Aging with Grace – by Dr. David Snowdon
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First, what this book is not: a book about Christianity. Don’t worry, we didn’t suddenly change the theme of 10almonds.
Rather, what this book is: a book about a famous large (n=678) study into the biology of aging, that took a population sample of women who had many factors already controlled-for, e.g. they ate the same food, had the same schedule, did the same activities, etc—for many years on end. In other words, a convent of nuns.
This allowed for a lot more to be learned about other factors that influence aging, such as:
- Heredity / genetics in general
- Speaking more than one language
- Supplementing with vitamins or not
- Key adverse events (e.g. stroke)
- Key chronic conditions (e.g. depression)
The book does also cover (as one might expect) the role that community and faith can play in healthy longevity, but since the subjects were 678 communally-dwelling people of faith (thus: no control group of faithless loners), this aspect is discussed only in anecdote, or in reference to other studies.
The author of this book, by the way, was the lead researcher of the study, and he is a well-recognised expert in the field of Alzheimer’s in particular (and Alzheimer’s does feature quite a bit throughout).
The writing style is largely narrative, and/but with a lot of clinical detail and specific data; this is by no means a wishy-washy book.
Bottom line: if you’d like to know what nuns were doing in the 1980s to disproportionally live into three-figure ages, then this book will answer those questions.
Click here to check out Aging with Grace, and indeed age with grace!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

No, sugar doesn’t make your kids hyperactive

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s a Saturday afternoon at a kids’ birthday party. Hordes of children are swarming between the spread of birthday treats and party games. Half-eaten cupcakes, biscuits and lollies litter the floor, and the kids seem to have gained superhuman speed and bounce-off-the-wall energy. But is sugar to blame?
The belief that eating sugary foods and drinks leads to hyperactivity has steadfastly persisted for decades. And parents have curtailed their children’s intake accordingly.
Balanced nutrition is critical during childhood. As a neuroscientist who has studied the negative effects of high sugar “junk food” diets on brain function, I can confidently say excessive sugar consumption does not have benefits to the young mind. In fact, neuroimaging studies show the brains of children who eat more processed snack foods are smaller in volume, particularly in the frontal cortices, than those of children who eat a more healthful diet.
But today’s scientific evidence does not support the claim sugar makes kids hyperactive.

Sharomka/Shutterstock The hyperactivity myth
Sugar is a rapid source of fuel for the body. The myth of sugar-induced hyperactivity can be traced to a handful of studies conducted in the 1970s and early 1980s. These were focused on the Feingold Diet as a treatment for what we now call Attention Deficit Hyperactivity Disorder (ADHD), a neurodivergent profile where problems with inattention and/or hyperactivity and impulsivity can negatively affect school, work or relationships.
Devised by American paediatric allergist Benjamin Feingold, the diet is extremely restrictive. Artificial colours, sweeteners (including sugar) and flavourings, salicylates including aspirin, and three preservatives (butylated hydroxyanisole, butylated hydroxytoluene, and tert-Butrylhdryquinone) are eliminated.
Salicylates occur naturally in many healthy foods, including apples, berries, tomatoes, broccoli, cucumbers, capsicums, nuts, seeds, spices and some grains. So, as well as eliminating processed foods containing artificial colours, flavours, preservatives and sweeteners, the Feingold diet eliminates many nutritious foods helpful for healthy development.
However, Feingold believed avoiding these ingredients improved focus and behaviour. He conducted some small studies, which he claimed showed a large proportion of hyperactive children responded favourably to his diet.
Even it doesn’t make kids hyperactive, they shouldn’t have too much sugar. DenisMArt/Shutterstock Flawed by design
The methods used in the studies were flawed, particularly with respect to adequate control groups (who did not restrict foods) and failed to establish a causal link between sugar consumption and hyperactive behaviour.
Subsequent studies suggested less than 2% responded to restrictions rather than Feingold’s claimed 75%. But the idea still took hold in the public consciousness and was perpetuated by anecdotal experiences.
Fast forward to the present day. The scientific landscape looks vastly different. Rigorous research conducted by experts has consistently failed to find a connection between sugar and hyperactivity. Numerous placebo-controlled studies have demonstrated sugar does not significantly impact children’s behaviour or attention span.
One landmark meta-analysis study, published almost 20 years ago, compared the effects of sugar versus a placebo on children’s behaviour across multiple studies. The results were clear: in the vast majority of studies, sugar consumption did not lead to increased hyperactivity or disruptive behaviour.
Subsequent research has reinforced these findings, providing further evidence sugar does not cause hyperactivity in children, even in those diagnosed with ADHD.
While Feingold’s original claims were overstated, a small proportion of children do experience allergies to artificial food flavourings and dyes.
Pre-school aged children may be more sensitive to food additives than older children. This is potentially due to their smaller body size, or their still-developing brain and body.
Hooked on dopamine?
Although the link between sugar and hyperactivity is murky at best, there is a proven link between the neurotransmitter dopamine and increased activity.
The brain releases dopamine when a reward is encountered – such as an unexpected sweet treat. A surge of dopamine also invigorates movement – we see this increased activity after taking psychostimulant drugs like amphetamine. The excited behaviour of children towards sugary foods may be attributed to a burst of dopamine released in expectation of a reward, although the level of dopamine release is much less than that of a psychostimulant drug.
Dopamine function is also critically linked to ADHD, which is thought to be due to diminished dopamine receptor function in the brain. Some ADHD treatments such as methylphenidate (labelled Ritalin or Concerta) and lisdexamfetamine (sold as Vyvanse) are also psychostimulants. But in the ADHD brain the increased dopamine from these drugs recalibrates brain function to aid focus and behavioural control.
Maybe it’s less of a sugar rush and more of a dopamine rush? Anastasiya Tsiasemnikava/Shutterstock Why does the myth persist?
The complex interplay between diet, behaviour and societal beliefs endures. Expecting sugar to change your child’s behaviour can influence how you interpret what you see. In a study where parents were told their child had either received a sugary drink, or a placebo drink (with a non-sugar sweetener), those parents who expected their child to be hyperactive after having sugar perceived this effect, even when they’d only had the sugar-free placebo.
The allure of a simple explanation – blaming sugar for hyperactivity – can also be appealing in a world filled with many choices and conflicting voices.
Healthy foods, healthy brains
Sugar itself may not make your child hyperactive, but it can affect your child’s mental and physical health. Rather than demonising sugar, we should encourage moderation and balanced nutrition, teaching children healthy eating habits and fostering a positive relationship with food.
In both children and adults, the World Health Organization (WHO) recommends limiting free sugar consumption to less than 10% of energy intake, and a reduction to 5% for further health benefits. Free sugars include sugars added to foods during manufacturing, and naturally present sugars in honey, syrups, fruit juices and fruit juice concentrates.
Treating sugary foods as rewards can result in them becoming highly valued by children. Non-sugar rewards also have this effect, so it’s a good idea to use stickers, toys or a fun activity as incentives for positive behaviour instead.
While sugar may provide a temporary energy boost, it does not turn children into hyperactive whirlwinds.
Amy Reichelt, Senior Lecturer (Adjunct), Nutritional neuroscientist, University of Adelaide
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Alzheimer’s may have once spread from person to person, but the risk of that happening today is incredibly low
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
An article published this week in the prestigious journal Nature Medicine documents what is believed to be the first evidence that Alzheimer’s disease can be transmitted from person to person.
The finding arose from long-term follow up of patients who received human growth hormone (hGH) that was taken from brain tissue of deceased donors.
Preparations of donated hGH were used in medicine to treat a variety of conditions from 1959 onwards – including in Australia from the mid 60s.
The practice stopped in 1985 when it was discovered around 200 patients worldwide who had received these donations went on to develop Creuztfeldt-Jakob disease (CJD), which causes a rapidly progressive dementia. This is an otherwise extremely rare condition, affecting roughly one person in a million.
What’s CJD got to do with Alzehimer’s?
CJD is caused by prions: infective particles that are neither bacterial or viral, but consist of abnormally folded proteins that can be transmitted from cell to cell.
Other prion diseases include kuru, a dementia seen in New Guinea tribespeople caused by eating human tissue, scrapie (a disease of sheep) and variant CJD or bovine spongiform encephalopathy, otherwise known as mad cow disease. This raised public health concerns over the eating of beef products in the United Kingdom in the 1980s.
Human growth hormone used to come from donated organs
Human growth hormone (hGH) is produced in the brain by the pituitary gland. Treatments were originally prepared from purified human pituitary tissue.
But because the amount of hGH contained in a single gland is extremely small, any single dose given to any one patient could contain material from around 16,000 donated glands.
An average course of hGH treatment lasts around four years, so the chances of receiving contaminated material – even for a very rare condition such as CJD – became quite high for such people.
hGH is now manufactured synthetically in a laboratory, rather than from human tissue. So this particular mode of CJD transmission is no longer a risk.
Human growth hormone is now produced in a lab.
National Cancer Institute/UnsplashWhat are the latest findings about Alzheimer’s disease?
The Nature Medicine paper provides the first evidence that transmission of Alzheimer’s disease can occur via human-to-human transmission.
The authors examined the outcomes of people who received donated hGH until 1985. They found five such recipients had developed early-onset Alzheimer’s disease.
They considered other explanations for the findings but concluded donated hGH was the likely cause.
Given Alzheimer’s disease is a much more common illness than CJD, the authors presume those who received donated hGH before 1985 may be at higher risk of developing Alzheimer’s disease.
Alzheimer’s disease is caused by presence of two abnormally folded proteins: amyloid and tau. There is increasing evidence these proteins spread in the brain in a similar way to prion diseases. So the mode of transmission the authors propose is certainly plausible.
However, given the amyloid protein deposits in the brain at least 20 years before clinical Alzheimer’s disease develops, there is likely to be a considerable time lag before cases that might arise from the receipt of donated hGH become evident.
When was this process used in Australia?
In Australia, donated pituitary material was used from 1967 to 1985 to treat people with short stature and infertility.
More than 2,000 people received such treatment. Four developed CJD, the last case identified in 1991. All four cases were likely linked to a single contaminated batch.
The risks of any other cases of CJD developing now in pituitary material recipients, so long after the occurrence of the last identified case in Australia, are considered to be incredibly small.
Early-onset Alzheimer’s disease (defined as occurring before the age of 65) is uncommon, accounting for around 5% of all cases. Below the age of 50 it’s rare and likely to have a genetic contribution.
Early onset Alzheimer’s means it occurs before age 65.
perfectlab/ShutterstockThe risk is very low – and you can’t ‘catch’ it like a virus
The Nature Medicine paper identified five cases which were diagnosed in people aged 38 to 55. This is more than could be expected by chance, but still very low in comparison to the total number of patients treated worldwide.
Although the long “incubation period” of Alzheimer’s disease may mean more similar cases may be identified in the future, the absolute risk remains very low. The main scientific interest of the article lies in the fact it’s first to demonstrate that Alzheimer’s disease can be transmitted from person to person in a similar way to prion diseases, rather than in any public health risk.
The authors were keen to emphasise, as I will, that Alzheimer’s cannot be contracted via contact with or providing care to people with Alzheimer’s disease.

Steve Macfarlane, Head of Clinical Services, Dementia Support Australia, & Associate Professor of Psychiatry, Monash University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Improve Your Insulin Sensitivity!
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve written before about blood sugar management, for example:
10 Ways To Balance Blood Sugars ← this one really is the most solid foundation possible; if you do nothing else, do these 10 things!
And as for why we care:
Good (Or Bad) Health Starts With Your Blood
…because the same things that cause type 2 diabetes, go on to cause many other woes, with particularly strong comorbidities in the case of Alzheimer’s disease and other dementias, as well as heart disease of various kinds, and a long long laundry list of immune dysfunctions / inflammatory disorders in general.
In short, if you can’t keep your blood sugars even, the rest of your health will fall like so many dominoes.
Getting a baseline
Are you counting steps? Counting calories? Monitoring your sleep? Heart rate zones? These all have their merits:
- Steps: One More Resource Against Osteoporosis!
- Calories: Is Cutting Calories The Key To Healthy Long Life?
- Sleep: A Head-To-Head Of Google and Apple’s Top Apps For Getting Your Head Down
- Heart Rate Zones: Heart Rate Zones, Oxalates, & More
But something far fewer people do unless they have diabetes or are very enthusiastic about personal health, is to track blood sugars:
Here’s how: Track Your Blood Sugars For Better Personalized Health
And for understanding some things to watch out for when using a continuous glucose monitor:
Continuous Glucose Monitors Without Diabetes: Pros & Cons
Writer’s anecdote: I decided to give one a try for a few months, and so far it has been informative, albeit unexciting. It seems that with my diet (mostly whole-foods plant based, though I do have a wholegrain wheat product about twice per week (usually: flatbread once, pasta once) which is… Well, we could argue it’s whole-food plant based, but let’s be honest, it’s a little processed), my blood sugars don’t really have spikes at all; the graph looks more like gently rolling low hills (which is good). However! Even so, by experimenting with it, I can see for myself what differences different foods/interventions make to my blood sugars, which is helpful, and it also improves my motivation for intermittent fasting. It also means that if I think “hmm, my energy levels are feeling low; I need a snack” I can touch my phone to my arm and find out if that is really the reason (so far, it hasn’t been). I expect that as I monitor my blood sugars continuously and look at the data frequently, I’ll start to get a much more intuitive feel for my own blood sugars, in much the same way I can generally intuit my hormone levels correctly after years of taking-and-testing.
So much for blood sugars. Now, what about insulin?
Step Zero
If taking care of blood sugars is step one, then taking care of insulin is step zero.
Often’s it’s viewed the other way around: we try to keep our blood sugars balanced, to reduce the need for our bodies to produce so much insulin that it gets worn out. And that’s good and fine, but…
To quote what we wrote when reviewing “Why We Get Sick” last month:
❝Dr. Bikman makes the case that while indeed hyper- or hypoglycemia bring their problems, mostly these are symptoms rather than causes, and the real culprit is insulin resistance, and this is important for two main reasons:
- Insulin resistance occurs well before the other symptoms set in (which means: it is the thing that truly needs to be nipped in the bud; if your fasting blood sugars are rising, then you missed “nipping it in the bud” likely by a decade or more)
- Insulin resistance causes more problems than “mere” hyperglycemia (the most commonly-known result of insulin resistance) does, so again, it really needs to be considered separately from blood sugar management.
This latter, Dr. Bikman goes into in great detail, linking insulin resistance (even if blood sugar levels are normal) to all manner of diseases (hence the title).
You may be wondering: how can blood sugar levels be normal, if we have insulin resistance?
And the answer is that for as long as it is still able, your pancreas will just faithfully crank out more and more insulin to deal with the blood sugar levels that would otherwise be steadily rising. Since people measure blood sugar levels much more regularly than anyone checks for actual insulin levels, this means that one can be insulin resistant for years without knowing it, until finally the pancreas is no longer able to keep up with the demand—then that’s when people finally notice.❞
You can read the full book review here:
Now, testing for insulin is not so quick, easy, or accessible as testing for glucose, but it can be worthwhile to order such a test—because, as discussed, your insulin levels could be high even while your blood sugars are still normal, and it won’t be until the pancreas finally reaches breaking point that your blood sugars show it.
So, knowing your insulin levels can help you intervene before your pancreas reaches that breaking point.
We can’t advise on local services available for ordering blood tests (because they will vary depending on location), but a simple Google search should suffice to show what’s available in your region.
Once you know your insulin levels (or even if you don’t, but simply take the principled position that improving insulin sensitivity will be good regardless), you can set about managing them.
Insulin sensitivity is important, because the better it is (higher insulin sensitivity), the less insulin the pancreas has to make to tidy up the same amount of glucose into places that are good for it to go—which is good. In contrast, the worse it is (higher insulin resistance), the more insulin the pancreas has to make to do the same blood sugar management. Which is bad.
What to do about it
We imagine you will already be eating in a way that is conducive to avoiding or reversing type 2 diabetes, but for anyone who wants a refresher,
See: How To Prevent And Reverse Type 2 Diabetes
…which yes, as well as meaning eating/avoiding certain foods, does recommend intermittent fasting. For anyone who wants a primer on that,
See: Intermittent Fasting: Methods & Benefits
There are also drugs you may want to consider:
Metformin Without Diabetes, For Weight-Loss & More
And “nutraceuticals” that sound like drugs, for example:
Glutathione’s Benefits: The Usual And The Unique ← the good news is, it’s found in several common foods
You may have heard the hype about “nature’s Ozempic”, and berberine isn’t exactly that (works in mostly different ways), but its benefits do include improving insulin sensitivity:
Berberine For Metabolic Health
Lastly, while eating for blood sugar management is all well and good, do be aware that some things affect insulin levels without increased blood sugar levels. So even if you’re using a CGM, you may go blissfully unaware of an insulin spike, because there was no glucose spike on the graph—and in contrast, there could even be a dip in blood sugar levels, if you consumed something that increased insulin levels without providing glucose at the same time, making you think “I should have some carbs”, which visually on the graph would even out your blood sugars, but invisibly, would worsen the already-extant insulin spike.
Read more about this: Strange Things Happening In The Islets Of Langerhans: When Carbs, Proteins, & Fats Switch Metabolic Roles
Now, since you probably can’t test your insulin at a moment’s notice, the way to watch out for this is “hmm, I ate some protein/fats (delete as applicable) without carbs and my blood sugars dipped; I know what’s going on here”.
Want to know more?
We heartily recommend the “Why We Get Sick” book we linked above, as this focuses on insulin resistance/sensitivity itself!
However, a very good general primer on blood sugar management (and thus, by extension, at least moderately good insulin management), is:
Glucose Revolution: The Life-Changing Power of Balancing Your Blood Sugar – by Jessie Inchauspé
Enjoy!
Share This Post






Related Posts
-

Getting to Neutral – by Trevor Moawad
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We all know that a pessimistic outlook is self-defeating… And yet, toxic positivity can also be a set-up for failure! At some point, reckless faith in the kindly nature of the universe will get crushed, badly. Sometimes that point is a low point in life… sometimes it’s six times a day. But one thing’s for sure: we can’t “just decide everything will go great!” because the world just doesn’t work that way.
That’s where Trevor Moawad comes in. “Getting to neutral” is not a popular selling point. Everyone wants joy, abundance, and high after high. And neutrality itself is often associated with boredom and soullessness. But, Moawad argues, it doesn’t have to be that way.
This book’s goal—which it accomplishes well—is to provide a framework for being a genuine realist. What does that mean?
“I’m not a pessimist; I’m a realist” – every pessimist ever.
^Not that. That’s not what it means. What it means instead is:
- Hope for the best
- Prepare for the worst
- Adapt as you go
…taking care to use past experiences to inform future decisions, but without falling into the trap of thinking that because something happened a certain way before, it always will in the future.
To be rational, in short. Consciously and actively rational.
Feel the highs! Feel the lows! But keep your baseline when actually making decisions.
Bottom line: this book is as much an antidote to pessimism and self-defeat, as it is to reckless optimism and resultant fragility. Highly recommendable.
Click here to check out “Getting to Neutral” and start creating your best, most reason-based life!
PS: in this book, Moawad draws heavily from his own experiences of battling adversity in the form of cancer—of which he died, before this book’s publication. A poignant reminder that he was right: we won’t always get the most positive outcome of any given situation, so what matters the most is making the best use of the time we have.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Are Brain Chips Safe?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Ready For Cyborgization?

In yesterday’s newsletter, we asked you for your views on Brain-Computer Interfaces (BCIs), such as the Utah Array and Neuralink’s chips on/in brains that allow direct communication between brains and computers, so that (for example) a paralysed person can use a device to communicate, or manipulate a prosthetic limb or two.
We didn’t get as many votes as usual; it’s possible that yesterday’s newsletter ended up in a lot of spam filters due to repeated use of a word in “extra ______ olive oil” in its main feature!
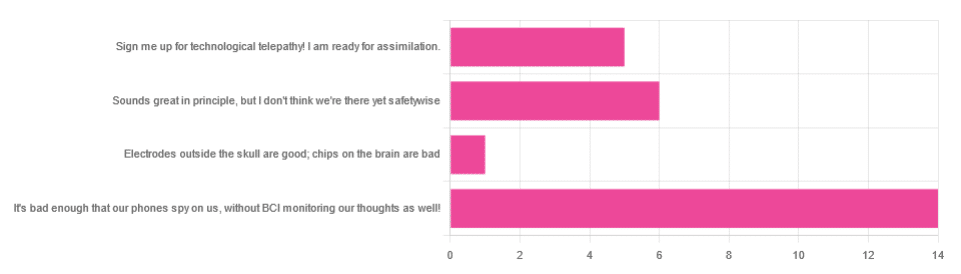
However, of the answers we did get…
- About 54% said “It’s bad enough that our phones spy on us, without BCI monitoring our thoughts as well!”
- About 23% said “Sounds great in principle, but I don’t think we’re there yet safetywise”
- About 19% said “Sign me up for technological telepathy! I am ready for assimilation”
- One (1) person said “Electrode outside the skull are good; chips on the brain are bad”
But what does the science say?
We’re not there yet safetywise: True or False?
True, in our opinion, when it comes to the latest implants, anyway. While it’s very difficult to prove a negative (it could be that everything goes perfectly in human trials), “extraordinary claims require extraordinary evidence”, and so far this seems to be lacking.
The stage before human trials is usually animal trials, starting with small creatures and working up to non-human primates if appropriate, before finally humans.
- Good news: the latest hot-topic BCI device (Neuralink) was tested on animals!
- Bad news: to say it did not go well would be an understatement
The Gruesome Story of How Neuralink’s Monkeys Actually Died
The above is a Wired article, and we tend to go for more objective sources, however we chose this one because it links to very many objective sources, including an open letter from the Physicians’ Committee for Responsible Medicine, which basically confirms everything in the Wired article. There are lots of links to primary (medical and legal) sources, too.
Electrodes outside the skull are good; chips on/in the brain are bad: True or False?
True or False depending on how they’re done. The Utah Array (an older BCI implant, now 20 years old, though it’s been updated many times since) has had a good safety record, after being used by a few dozen people with paralysis to control devices:
How the Utah Array is advancing BCI science
The Utah Array works on the same general principle as Neuralink, but the mechanics of its implementation are very different:
- The Utah Array involves a tiny bundle of microelectrodes (held together by a rigid structure that looks a bit like a nanoscale hairbrush) put in place by a brain surgeon, and that’s that.
- The Neuralink has a dynamic web of electrodes, implanted by a little robot that acts like a tiny sewing machine to implant many polymer threads, each containing its own a bunch of electrodes.
In theory, the latter is much more advanced. In practice, so far, the former has a much better safety record.
I am right to be a little worried about giving companies access to my brain: True or False?
True or False, depending on the nature of your concern.
For privacy: current BCI devices have quite simple switches operated consciously by the user. So while technically any such device that then runs its data through Bluetooth or WiFi could be hacked, this risk is no greater than using a wireless mouse and/or keyboard, because it has access to about the same amount of information.
For safety: yes, probably there is cause to be worried. Likely the first waves of commercial users of any given BCI device will be severely disabled people who are more likely to waive their rights in the hope of a life-changing assistance device, and likely some of those will suffer if things go wrong.
Which on the one hand, is their gamble to make. And on the other hand, makes rushing to human trials, for companies that do that, a little more predatory.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What Curiosity Really Kills
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Curiosity Kills The Neurodegeneration
Of the seven things that Leonardo da Vinci considered most important for developing and maintaining the mind, number one on his list was curiosity, and we’re going to be focussing on that today.
In case you are curious about what seven things made Leonardo’s* list, they were:
- Curiosità: an insatiably curious approach to life and an unrelenting quest for continuous learning
- Dimostrazione: a commitment to test knowledge through experience, persistence, and a willingness to learn from mistakes
- Sensazione: the continual refinement of the senses, especially sight, as a means to enliven experience
- Sfumato: (lit: “gone up in smoke”) a willingness to embrace ambiguity, paradox, and uncertainty
- Arte/Scienza: the curated balance of art and science, imagination and logic
- Corporalità: the cultivation of physical grace, ambidexterity, and fitness
- Connessione: a recognition of and appreciation for the interconnectedness of phenomena (systems-based thinking)
*In case you are curious why we wrote “Leonardo” and not “da Vinci” as per our usual convention of shortening names to last names, da Vinci is not technically a name, in much the same way as “of Nazareth” was not a name.
You can read more about all 7 of these in a book that we’ve reviewed previously:
How to Think Like Leonardo da Vinci: Seven Steps to Genius Every Day – by Michael J. Gelb
But for now, let’s take on “curiosity”!
If you need an extra reason to focus on growing and nurturing your curiosity, it was also #1 of Dr. Daniel Levitin’s list of…
The Five Keys Of Aging Healthily
…and that’s from a modern-day neuroscientist whose research focuses on aging, the brain, health, productivity, and creativity.
But how do we foster curiosity in the age of Google?
Curiosity is like a muscle: use it or lose it
While it’s true that many things can be Googled to satisfy one’s curiosity in an instant…
- do you? It’s only useful if you do use it
- is the top result on Google reliable?
- there are many things that aren’t available there
In short: douse “fast
foodinformation” sources, but don’t rely on them! Not just for the sake of having correct information, but also: for the actual brain benefits which is what we are aiming for here with today’s article.If you want the best brain benefits, dive in, and go deep
Here at 10almonds we often present superficial information, with links to deeper information (often: scholarly articles). We do this because a) there’s only so much we can fit in our articles and b) we know you only have so much time available, and/but may choose to dive deeper.
Think of it in layers, e.g:
- Collagen is good for joints and bones
- Collagen is a protein made of these amino acids that also requires these vitamins and minerals to be present in order to formulate it
- Those amino acids are needed in these quantities, of which this particular one is usually the weakest link that might need supplementing, and those vitamins and minerals need to be within this period of time, but not these ones at the exact same time, or else it will disrupt the process of collagen synthesis
(in case you’re curious, we covered this here and here and offered a very good, very in-depth book about it here)
Now, this doesn’t mean that to have a healthy brain you need to have the equivalent knowledge of an anatomy & physiology degree, but it is good to have that level of curiosity in at least some areas of your life—and the more, the better.
Top tips for developing a habit of curiosity
As you probably know, most of our endeavors as humans go best when they are habits:
How To Really Pick Up (And Keep!) Those Habits
And as for specifically building a habit of curiosity:
- Make a deal with yourself that when someone is excited to tell you what they know about something (no matter whether it is your grandkid, or the socially awkward nerd at a party, or whoever), listen and learn, no matter the topic.
- Learn at least one language other than your native language (presumably English for most of our readers). Not only does learning a language convey a lot of brain benefits of its own, but also, it is almost impossible to separate language learning from cultural learning, and so you will learn a lot about another culture too, and have whole new worlds opened up to you. Again, more is better, but one second language is already a lot better than none.
- Make a regular habit of going to your local library, and picking out a non-fiction book to take home and read. This has an advantage over a bookshop, by the way (and not just that the library is free): since library books must be returned, you will keep going back, and build a habit of taking out books.
- Pick a skill that you’d like to make into a fully-fledged hobby, and commit to continually learning as much about it as you can. We already covered language-learning above, but others might include: gardening (perhaps a specific kind), cooking (perhaps a specific kind), needlecraft (perhaps a specific kind), dance (perhaps a specific kind). You could learn a musical instrument. Or it could be something very directly useful, like learning to be a first responder in case of emergencies, and committing to continually learning more about it (because there is always more to learn).
And when it comes to the above choices… Pick things that excite you, regardless of how practical or not they are. Because that stimulation that keeps on driving you? That’s what keeps your brain active, healthy, and sharp.
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: