Can An Alkaline Diet Help You?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small 😎
❝What is the science on eating alkaline foods and minimizing acid foods, does it help against diabetes and/or osteoporosis?❞
The short answer: no
The fuller answer: there are a number of acidic foods that can increase some disease risks—red meat scores highly for many diseases, for example:
- Processed Meat Consumption and the Risk of Cancer: A Critical Evaluation of the Constraints of Current Evidence from Epidemiological Studies
- Red Meat Consumption (Heme Iron Intake) and Risk for Diabetes and Comorbidities?
- Health Risks Associated with Meat Consumption: A Review of Epidemiological Studies
- Associations of Processed Meat, Unprocessed Red Meat, Poultry, or Fish Intake With Incident Cardiovascular Disease and All-Cause Mortality
- Meat consumption: Which are the current global risks? A review of recent (2010-2020) evidences
However, the issue here is the red meat (or processed meat, or worst of all, processed red meat), not the acidity.
Other quadruped-derived meats (especially from pigs) don’t fare much better in terms of metabolic health risks, but fish is generally considered healthful in moderation, and the jury is out on poultry, but it seems to be health-neutral. For more detail, see: Do We Need Animal Products To Be Healthy?
But there are other quite acidic foods that are, for most people, at least very healthful. For example: An Apple (Cider Vinegar) A Day…
…which actually has an antidiabetic (or at least: hypoglycemic, i.e. blood sugar-lowering) effect!
And, less acidic but still notably so: Do Tomatoes & Other Nightshades Cause Inflammation & Worsen Arthritis? ← Betteridge’s Law of Headlines strikes again; the answer is “no”.
And in fact, once again, it really does the opposite: Lycopene’s Benefits For The Gut, Heart, Brain, & More ← tomatoes are generally considered anti-inflammatory (not something their fellow nightshades, potatoes, can boast) due to their lycopene content and polyphenols.
So what’s the deal with the alkaline diet?
The British Dietetic Association explained it well in a nutshell:
❝What is it? Supporters of this diet believe that changing the foods they eat, consuming more alkaline and less acidic foods, will help change the pH balance of the blood and reduce health risks. Worryingly some wrongly claim it can treat cancer and that incorrectly ‘acidic’ foods cause osteoporosis.
Our Verdict: Unfortunately, this diet is based on a basic misunderstanding of human physiology. While encouraging people to eat more fresh veggies is a good thing, the pH of your food will not have an impact on the pH of your blood – and you wouldn’t want it to! Your body is perfectly capable of keeping its blood within a very specific pH range (between 7.35 and 7.45). If it fails to do so you would become very ill very quickly and die if not treated! Diet can change the pH value of urine, but testing the pH of your urine just measures the pH of your urine and is not related to the pH of your blood, which cannot be affected by diet.
Bottom Line: It’s alka-lie! You’ll most likely lose weight as you are cutting out processed foods and eating more healthily – nothing to do with acid or alkali nonsense.❞
Read more: British Dietetic Association | Top 5 worst celeb diets to avoid
About the idea of it treating cancer, let’s look to the American Institute for Cancer Research:
❝The alkaline diet cannot change body pH. While it promotes healthy foods like fruits and vegetables, the body tightly regulates blood pH, and diet cannot alter it.
There is no evidence that an alkaline diet can prevent or cure cancer. The tumor environment’s acidity is a result of cancer metabolism, not a cause of it.
A balanced plant-focused diet is best, especially if it’s not too restrictive. Following evidence-based recommendations such as AICR’s New American Plate is a smart approach for overall health and cancer prevention.❞
Read more: American Institute for Cancer Research: Does the Alkaline Diet Cure Cancer?
As for osteoporosis, once again, there’s a clear answer:
❝A causal association between dietary acid load and osteoporotic bone disease is not supported by evidence and there is no evidence that an alkaline diet is protective of bone health.❞
Read more: Causal assessment of dietary acid load and bone disease: a systematic review & meta-analysis
In short: it was an interesting idea, but the science said “no” in every respect.
There are some exceptions
For some people, there can be a health-related reason to avoid acidic foods.
For example:
- Foods For & Against Hiatus Hernia (acidic foods can worsen such)
- Acid Reflux After Meals? Here’s How To Stop It Naturally (shocking nobody, reducing the acids one puts into one’s stomach can help reduce acid reflux).
But, those are things to bear in mind if you are facing those specific health problems, not something to do prophylactically.
Your stomach acid is supposed to be acidic, after all.
It wouldn’t work otherwise!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What Happens When You Break A Bone?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Drs. Gurpreet Baht and Natalie Pang give us the insider info:
To the bone
About half of all people will break at least one bone during their lifetime, and the body’s 200+* bones come in several categories including short bones, long bones, flat bones, and irregular bones.
*You may have heard different numbers. Popular numbers in the public consciousness include 215 (thanks to a famous line in the movie Terminator II: Judgment Day), and 206 which is a very popular reckoning with rather sounder reasoning, but 200 is the baseline unless you’re missing some. The reason for the variation is that humans start with 270–300 bones, but many of these fuse together in infancy (for example, much of the skull and coccyx, most of which fusing is done around ages 1–2 years), resulting in a smaller total number. Another reason for variation in total number is that some people have some extra bones, which is usually a case of a harmless copying error.
Of these, long bones tend to fracture more frequently because they usually absorb the main force of impacts such as falls. However, in the case of somebody more frail than average (so, a lot of older people, for example), hips become quite common candidates, because upon falling: a) they’re often not falling from a great height than their own, so they didn’t break a leg b) they weren’t quick enough to put an arm out to try to break their fall, which means, if falling sideways, which there’s a 50% chance of being the case, the hip hits the floor full-force.
Some quick notes on the physiology going on here:
- On why it hurts quite so much: bones contain blood vessels and nerves that transmit intense pain signals during fractures, though scientists still don’t fully understand why broken bones hurt so much because these nerves are encased in hard tissue and difficult to study.
- On how healing gets going: when a bone breaks the internal blood vessels rupture, causing bleeding and inflammation that begin the healing process.
That process is a several-stage affair:
- Inflammatory phase: during roughly the first week immune cells clear damaged tissue and release signalling molecules that recruit stem cells to the injury site.
- Cartilage callus formation: recruited stem cells become chondrocytes that use the blood clot at the fracture site as a scaffold to quickly build a temporary cartilage callus.
- Bony callus formation and remodeling: some chondrocytes and stem cells become osteoblasts that create a stronger bony callus, after which specialized cells gradually reshape the bone over several months while osteoblasts lay down new bone tissue.
- Treatment and healing variability: healing time depends on factors such as diet, rest, and fracture severity, with clean breaks often treated using casts or splints while severe or displaced fractures may require surgery with pins, plates, or screws.
- Misaligned healing and final outcome: if a bone heals incorrectly surgeons may need to refracture and realign it, and although a small bump may remain temporarily after healing the bone typically becomes as strong as it was before.
For more on all of this, plus some visual illustrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
5 Hip Exercises To Strengthen Bones & Improve Balance (Osteoporosis-Friendly)
Take care!
Share This Post
-
What Does Hypermobile Posture Look Like?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Is this how you stand and/or walk?
Every which way and loose
Posture, with hypermobility, can be quite paradoxical—for example, it can be either overly stiff for protection, or overly loose with poor control, often alternating between bracing and collapsing.
Some things to watch out for:
- Standing posture: favoring one leg over both, locking your knees backwards or keeping a slight constant bend, your pelvis tucked under and/or shifted forwards.
- Walking pattern: feet turned out, glute clenching, and/or excessive leg rotation where your leg rolls in then your knee swings out as weight transfers.
- Joint behaviour: frequent hyperextension, especially in your knees, elbows, fingers, or spine, plus excessive fidgeting or moving into end-range positions even while standing still.
- Upper body signs: exaggerated hand gestures, frequent neck movement, shoulder tension, and a tendency to overextend your neck or back beyond neutral.
Confession: your writer here is currently writing this while standing on one leg, hip cocked, as she types with her very spidery fingers, and proofreading with a tilted head like a dog that thinks things might make more sense at 45°. This video is taking no prisoners today, it seems.
In the video, we also learn about unusual flexibility positions like curling our toes, sitting in extreme folded postures, “W-sitting,” or “frog-leg” positions that feel natural but may stress our joints.
Notably, the main visual clue isn’t just flexibility, but rather also instability, where our body uses compensations like muscle gripping, locking joints, or shifting alignment to create support.
For once, there’s no real call-to-action here; we cannot re-posture our way out of having hypermobility. If our body’s built this way, it’s built this way, and that’s that (per current science anyway; who knows what future developments may be discovered).
However, it can be good to recognize the signs and symptoms, such that we can better understand what’s going on.
For more on all of this plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
What Your Hands Can Tell You About Your Health ← about some hypermobility signs that can show up in our hands
Take care!
Share This Post
-
What’s the difference between food poisoning and gastro? A gut expert explains
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
If you’ve got a dodgy tummy, diarrhoea and have been vomiting, it’s easy to blame a “tummy bug” or “off food”.
But which is it? Gastro or food poisoning?
What’s the difference anyway?

Andrey_Popov/Shutterstock What’s gastroenteritis?
Gastroenteritis, or gastro for short, is a gut infection caused by a virus, bacterium or other microbe.
The gut is teeming with cells including healthy microbes and the cells lining the gut. But when viruses, bacteria and other microbes start to invade your gut, they colonise, build up in large numbers and eventually cause the cells lining the gut to inflame. The “-itis” at the end of gastroenteritis means inflammation.
Gastroenteritis is extremely common. In Australia there are an estimated 17.2 million cases a year.
So where do these gastro-causing microbes come from? Eating contaminated food is often the source.
However you can acquire these microbes in other ways. For example, if you touch a surface where someone sick from viral gastroenteritis had vomited on, that virus could transfer to your hands. And if your hands touched your mouth, you in turn could contract viral gastroenteritis.
What’s food poisoning?
Food poisoning refers to getting sick from eating food contaminated with chemicals, microbes or toxins.
For example if you ate food contaminated with insecticides or methyl alcohol (methanol) that would count as food poisoning. If you ate puffer fish or poisonous mushrooms that would count too. But food poisoning doesn’t include the effects of eating a food you’re allergic to.
The vast majority of food poisonings are as a result of food contaminated by microbes and their toxins. When you eat or drink them it’s like a missile strike. The toxins in particular can rapidly cause inflammation and damage the lining of the gut.
To add to the confusion, food poisoning is often referred to as foodborne gastroenteritis.
Food poisoning (or foodborne gastroenteritis) is also common in Australia. It accounts for about one-third of all cases of gastroenteritis or an estimated 5.4 million cases every year.
How can we tell the two apart?
Both gastroenteritis and food poisoning have symptoms such as diarrhoea, vomiting, nausea, abdominal cramps, fever and headaches. But these symptoms can come on in different ways.
Viral gastroenteritis, such as with norovirus, usually causes symptoms 24–48 hours after exposure, which can last for one to two days.
But food poisoning after eating microbial toxins can come on very quickly. For example, toxins from the bacterium Staphylococcus aureus can cause symptoms within 30 minutes of eating contaminated food, such as undercooked meat. Fortunately, symptoms usually get better within 24 hours.
Symptoms don’t always come on so quickly in all cases of bacterial food poisoning. For example, it can take as long as 70 days between exposure to Listeria and symptoms occurring, although, on average it’s about three weeks. This long incubation period can make it difficult to work out if a particular food is responsible for someone getting sick.
As a general guide food poisoning occurs quite quickly (within hours of eating contaminated food) while gastroenteritis can take a day or more after eating to get sick. But there is no hard and fast rule.
It can take weeks from eating soft cheese contaminated with Listeria before you have symptoms. In Green/Shutterstock How do I prevent them?
The same precautions when handling food apply to preventing both gastroenteritis and food poisoning. These steps not only lower your risk of being affected in the first place, they lower your risk of you infecting others.
Wash your hands thoroughly with soap and water before preparing food. Use separate cutting boards and utensils for raw and cooked foods to help avoid cross-contamination. Cook food thoroughly and store it at safe temperatures.
Gastroenteritis can involve transmission of microbes through means other than food, for instance, via poo on your hands if you don’t wash your hands after using the toilet or after changing a child’s nappy. So wash your hands afterwards.
To prevent others from becoming sick, make sure you quickly disinfect contaminated surfaces thoroughly after someone vomits or has diarrhoea. First, put on gloves and wash surfaces with hot water and a detergent. Then disinfect using household bleach containing 0.1% hypochlorite.
How can I get better?
Treating both gastroenteritis and food poisoning focuses on preventing dehydration and relieving symptoms.
To avoid dehydration, drink plenty of fluids. For moderate or severe cases, you can buy commercial oral rehydration solution from a pharmacy.
You can also make your own oral rehydration solution by adding 6 teaspoons of sugar, ½ teaspoon of salt and ½ teaspoon of sodium bicarbonate to a litre of water. You can splash in some cordial for taste.
If symptoms are severe or persist you should see your GP or go to the emergency department.
Vincent Ho, Associate Professor and Clinical Academic Gastroenterologist, Western Sydney University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post





Related Posts
-

The Body Is Not an Apology – by Sonya Renee Taylor
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First, a couple of things that this book is not about:
- Self-confidence (it’s about more than merely thinking highly of oneself)
- Self-acceptance (it’s about more than merely settling for “good enough”)
In contrast, it’s about loving and celebrating what is, while striving for better, for oneself and for others.
You may be wondering: whence this “radical” in the title?
The author argues that often, the problem with our bodies is not actually our bodies. If we have cancer, or diabetes, then sure, that’s a problem with the body. But most of the time, the “problem with our bodies” is simply society’s rejection of our “imperfect” bodies as somehow “less than”, and something we must invest time and money to correct. Hence, the need for a radical uprooting of ideas, to fix the real problem.
Bottom line: if, like most of us, you have a body that would not entirely pass for that of a Marvel Comics superhero, this is a book for you. And if you do have a MCU body? This is also a book for you, because we have bad news for you about what happens with age.
Click here to check out The Body Is Not An Apology, and appreciate more about yours!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Reverse Inflammation Naturally – by Dr. Michelle Honda
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This book is in some ways not as marketable as some; it doesn’t have lots of colorful healthy food on the cover; it doesn’t even have a “woman laughing alone with salad” (you know the stock photo trope), let alone someone looking glamorous in a labcoat with a stethoscope draped over their shoulder despite listening to hearts not being a regular part of their job as an immunologist or such.
What it does have, instead, is a lot of very useful information, and much more than you’ll usually find in a book for laypeople.
For example, you probably know that for fighting inflammation, a green salad is better than a cheeseburger, say, and a black coffee is better than a glass of wine.
But do you know about the roles, for good or ill, of prostaglandins and linoleic fats vs dietary fats? How about delta-6-desaturase? Neu5Gc and arachidonic acid?
Dr. Honda demystifies all of these and more, as well as talking about the impacts of very many foods and related habits on various different inflammation-based disease. And of course, almost all disease involves some kind of inflammation (making fighting inflammation one of the best things you can do for your overall disease-avoidance strategy!), but she singles out some of the most relevant, as per the list on the front cover.
She also talks a lot of “pharmacy in your kitchen”, in other words, what herbs, spices, and plant extracts we can enjoy for (evidence-based!) benefits on top of our default healthy diet free (or at least mostly free, for surely none of us are perfect) from inflammatory agents.
Not content with merely giving a huge amount of information, she also gives recipes and a meal plan, but honestly, it’s the informational chapters that are the real value of the book.
Bottom line: if you’d like to reduce your body’s inflammation levels (and/or perhaps those of a loved one for whom you cook), then this book will be an invaluable resource.
Click here to check out Reverse Inflammation Naturally, and reverse inflammation naturally!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Half of Australians in aged care have depression. Psychological therapy could help
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
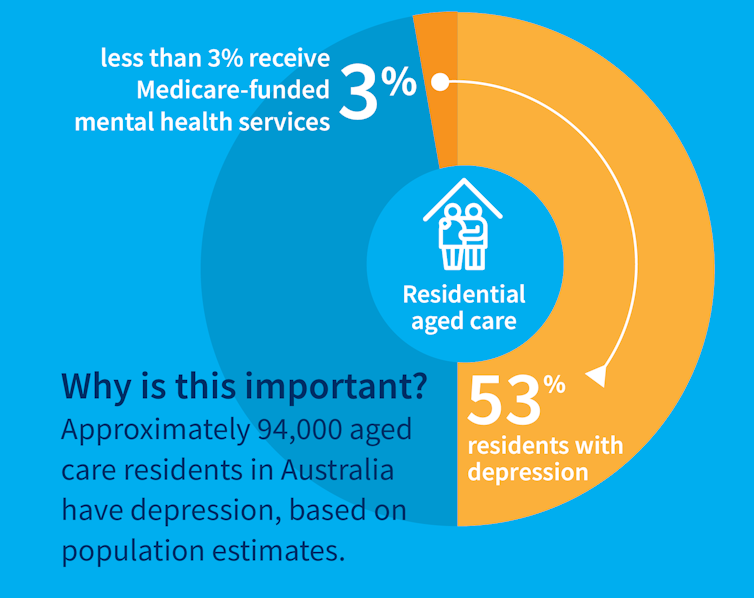
While many people maintain positive emotional wellbeing as they age, around half of older Australians living in residential aged care have significant levels of depression. Symptoms such as low mood, lack of interest or pleasure in life and difficulty sleeping are common.
Rates of depression in aged care appear to be increasing, and without adequate treatment, symptoms can be enduring and significantly impair older adults’ quality of life.
But only a minority of aged care residents with depression receive services specific to the condition. Less than 3% of Australian aged care residents access Medicare-subsidised mental health services, such as consultations with a psychologist or psychiatrist, each year.
Cochrane AustraliaInstead, residents are typically prescribed a medication by their GP to manage their mental health, which they often take for several months or years. A recent study found six in ten Australian aged care residents take antidepressants.
While antidepressant medications may help many people, we lack robust evidence on whether they work for aged care residents with depression. Researchers have described “serious limitations of the current standard of care” in reference to the widespread use of antidepressants to treat frail older people with depression.
Given this, we wanted to find out whether psychological therapies can help manage depression in this group. These treatments address factors contributing to people’s distress and provide them with skills to manage their symptoms and improve their day-to-day lives. But to date researchers, care providers and policy makers haven’t had clear information about their effectiveness for treating depression among older people in residential aged care.
The good news is the evidence we published today suggests psychological therapies may be an effective approach for people living in aged care.
We reviewed the evidence
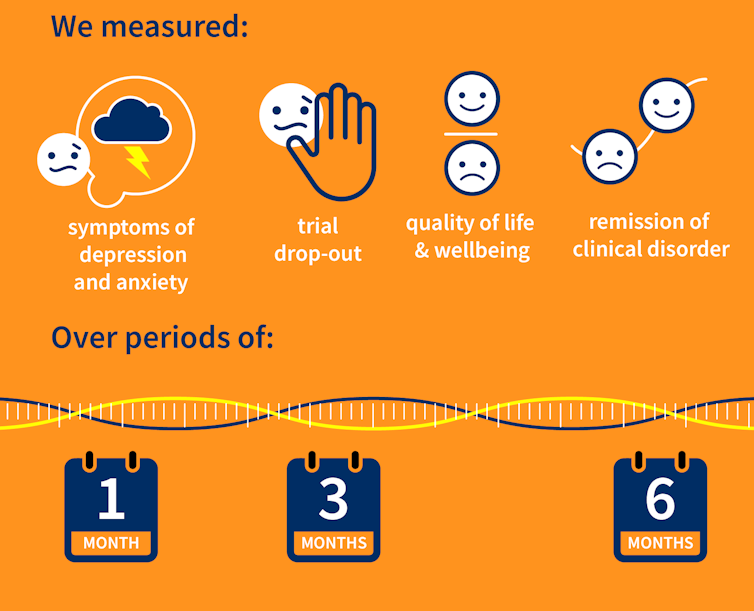
Our research team searched for randomised controlled trials published over the past 40 years that were designed to test the effectiveness of psychological therapies for depression among aged care residents 65 and over. We identified 19 trials from seven countries, including Australia, involving a total of 873 aged care residents with significant symptoms of depression.
The studies tested several different kinds of psychological therapies, which we classified as cognitive behavioural therapy (CBT), behaviour therapy or reminiscence therapy.
CBT involves teaching practical skills to help people re-frame negative thoughts and beliefs, while behaviour therapy aims to modify behaviour patterns by encouraging people with depression to engage in pleasurable and rewarding activities. Reminiscence therapy supports older people to reflect on positive or shared memories, and helps them find meaning in their life history.
The therapies were delivered by a range of professionals, including psychologists, social workers, occupational therapists and trainee therapists.
Cochrane AustraliaIn these studies, psychological therapies were compared to a control group where the older people did not receive psychological therapy. In most studies, this was “usual care” – the care typically provided to aged care residents, which may include access to antidepressants, scheduled activities and help with day-to-day tasks.
In some studies psychological therapy was compared to a situation where the older people received extra social contact, such as visits from a volunteer or joining in a discussion group.
What we found
Our results showed psychological therapies may be effective in reducing symptoms of depression for older people in residential aged care, compared with usual care, with effects lasting up to six months. While we didn’t see the same effect beyond six months, only two of the studies in our review followed people for this length of time, so the data was limited.
Our findings suggest these therapies may also improve quality of life and psychological wellbeing.
Psychological therapies mostly included between two and ten sessions, so the interventions were relatively brief. This is positive in terms of the potential feasibility of delivering psychological therapies at scale. The three different therapy types all appeared to be effective, compared to usual care.
However, we found psychological therapy may not be more effective than extra social contact in reducing symptoms of depression. Older people commonly feel bored, lonely and socially isolated in aged care. The activities on offer are often inadequate to meet their needs for stimulation and interest. So identifying ways to increase meaningful engagement day-to-day could improve the mental health and wellbeing of older people in aged care.
Some limitations
Many of the studies we found were of relatively poor quality, because of small sample sizes and potential risk of bias, for example. So we need more high-quality research to increase our confidence in the findings.
Many of the studies we reviewed were also old, and important gaps remain. For example, we are yet to understand the effectiveness of psychological therapies for people from diverse cultural or linguistic backgrounds.
Separately, we need better research to evaluate the effectiveness of antidepressants among aged care residents.
What needs to happen now?
Depression should not be considered a “normal” experience at this (or any other) stage of life, and those experiencing symptoms should have equal access to a range of effective treatments. The royal commission into aged care highlighted that Australians living in aged care don’t receive enough mental health support and called for this issue to be addressed.
While there have been some efforts to provide psychological services in residential aged care, the unmet need remains very high, and much more must be done.
The focus now needs to shift to how to implement psychological therapies in aged care, by increasing the competencies of the aged care workforce, training the next generation of psychologists to work in this setting, and funding these programs in a cost-effective way.

Tanya Davison, Adjunct professor, Health & Ageing Research Group, Swinburne University of Technology and Sunil Bhar, Professor of Clinical Psychology, Swinburne University of Technology
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: