If it does, he said, bemotrizinol would be the most vetted and safest sunscreen ingredient on the market, outperforming even the safety profiles of zinc oxide and titanium dioxide.
As Congress and the FDA debate, many Americans have taken to importing their own sunscreens from Asia or Europe, despite the risk of fake products.
“The sunscreen issue has gotten people to see that you can be unsafe if you’re too slow,” said Alex Tabarrok, a professor of economics at George Mason University. “The FDA is just incredibly slow. They’ve been looking at this now literally for 40 years. Congress has ordered them to do it, and they still haven’t done it.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
From Painkillers To Hunger-Killers
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Here’s this week’s selection of health news discoveries, the science behind them, what they mean for you, and where you can go from there:
Killing more than pain
It’s well-known that overuse of opioids can lead to many problems, and here’s another one: messing with the endocrine system. This time, mostly well-evidenced in men—however, the researchers are keen to point out that absence of evidence is very much not evidence of absence, hence “the hidden effects” in the headline below. It’s not that the effects are hard to see—it’s that a lot of the research has yet to be done. For now, though, we know at the very least that there’s an association between opioid use and hyperprolactinemia in men. The same research also begins to shine a light on the effects of opioid use on the hypothalamic-pituitary system and bone health, too:
Read in full: The hidden effects of opioid use on the endocrine system
Related: The 7 Approaches To Pain Management
Gut microbiome dysbiosis may lead to slipping disks
These things sound quite unconnected, but the association is strong. The likely mechanism of action is that the gut dysbiosis influences systemic inflammation, and thus spinal health—because the gut-spine axis cannot really be disconnected (while you’re alive, at least). It’s especially likely if you’re over 50 and female:
Read in full: Are back problems influenced by your gut?
Related: Is Your Gut Leading You Into Osteoporosis?
The Internet is really really great (for brains)
It’s common to see many articles on the Internet telling us, paradoxically, that we should spend less time on the Internet. However… Remember when in the 90s, it was all about “the information superhighway”? It turns out, the fact that it’s more like “the information spaghetti junction” these days doesn’t change the fact that stimulation is good for our brains, and daily Internet use improves memory, because of the different way that we index and store information that came from a virtual source. While there are parts of your brain for “things at home” and “things at the local supermarket”, there are also parts for “things at 10almonds” and “things at Facebook” and so forth. You are, in effect, building a vast mental library as you surf:
Read in full: Daily internet use supercharges your memory!
Related: Make Social Media Work For Your Mental Health
Fall back
Around this time of year in many places in the Northern Hemisphere, the clocks go back an hour (it’s next weekend in the US and Canada, by the way, and this weekend in most of Europe). Many enjoy this as the potential for an extra hour’s sleep, but for night owls, it can be more of a nuisance than a benefit—throwing out what’s often an already difficult relationship with the clock, and presenting challenges both practical and physiological (different processing of melatonin, for instance). Here be science:
Read in full: Why night owls struggle more when the clocks go back
Related: Early Bird Or Night Owl? Genes vs Environment
Can you outrun your hunger?
It seems so, though benefits are strongest in women. We say “outrun”, though this study did use stationary cycling. To put it in few words, intense exercise (but not moderate exercise) significantly reduced acylated ghrelin (hunger hormone) levels, and subjective reports of hunger, especially in women:
Read in full: Study finds intense exercise may suppress appetite in healthy humans
Related: 3 Appetite Suppressants Better Than Ozempic
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: