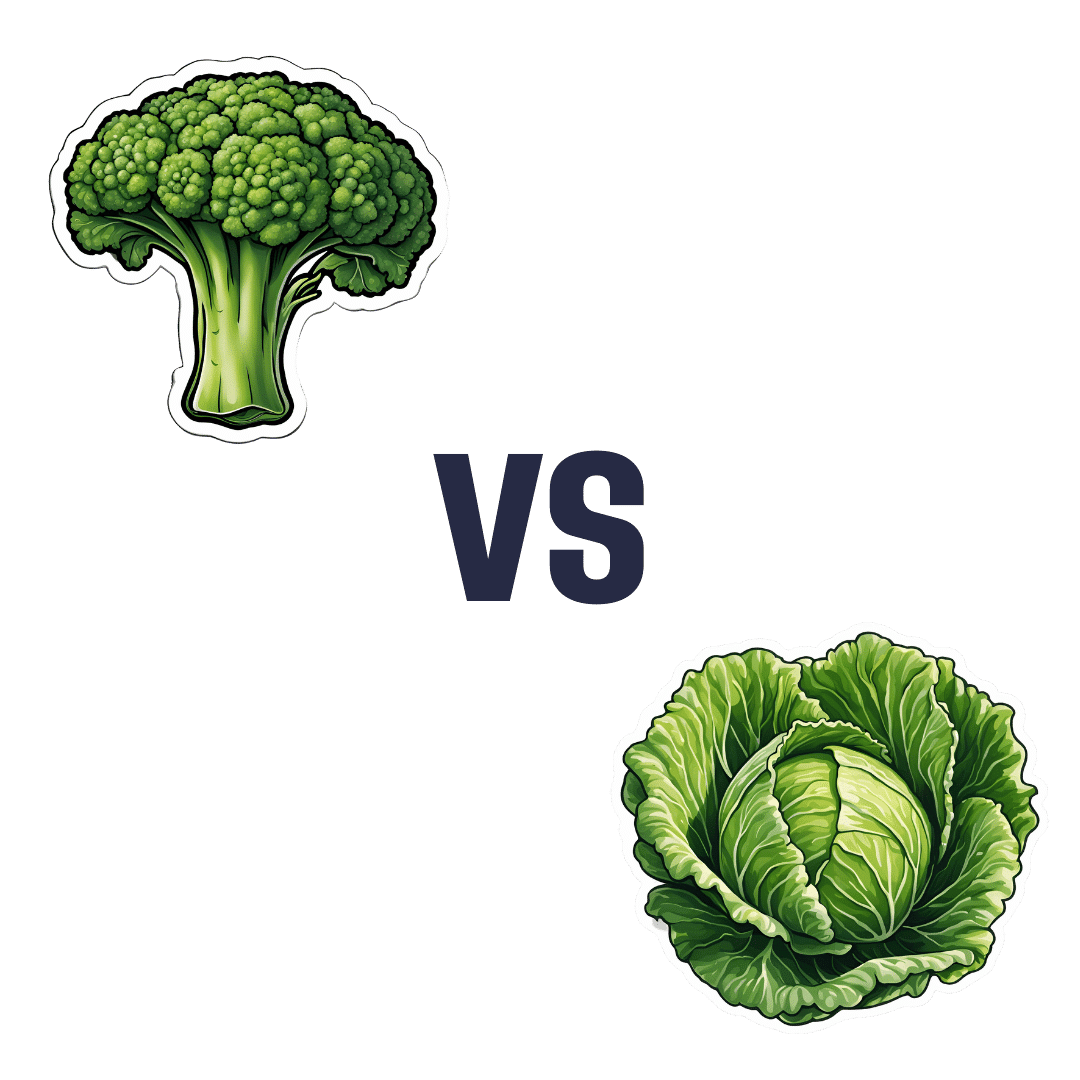
Broccoli vs Cabbage – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing broccoli to cabbage, we picked the broccoli.
Why?
Here we go once again pitting two different cultivars of the same species (Brassica oleracea) against each other, and/but once again, there is one that comes out as nutritionally best.
In terms of macros, broccoli has more protein, carbs, and fiber, while they are both low glycemic index foods. The differences are small though, so it’s fairest to call this category a tie.
When it comes to vitamins, broccoli has more of vitamins A, B1, B2, B3, B5, B6, B7, B9, C, E, K, and choline, while cabbage is not higher in any vitamins. It should be noted that cabbage is still good for these, especially vitamins C and K, but broccoli is simply better.
In the category of minerals, broccoli has more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc, while cabbage is not higher in any minerals. Again though, cabbage is still good, especially in calcium, iron, and manganese, but again, broccoli is simply better.
Of course, enjoy either or both! But if you want the nutritionally densest option, it’s broccoli.
Want to learn more?
You might like to read:
What’s Your Plant Diversity Score?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Easing Election Stress & Anxiety

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
At the time of writing, the US is about to have a presidential election. Most of our readers are Americans, and in any case, what the US does tends to affect most of the world, so certainly many readers in other countries will be experiencing stress and anxiety about it too.
We’re a health science publication, not a political outlet, so we’ll refrain from commenting on any candidates or campaign policies, and we’d also like to be clear we are not urging you to any particular action politically—our focus today is simply about mental health.
First, CBT what can be CBT’d
Cognitive Behavioral Therapy (CBT) is far from a panacea, but it’s often a very good starting point. And when it seems the stakes are high, it’s easy to fall into such cognitive distortions as “crystal ball” and “catastrophization”, that is to say, predicting the future and feeling the impact of that (probably undesired version of the) future, and also feeling like it will be the end of the world.
Recognizing these processes and how they work, is the first step to managing our feelings about them.
Learn more: The Art of Being Unflappable (Tricks For Daily Life)
Next, DBT what can be DBT’d
A lot of CBT hinges on the assumption that our assumptions are incorrect. For example, that our friend does not secretly despise us, that our spouse is not about to leave us, that the symptoms we are experiencing are not cancer, and in this case, that the election outcome will not go badly, and if it does, the consequences will be less severe than imagined.
But… What if our concerns are, in fact, fully justified? Here’s where Dialectic Behavior Therapy (DBT) comes in, and with it, what therapists call “radical acceptance”.
In other words, we accept up front the idea that maybe it’s going to be terrible and that will truly suck, and then either:
- there’s nothing we can reasonably do about it now (so worrying just means you’ll suffer twice), or
- there is something we can reasonably do about it now (so we can go do that thing)
After doing the thing (if appropriate), defer processing the outcome of the election until after the election. There is no point in wasting energy to worry before then. In a broadly two-party system where things are usually close between those two largest parties, there’s something close to a 50% chance of an outcome that’s, at least, not the worst you feared.
Learn more: CBT, DBT, & Radical Acceptance
Lastly, empower yourself with Behavioral Activation (BA)
Whatever the outcome of any given election, the world will keep turning, and the individual battles about any given law or policy or such will continue to go on. That’s not to say an election won’t change things—it will—but there will always still be stuff to do on a grassroots level to make the world a better place, no matter what politician has been elected.
Being involved in doing things on a community level will not only help banish any feelings of despair (and if you got the election outcome you wanted, it’ll help you feel involved), but also, it can give you a sense of control, and can even form a part of the “ikigai” that is often talked about as one of the pillars of healthy longevity.
Learn more: What’s Your Ikigai?
And if you like videos, then enjoy this one (narrated by the ever soothing-voiced Alain de Botton):
Watch now: How To Escape From A Despairing Mood (4:46) ← it also has a text version if you prefer that
Take care!
Share This Post
-

How To Keep On Keeping On?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How To Keep On Keeping On… Long Term!
For many when it comes to health-related goals and practices, it’s easy to find ourselves in a bit of a motivational dip around this time of year. The enthusiasm of new year’s resolutions has been and gone, and there’s not yet much of a drive to “get a beach body” or “be summer-ready”.
A word to the wise on those before moving on, though:
- How to get a beach body: take your body to a beach. Voilà. Beach body.
- Remember: the beach is there for your pleasure and entertainment, not the other way around!
- How to be summer-ready: the real question is, will summer be ready for you?
But what is this, demotivational rhetoric to discourage you from getting fit and healthy?
Not at all, but rather, to be sure that you’re pursuing your own goals and not just what you feel might be expected of you.
All that in mind, let’s get to the tips…
Focus on adding health
It can be tempting (and even, good) to cut down on unhealthy things. But when it comes to motivation, it’s harder to stay motivated for deprivation, than it is for some healthy addition to life.
So for example, this philosophy would advocate for:
- Instead of counting calories, count steps! Or even…
- Instead of counting calories, count colors! Eat the rainbow and all that. No, skittles do not count, but eating a variety of naturally different-colored foods will tend to result in adding different nutrients to your diet.
- Instead of cutting out sugar, add fruit! How many per day will you go for? If you don’t eat much fruit as it is, consider making it a goal to have even just one piece of fruit a day, then build up from there. Find fruit you like! If you pick the fruit you want instead of the fruit you think you “should” have, it’s basically a dessert snack.
We’ve recommended it before, and we’ll recommend it again, but if you’re interested in “adding health”, you should definitely check out:
Dr. Greger’s Daily Dozen (checklist, plus app if you want it)
More details: it’s a checklist of 12 things you should try to include in your diet, with a free streak-tracking app, if you want it, all based on the same scientific research as the best-selling book “How Not To Die”.
“Minimum effort!”
Did you see the movie “Deadpool”? The protagonist has a catch-phrase as he goes into battle, saying to himself “Maximum effort!”.
And, that’s all very well and good if your superpower is immediate recovery from pretty much anything, but for the rest of us, sometimes it’s good to hold ourselves to “minimum effort!”.
Sometimes, something worth doing is worth doing just a little a bit. It’s always better than nothing! Even if feels like you gained nothing from it, it’s the foundation of a habit, and the habit will grow and add up. Sometimes it may even take you by surprise…
Don’t feel like doing 20 bodyweight squats? Do literally just one. Make a deal with yourself: do just one, then you can stop if you like. Then after you’ve done one, you might think to yourself “huh, that wasn’t so bad”, and you try out a few more. Maybe after 5 you can feel your blood pumping a bit and you think “you know what, that’s enough for now”, and great, you did 5x as much exercise as you planned! Wonder what you’ll do tomorrow!
(personal note from your writer here: I’ve managed to “just extend this exercise a little bit more than last time” my way into hour-long exercise sessions before now; I started with “just 10 squats” or “just one sun salutation” etc, to get myself out of a no-exercise period that I’d slipped into, and it’s amazing how quickly adding just a little bit to the previous day’s “minimum effort!” adds up to a very respectable daily exercise session)
Wondering what a good, easy, respectable short term goal could be?
Check Out, For Example: The Seven-Minute Workout
(You might have heard of this one before; it’s an incredibly efficient well-optimized short complete workout that requires no special equipment, just a bit of floorspace and a wall—the above app allows for customizations of it per your preferences, but the basic routine is an excellent starting point for most people)
Commit to yourself (and do any self-negotiation up-front)
Really commit, though. No “or I will look silly because I told people I’d do it”, no “or I will donate x amount to charity” etc, just “I will do it and that’s that”. If you find yourself second-guessing yourself or renegotiating with yourself, just shut that down immediately and refuse to consider it.
Note: you should have break-clauses in this contract with yourself, though. For example, “unless I am ill or injured” is a sensible rule to have in advance for most exercise regimes that weren’t undertaken with your illness or injury in mind.
Make a “To-Don’t” list
Much like how addicts are often advised to not try to quit more than one thing at once, we must also be mindful of not taking on too much at once. It can be very tempting to think:
“I will turn my life around, now! I’ll quit alcohol and animal products and sugar and refined grains, and I’ll go for a run each morning, and I’ll do this and that and there, I’ve got it, here is the blueprint for my healthy perfect life from this day forth!”
And, it’s great to have any and all of that as your end goal if you want, but please, pick one or two things at most to start with, focus on those, and when those have become second nature to you and just a normal part of your life, then choose the next thing to work on.
(You can plan out the whole thing in advance if you want! i.e., I’ll do this, then this, then this, but just… make sure that you’ve really got each one down to a matter of comfort and ease before you take up the next one)
In summary:
- Focus on adding health, whatever that looks like to you
- Figure out what “minimum effort!” is for you, and let that be your baseline
- Commit to yourself (and do any self-negotiation up-front, not later)
- Decide what you’re not going to do yet, and stick to that, too.
Share This Post
- How to get a beach body: take your body to a beach. Voilà. Beach body.
-

Fitness In Our Fifties
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
Q: What’s a worthwhile fitness goal for people in their 50s?
A: At 10almonds, we think that goals are great but habits are better.
If your goal is to run a marathon, that’s a fine goal, and can be very motivating, but then after the marathon, then what? You’ll look back on it as a great achievement, but what will it do for your future health?
PS, yes, marathon-running in one’s middle age is a fine and good activity for most people. Maybe skip it if you have osteoporosis or some other relevant problem (check with your doctor), but…
Marathons in Mid- and Later-Life ← we wrote about the science of it here
PS, we also explored some science that may be applicable to your other question, on the same page as that about marathons!
The thing about habits vs goals is that habits give ongoing cumulative (often even: compounding) benefits:
How To Really Pick Up (And Keep!) Those Habits
If you pressingly want advice on goals though, our advice is this:
Make it your goal to be prepared for the health challenges of later life. It may seem gloomy to say that old age is coming for us all if something else doesn’t get us first, but the fact is, old age does not have to come with age-related decline, and the very least, we can increase our healthspan (so we’re hitting 90 with most of the good health we enjoyed in our 70s, for example, or hitting 80 with most of the good health we enjoyed in our 60s).
If that goal seems a little wishy-washy, here are some very specific and practical ideas to get you started:
Train For The Event Of Your Life!
As for the limits and/or extents of how much we can do in that regard? Here are what two aging experts have to say:
And here’s what we at 10almonds had to say:
Age & Aging: What Can (And Can’t) We Do About It?
Take care!
Share This Post
Related Posts
-

The Science-Backed Anti-Inflammatory Diet for Beginners – by Dr. Yasmine Elamir & Dr. William Grist
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We have written about how to eat to beat inflammation, but what we didn’t do is include 75 recipes and a plan for building up one’s culinary repertoire around those core dishes!
That’s what this book does. It covers briefly the science of inflammation and anti-inflammatory diet, discusses experimental elimination diets (e.g. you eliminate likely culprits of triggering your inflammation, then reintroduce them one by one to see which it was), and ingredients likely to increase or decrease inflammation.
The 75 recipes are good, and/but a caveat is “yes, one of the recipes is ketchup and another is sour cream” so it’s not exactly 75 mains.
However! Where this book excels is in producing anti-inflammatory versions of commonly inflammatory dishes. That ketchup? Not sugary. The sour cream? Vegan. And so forth. We also see crispy roast potatoes, an array of desserts, and sections for popular holiday dishes too, so you will not need to be suddenly inflamed into the next dimension when it comes to festive eating.
The recipes are what the title claims them to be, “science-backed anti-inflammatory”, and that is clearly the main criterion for their inclusion. They are not by default vegan, vegetarian, dairy-free, nut-free, gluten-free, etc. For this reason, all recipes are marked with such tags as “V, VG, DF, GF, EF, NF” etc as applicable.
Bottom line: we’d consider this book more of a jumping-off point than a complete repertoire, but it’s a very good jumping-off point, and will definitely get you “up and running” (there’s a 21-day meal plan, for example).
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

‘Noisy’ autistic brains seem better at certain tasks. Here’s why neuroaffirmative research matters
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Pratik Raul, University of Canberra; Jeroen van Boxtel, University of Canberra, and Jovana Acevska, University of Canberra
Autism is a neurodevelopmental difference associated with specific experiences and characteristics.
For decades, autism research has focused on behavioural, cognitive, social and communication difficulties. These studies highlighted how autistic people face issues with everyday tasks that allistic (meaning non-autistic) people do not. Some difficulties may include recognising emotions or social cues.
But some research, including our own study, has explored specific advantages in autism. Studies have shown that in some cognitive tasks, autistic people perform better than allistic people. Autistic people may have greater success in identifying a simple shape embedded within a more complex design, arranging blocks of different shapes and colours, or spotting an object within a cluttered visual environment (similar to Where’s Wally?). Such enhanced performance has been recorded in babies as young as nine months who show emerging signs of autism.
How and why do autistic individuals do so well on these tasks? The answer may be surprising: more “neural noise”.
What is neural noise?
Generally, when you think of noise, you probably think of auditory noise, the ups and downs in the amplitude of sound frequencies we hear.
A similar thing happens in the brain with random fluctuations in neural activity. This is called neural noise.
This noise is always present, and comes on top of any brain activity caused by things we see, hear, smell and touch. This means that in the brain, an identical stimulus that is presented multiple times won’t cause exactly the same activity. Sometimes the brain is more active, sometimes less. In fact, even the response to a single stimulus or event will fluctuate continuously.
Neural noise in autism
There are many sources of neural noise in the brain. These include how the neurons become excited and calm again, changes in attention and arousal levels, and biochemical processes at the cellular level, among others. An allistic brain has mechanisms to manage and use this noise. For instance, cells in the hippocampus (the brain’s memory system) can make use of neural noise to enhance memory encoding and recall.
Evidence for high neural noise in autism can be seen in electroencephalography (EEG) recordings, where increased levels of neural fluctuations were observed in autistic children. This means their neural activity is less predictable, showing a wider range of activity (higher ups and downs) in response to the same stimulus.
In simple terms, if we imagine the EEG responses like a sound wave, we would expect to see small ups and downs (amplitude) in allistic brains each time they encounter a stimulus. But autistic brains seem to show bigger ups and downs, demonstrating greater amplitude of neural noise.
Many studies have linked this noisy autistic brain with cognitive, social and behavioural difficulties.
But could noise be a bonus?
The diagnosis of autism has a long clinical history. A shift from the medical to a more social model has also seen advocacy for it to be reframed as a difference, rather than a disorder or deficit. This change has also entered autism research. Neuroaffirming research can examine the uniqueness and strengths of neurodivergence.
Psychology and perception researcher David Simmons and colleagues at the University of Glasgow were the first to suggest that while high neural noise is generally a disadvantage in autism, it can sometimes provide benefits due to a phenomenon called stochastic resonance. This is where optimal amounts of noise can enhance performance. In line with this theory, high neural noise in the autistic brain might enhance performance for some cognitive tasks.
Our 2023 research explores this idea. We recruited participants from the general population and investigated their performance on letter-detection tasks. At the same time, we measured their level of autistic traits.
We performed two letter-detection experiments (one in a lab and one online) where participants had to identify a letter when displayed among background visual static of various intensities.
By using the static, we added additional visual noise to the neural noise already present in our participants’ brains. We hypothesised the visual noise would push participants with low internal brain noise (or low autistic traits) to perform better (as suggested by previous research on stochastic resonance). The more interesting prediction was that noise would not help individuals who already had a lot of brain noise (that is, those with high autistic traits), because their own neural noise already ensured optimal performance.
Indeed, one of our experiments showed people with high neural noise (high autistic traits) did not benefit from additional noise. Moreover, they showed superior performance (greater accuracy) relative to people with low neural noise when the added visual static was low. This suggests their own neural noise already caused a natural stochastic resonance effect, resulting in better performance.
It is important to note we did not include clinically diagnosed autistic participants, but overall, we showed the theory of enhanced performance due to stochastic resonance in autism has merits.
Why this is important?
Autistic people face ignorance, prejudice and discrimination that can harm wellbeing. Poor mental and physical health, reduced social connections and increased “camouflaging” of autistic traits are some of the negative impacts that autistic people face.
So, research underlining and investigating the strengths inherent in autism can help reduce stigma, allow autistic people to be themselves and acknowledge autistic people do not require “fixing”.
The autistic brain is different. It comes with limitations, but it also has its strengths.
Pratik Raul, PhD candidiate, University of Canberra; Jeroen van Boxtel, Associate professor, University of Canberra, and Jovana Acevska, Honours Graduate Student, University of Canberra
This article is republished from The Conversation under a Creative Commons license. Read the original article.

Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Art and Science of Connection – by Kasley Killam, MPH
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We can eat well, exercise well, and even sleep well, and we’ll still have a +53% increased all-cause mortality if we lack social connection—even if we technically have support and access to social resources, just not the real human connection itself. And as we get older, it gets increasingly easy to find ourselves isolated.
The author is a social scientist by profession, and it shows. None of what she shares in the book is wishy-washy; it has abundant scientific references coming thick and fast, and a great deal of clarity with regard to terms, something often not found in books of this genre that lean more towards the art than the science.
On which note, for the reader who may be thinking “I am indeed quite alone”, she also offers proven techniques for remedying that; not in the way that many books use the word “proven” to mean “we got some testimonials”, but rather, proven in the sense of “we did science to it and based on these 17 large population-based retrospective cohort studies, we can say with 99% confidence that this is an effective tool to mediate improved social bonds and social health outcomes”.
To this end, it’s a very practical book also, and should bestow upon any isolated reader a sense of confidence that in fact, things can be better. A particular strength is that it also looks at many different scenarios, so for the “what if I…” people with clear reasons why social connection is not abundantly available, yes, she has such cases covered too.
Bottom line: if you’d like to live more healthily for longer, social health is an underrated and oft-forgotten way of greatly increasing those things, by science.
Click here to check out The Art And Science Of Social Connection, and get connected!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: