We’re only using a fraction of health workers’ skills. This needs to change
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Roles of health professionals are still unfortunately often stuck in the past. That is, before the shift of education of nurses and other health professionals into universities in the 1980s. So many are still not working to their full scope of practice.
There has been some expansion of roles in recent years – including pharmacists prescribing (under limited circumstances) and administering a wider range of vaccinations.
But the recently released paper from an independent Commonwealth review on health workers’ “scope of practice” identifies the myriad of barriers preventing Australians from fully benefiting from health professionals’ skills.
These include workforce design (who does what, where and how roles interact), legislation and regulation (which often differs according to jurisdiction), and how health workers are funded and paid.
There is no simple quick fix for this type of reform. But we now have a sensible pathway to improve access to care, using all health professionals appropriately.
A new vision for general practice
I recently had a COVID booster. To do this, I logged onto my general practice’s website, answered the question about what I wanted, booked an appointment with the practice nurse that afternoon, got jabbed, was bulk-billed, sat down for a while, and then went home. Nothing remarkable at all about that.
But that interaction required a host of facilitating factors. The Victorian government regulates whether nurses can provide vaccinations, and what additional training the nurse requires. The Commonwealth government has allowed the practice to be paid by Medicare for the nurse’s work. The venture capitalist practice owner has done the sums and decided allocating a room to a practice nurse is economically rational.
The future of primary care is one involving more use of the range of health professionals, in addition to GPs.
It would be good if my general practice also had a physiotherapist, who I could see if I had back pain without seeing the GP, but there is no Medicare rebate for this. This arrangement would need both health professionals to have access to my health record. There also needs to be trust and good communication between the two when the physio might think the GP needs to be alerted to any issues.
This vision is one of integrated primary care, with health professionals working in a team. The nurse should be able to do more than vaccination and checking vital signs. Do I really need to see the GP every time I need a prescription renewed for my regular medication? This is the nub of the “scope of practice” issue.
How about pharmacists?
An integrated future is not the only future on the table. Pharmacy owners especially have argued that pharmacists should be able to practise independently of GPs, prescribing a limited range of medications and dispensing them.
This will inevitably reduce continuity of care and potentially create risks if the GP is not aware of what other medications a patient is using.
But a greater role for pharmacists has benefits for patients. It is often easier and cheaper for the patient to see a pharmacist, especially as bulk billing rates fall, and this is one of the reasons why independent pharmacist prescribing is gaining traction.

Every five years or so the government negotiates an agreement with the Pharmacy Guild, the organisation of pharmacy owners, about how much pharmacies will be paid for dispensing medications and other services. These agreements are called “Community Pharmacy Agreements”. Paying pharmacists independent prescribing may be part of the next agreement, the details of which are currently being negotiated.
GPs don’t like competition from this new source, even though there will be plenty of work around for GPs into the foreseeable future. So their organisations highlight the risks of these changes, reopening centuries old turf wars dressed up as concerns about safety and risk.
Who pays for all this?
Funding is at the heart of disputes about scope of practice. As with many policy debates, there is merit on both sides.
Clearly the government must increase its support for comprehensive general practice. Existing funding of fee-for-service medical benefits payments must be redesigned and supplemented by payments that allow practices to engage a range of other health professionals to create health-care teams.
This should be the principal direction of primary care reform, and the final report of the scope of practice review should make that clear. It must focus on the overall goal of better primary care, rather than simply the aspirations of individual health professionals, and working to a professional’s full scope of practice in a team, not a professional silo.
In parallel, governments – state and federal – must ensure all health professionals are used to their best of their abilities. It is a waste to have highly educated professionals not using their skills fully. New funding arrangements should facilitate better access to care from all appropriately qualified health professionals.
In the case of prescribing, it is possible to reconcile the aspirations of pharmacists and the concerns of GPs. New arrangements could be that pharmacists can only renew medications if they have agreements with the GP and there is good communication between them. This may be easier in rural and suburban areas, where the pharmacists are better known to the GPs.
The second issues paper points to the complexity of achieving scope of practice reforms. However, it also sets out a sensible path to improve access to care using all health professionals appropriately.
Stephen Duckett, Honorary Enterprise Professor, School of Population and Global Health, and Department of General Practice and Primary Care, The University of Melbourne
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Is TikTok right? Can adding a teaspoon of cinnamon to your coffee help you burn fat?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cinnamon has been long used around the world in both sweet and savoury dishes and drinks.
But a new TikTok trend claims adding a teaspoon of cinnamon to your daily coffee (and some cocoa to make it more palatable) for one week can help you burn fat. Is there any truth to this?

Evannovostro/Shutterstock Not all cinnamon is the same
There are two types of cinnamon, both of which come from grinding the bark of the cinnamomum tree and may include several naturally occurring active ingredients.
Cassia cinnamon is the most common type available in grocery stores. It has a bitter taste and contains higher levels of one of the active ingredient cinnamaldehyde, a compound that gives cinnamon its flavour and odour. About 95% of cassia cinnamon is cinnamaldehyde.
The other is Ceylon cinnamon, which tastes sweeter. It contains about 50-60% cinnamaldehyde.
Does cinnamon burn fat? What does the research say?
A review of 35 studies examined whether consuming cinnamon could affect waist circumference, which is linked to increased body fat levels. It found cinnamon doses below 1.5 grams per day (around half a teaspoon) decreased waist circumference by 1.68cm. However, consuming more than 1.5g/day did not have a significant effect.
A meta-analysis of 21 clinical trials with 1,480 total participants found cinnamon also reduced body mass index (BMI) by 0.40kg/m² and body weight by 0.92kg. But it did not change the participants’ composition of fat or lean mass.
Another umbrella review, which included all the meta-analyses, found a small effect of cinnamon on weight loss. Participants lost an average of 0.67kg and reduced their BMI by 0.45kg/m².
The effect appears small. Radu Sebastian/Shutterstock So overall, the weight loss we see from these high-quality studies is very small, ranging anywhere from two to six months and mostly with no change in body composition.
The studies included people with different diseases, and most were from the Middle East and/or the Indian subcontinent. So we can’t be certain we would see this effect in people with other health profiles and in other countries. They were also conducted over different lengths of time from two to six months.
The supplements were different, depending on the study. Some had the active ingredient extracted from cinnamon, others used cinnamon powder. Doses varied from 0.36g to 10g per day.
They also used the two different types of cinnamon – but none of the studies used cinnamon from the grocery store.
How could cinnamon result in small amounts of weight loss?
There are several possible mechanisms.
It appears to allow blood glucose (sugar) to enter the body’s cells more quickly. This lowers blood glucose levels and can make insulin work more effectively.
It also seems to improve the way we break down fat when we need it for energy.
Finally, it may make us feel fuller for longer by slowing down how quickly the food is released from our stomach into the small intestine.
What are the risks?
Cinnamon is generally regarded as safe when used as a spice in cooking and food.
However, in recent months the United States and Australia have issued health alerts about the level of lead and other heavy metals in some cinnamon preparations.
Lead enters as a contaminant during growth (from the environment) and in harvesting. In some cases, it has been suggested there may have been intentional contamination.
Some people can have side effects from cinnamon, including gastrointestinal pain and allergic reactions.
One of the active ingredients, coumarin, can be toxic for some people’s livers. This has prompted the European Food Authority to set a limit of 0.1mg/kg of body weight.
Cassia cinnamon contains up to 1% of coumarin, and the Ceylon variety contains much less, 0.004%. So for people weighing above 60kg, 2 teaspoons (6g) of cassia cinnamon would bring them over the safe limit.
What about the coffee and cocoa?
Many people may think coffee can also help us lose weight. However there isn’t good evidence to support this yet.
An observational study found drinking one cup of regular coffee was linked to a reduction in weight that is gained over four years, but by a very small amount: an average of 0.12kg.
Good-quality cocoa and dark chocolate have also been shown to reduce weight. But again, the weight loss was small (between 0.2 and 0.4kg) and only after consuming it for four to eight weeks.
So what does this all mean?
Using cinnamon may have a very small effect on weight, but it’s unlikely to deliver meaningful weight loss without other lifestyle adjustments.
We also need to remember these trials used products that differ from the cinnamon we buy in the shops. How we store and how long we keep cinnamon might also impact or degrade the active ingredients.
And consuming more isn’t going to provide additional benefit. In fact, it could increase your risk of side effects.
So if you enjoy the taste of cinnamon in your coffee, continue to add it, but given its strong taste, you’re likely to only want to add a little.
And no matter how much we’d like this to be true, we certainly won’t gain any fat-loss benefits by consuming cinnamon on doughnuts or in buns, due to their high kilojoule count.
If you want to lose weight, there are evidence-backed approaches that won’t spoil your morning coffee.
Evangeline Mantzioris, Program Director of Nutrition and Food Sciences, Accredited Practising Dietitian, University of South Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

A Supplement To Rival St. John’s Wort Against Depression
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Do You Feel The SAMe?
S-Adeonsyl-L-Methionone (SAMe) is a chemical found naturally in the body, and/but enjoyed widely as a supplement. The main reasons people take it are:
- Improve mood (antidepressant effect)
- Improve joints (reduce osteoarthritis symptoms)
- Improve liver (detoxifying effect)
Let’s see what the science says for each of those claims…
Does it improve mood?
It seems to perform comparably to St. John’s Wort (which is good; it performs comparably to Prozac).
Best of all, it does this with fewer contraindications (St. John’s Wort has so many contraindications).
Here’s how they stack up:
This looks very promising, though it’d be nice to see a larger body of research, to be sure.
Does it reduce osteoarthritis symptoms?
The good news: it performs comparably to ibuprofen, with fewer side effects!
The bad news: it also performs comparably to placebo!
Read into that what you will about ibuprofen’s usefulness vs OA symptoms.
Read all about it:
S-Adenosylmethionine for osteoarthritis of the knee or hip
If you were hoping for something for OA or similar symptoms, you might like our previous main features:
- Avoiding/Managing Osteoarthritis
- Managing Chronic Pain (Realistically!)
- The 7 Approaches To Pain Management
- (Science-Based) Alternative Pain Relief
Does it help against liver disease?
According to adverts for SAMe: absolutely!
According to science: we don’t know
The science for this is so weak that it’d be unworthy of mention if it weren’t for the fact that SAMe is so widely sold as good against hepatotoxicity.
To be clear: maybe it really is great! Science hasn’t yet disproved its usefulness either.
It is popularly assumed to be beneficial due to there being an association between lower levels of SAMe in the body (remember, it is also produced inside our bodies) and development of liver disease, especially cholestasis.
Here’s an example of what pretty much every study we found was like (inconclusive research based mostly on mice):
S-adenosylmethionine in liver health, injury, and cancer
For other options for liver health, consider:
Is it safe?
Safety trials have been done ranging from 3 months to 2 years, with no serious side effects coming to light. So, it appears quite safe.
That said, as with anything, there are contraindications, such as:
- if you have bipolar disorder, skip this unless directed by your health care provider, because it may worsen the symptoms of mania
- if you are on SSRIs or other serotonergic drugs, it may interact with those
- if you are immunocompromised, you might want to skip it can increase the risk of P. carinii growth in such cases
As always, do speak with your doctor/pharmacist for personalized advice.
Summary
SAMe’s evidence-based qualities seem to stack up as follows:
- Against depression: good
- Against osteoarthritis: weak
- Against liver disease: unknown
As for safety, it has been found quite safe for most people.
Where can I get it?
We don’t sell it, but here is an example product on Amazon, for your convenience
Enjoy!
Share This Post
-

Uric Acid’s Extensive Health Impact (And How To Lower It)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Uric Acid’s Extensive Health Impact (And How To Lower It)

This is Dr. David Perlmutter. He’s a medical doctor, and a Fellow of the American College of Nutrition. He’s a member of the Editorial Board for the Journal of Alzheimer’s Disease, and has been widely published in many other peer-reviewed journals.
What does he want us to know?
He wants us to know about the health risks of uric acid (not something popularly talked about so much!), and how to reduce it.
First: what is it? Uric acid is a substance we make in our own body. However, unlike most substances we make in our body, we have negligible use for it—it’s largely a waste product, usually excreted in urine.
However, if we get too much, it can build up (and crystallize), becoming such things as kidney stones, or causing painful inflammation if it shows up in the joints, as in gout.
More seriously (unpleasant as kidney stones and gout may be), this inflammation can have a knock-on effect triggering (or worsening) other inflammatory conditions, ranging from non-alcoholic fatty liver disease, to arthritis, to dementia, and even heart problems. See for example:
- David Perlmutter | Uric Acid and Cognitive Decline
- American Heart Association | Uric acid linked to later risk for irregular heart rhythm
- World Journal of Gastroenterology | The role of uric acid in non-alcoholic steatohepatitis development
How can we reduce our uric acid levels?
Uric acid is produced when we metabolize purine nucleotides, which are found in many kinds of food. We can therefore reduce our uric acid levels by reducing our purine intake, as well as things that mess up our liver’s ability to detoxify things. Offsetting the values for confounding variables (such as fiber content, or phytochemicals that mitigate the harm), the worst offenders include…
Liver-debilitating things:
- Alcohol (especially beer)
- High-fructose corn syrup (and other fructose-containing things that aren’t actual fruit)
- Other refined sugars
- Wheat / white flour products (this is why beer is worse than wine, for example; it’s a double-vector hit)
Purine-rich things:
- Red meats and game
- Organ meats
- Oily fish, and seafood (great for some things; not great for this)
Some beans and legumes are also high in purines, but much like real fruit has a neutral or positive effect on blood sugar health despite its fructose content, the beans and legumes that are high in purines, also contain phytochemicals that help lower uric acid levels, so have a beneficial effect.
Eggs (consumed in moderation) and tart cherries have a uric-acid lowering effect.
Water is important for all aspects of health, and doubly important for this.
Hydrate well!
Lifestyle matters beyond diet
The main key here is metabolic health, so Dr. Perlmutter advises the uncontroversial lifestyle choices of moderate exercise and good sleep, as well as (more critically) intermittent fasting. We wrote previously on other things that can benefit liver health:
…in this case, that means the liver gets a break to recuperate (something it’s very good at, but does need to get a chance to do), which means that while you’re not giving it something new to do, it can quickly catch up on any backlog, and then tackle any new things fresh, next time you start eating.
Want to know more about this from Dr. Perlmutter?
You might like his article:
An Integrated Plan for Lowering Uric Acid ← more than we had room for here; he also talks about extra things to include in your diet/supplementation regime for beneficial effects!
And/or his book:
…on which much of today’s main feature was based.
Take care!
Share This Post




Related Posts
-
Workout Advice For Busy People
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Hampton at Hybrid Calisthenics always has very sound advice in his uplifting videos, and this one’s no exception:
Key tips for optimizing workouts without burning out
“We all have the same 24 hours” is a folly when in fact, some of us have more responsibilities and/or other impediments to getting things done (e.g. disabilities).
A quick word on disabilities first: sometimes people are quick to point out Paralympian athletes, and “if they can do it, so can you!” and forget that these people are in the top percentile of the top percentile of the top percentile of human performance. If you wouldn’t disparagingly say “if Simone Biles/Hussein Bolt/Michael Phelps can do it, so can you”, then don’t for Paralympians either 😉
Now, as for Hampton’s advice, he recommends:
Enjoy short, intense workouts:
- You can get effective results in under 30 minutes (or even just a few minutes per day) with compound exercises (e.g., squats, pull-ups).
- Focus on full-body movements also saves time!
- Push closer to failure when possible to maximize efficiency. It’s the last rep where most of the strength gains are made! Same deal with cardiovascular fitness, too. Nevertheless, do take safety into account in both cases, of course.
Time your rest periods:
- Resting for 2–3 minutes between sets ensures optimal recovery.
- Avoid getting distracted during rest by setting a timer to stay focused.
- 10almonds tip: use this time to practice a mindfulness meditation. That will greatly reduce the chance of you becoming distracted.
Remember holistic fitness:
- Fitness isn’t just about exercise; diet, sleep, and stress management are equally important for your fitness as much as for the rest of your health.
- Better sleep and reduced stress will help you exercise more consistently and avoid junk food.
Address burnout:
- If feeling too exhausted to apply these tips, focus on getting better rest and reducing stress first.
- Taking a short break to reset can help in the long run.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- How To Do High Intensity Interval Training (Without Wrecking Your Body)
- How To Rest More Efficiently (Yes, Really)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
How To Stay A Step Ahead Of Peripheral Artery Disease
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Far less well-known than Coronary Artery Disease, it can still result in loss of life and limb (not in that order). Fortunately, there are ways to be on your guard:
What it is
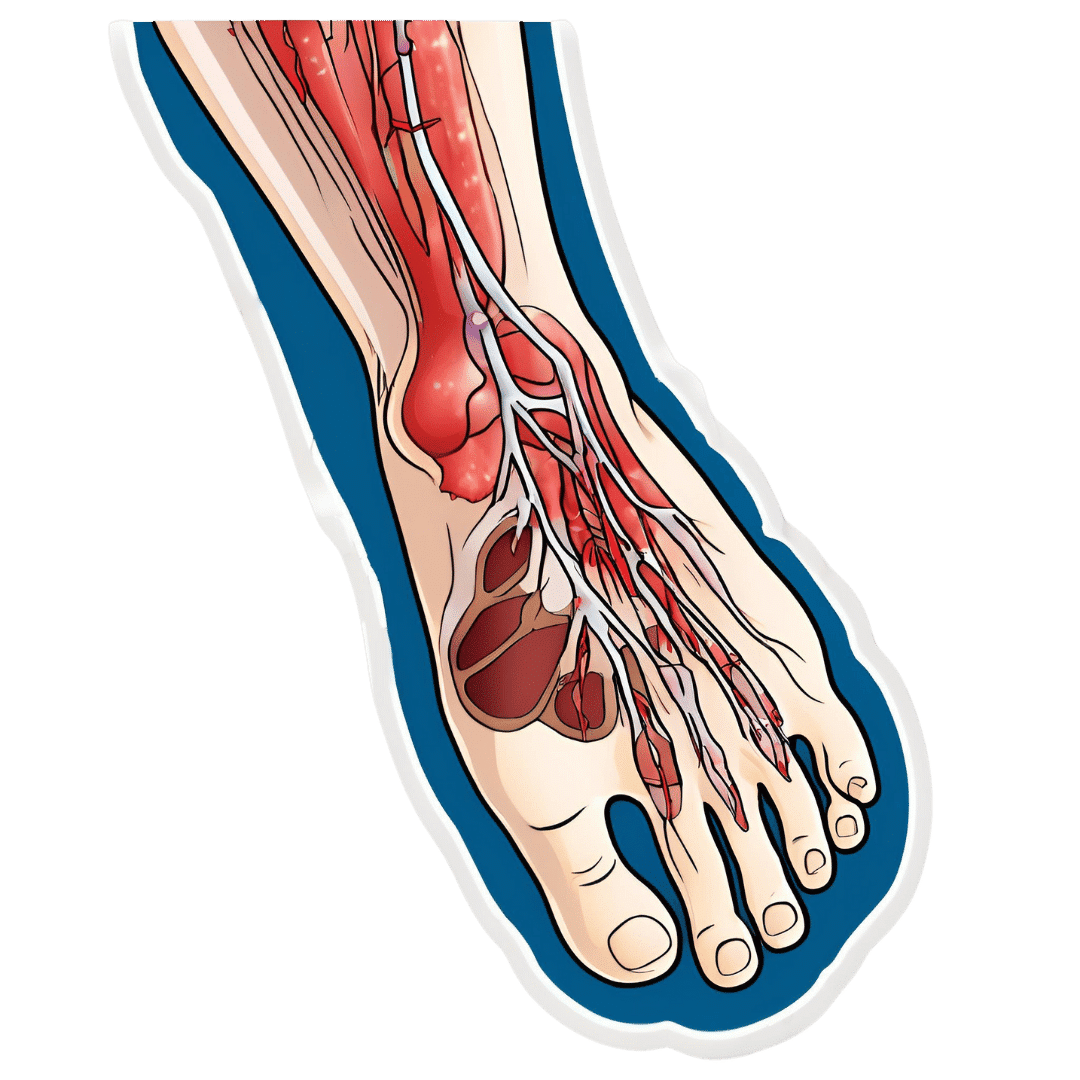
Peripheral Artery Disease (PAD) is the same thing as Coronary Artery Disease (CAD), just, in the periphery—which by definition means “outside of the heart and brain”, but in practice, it starts with the extremities. And of the extremities, it tends to start with the feet and legs, for the simple reason that if someone’s circulation is sluggish, then because of gravity, that’s where’s going to get blocked first.
In both CAD and PAD, the usual root cause is atherosclerosis, that is to say, the build-up of fatty material inside the arteries, usually commensurate to LDL (“bad”) cholesterol, especially in men (high LDL is still a predictor of cardiovascular disease in women though, just more modestly so, at least pre-menopause or in cases of treated menopause whereby HRT has returned hormones to pre-menopause levels).
See also: Demystifying Cholesterol
And for that about sex differences: His & Hers: The Hidden Complexities of Statins and Cardiovascular Disease (CVD)
Why it is
This one’s straightforward, as it’s the same things as any kind of cardiovascular disease: high blood pressure, high cholesterol, older age, obesity, smoking, drinking, diabetes, and genetic factors (so, a risk factor is: family history of heart disease).
However, while those are the main causes and/or risk factors, it absolutely can still strike other people, so it’s as well to be watch out for…
What to look out for
Many people first notice signs and symptoms that turn out to be PAD when they experience pain or numbness in the foot or feet, and/or a discoloration of the feet (especially toes), and slow wound healing.
At that stage, chances are you will need to go urgently to a specialist, and surgery is a likely necessity. With a little luck, it’ll be a minimally-invasive surgery to unblock an artery; failing that, an amputation will be in order.
At that stage, under 50% will be alive 5 years from diagnosis:
You probably want to avoid those. Good news is, you can, by catching it earlier!
What to look out for before that
The most common test for PAD is one you can do at home, but enlisting a nurse to do it for you will help ensure accurate readings. It’s called the Ankle-Brachial Index (ABI) test, and it involves comparing the blood pressure in your ankle with the blood pressure in your arm, and expressing them as a ratio.
Here’s how to do it (instructions and a video demonstration if you want it):
Do Try This At Home: ABI Test For Clogged Arteries
If you need a blood pressure monitor, by the way, here’s an example product on Amazon.
- A healthy ABI score is between 1.0 and 1.4; anything outside this range may indicate arterial problems.
- Low ABI scores (below 0.8) suggest plaque is likely obstructing blood flow
- High ABI scores (above 1.4) may indicate artery hardening
Do note also that yes, if you have plaque obstructing blood flow and hardened arteries, your scores may cancel out and give you a “healthy” score, despite your arteries being very much not healthy.
For this reason, this test can be used to raise the alarm, but not to give the “all clear”.
There are other tests that clinicians can do for you, but you can’t do at home unless you have an MRI machine, a CT scanner, an x-ray machine, a doppler-and-ultrasound machine, etc. We’ll not go into those in detail here, but ask your doctor about them if you’re concerned.
What to do about it
In the mid-to-late stages of the disease, the options are medication and surgery, respectively, but your doctor will advise about those in that eventuality.
In the early stages of the disease, the first-line recommend treatment is exercise, of which, especially walking:
Lower Extremity Peripheral Artery Disease: Diagnosis and Treatment
Given that this more often happens when someone hasn’t been walking so much, it can be a walk-rest-walk approach at first (a treadmill on a low setting can be very useful for this):
See also: Exercise Comparison Head-to-Head: Treadmill vs Road
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Burned Out By Tuesday?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Avoiding Burnout, The Active Way

This is Dr. Claudine Holt. She’s double board-certified, in Occupational & Environmental Medicine, and Lifestyle Medicine.
In short: preventative medicine in all parts of our life.
Hopefully, you are reading this bright-eyed and bushy-tailed and ready to take on another exciting day in this wonderful, beautiful world!
On the other hand, it’s possible that you’re reading this semi-focussed, looking for a crumb of dopamine as much as you are looking for information.
If you’ve ever had the “What a week!” / “It’s only Tuesday” moment, this one’s for you.
What does Dr. Holt want us to know?
You can recover from burnout without guilt
Sometimes, we overreach ourselves. Sometimes, life overreaches us! Sometimes it’s not that we overcommitted—it’s just that we were taking each day as it comes, but sometimes several days gang up on us at once.
Sometimes, even, we can feel exhausted when it seems like we haven’t done anything.
Note: if you feel exhausted and it seems like you haven’t done anything, then be aware: you are exhausted for a reason!
What that reason might be may vary, but contrary to popular belief, energy does not just vanish. It went somewhere.
This goes double if you have any chronic illness(es), even if you’re not aware of having had a flare-up, chances are you were just exceptionally busy (on a cellular level).
And it’s easy to think that “mere” cellular activity shouldn’t be exhausting, but that is 100% of where our energy transactions happen—whether or not we are consciously aware of them!
See also: Eat To Beat Chronic Fatigue ← yes, this also covers when you are too exhausted to shop and cook like a TV chef
Dr. Holt specializes in working with burned out medical professionals (and also specifically specializes in working with women), but there are lessons for everyone in her advice. For example:
Fiction: ”Medicine is my calling–it’s who I am.”
Fact: You are more than medicine! Remember that your career is just one aspect of your life. Don’t forget to create your big-picture vision and tend the garden of the other areas of your life too.
Read more: Dr. Claudine Holt | Burnout: Fact vs Fiction
This same thing can go for whatever part of your identity frequently follows “I’m a…”, and is somewhere that you put a lot of your energy; it could equally be a non-professional job like “homemaker”, or a relational status like “husband”, or a cultural identifier like “Christian”, or a hobby like “gardener” (assuming that is not also your profession, in which case, same item, different category).
Indeed, a lot of women especially get hit by “the triple burden” of professional work, housework, and childcare. And it’s not even necessarily that we resent any of those things or feel like they’re a burden; we (hopefully) love our professions, homes, children. But, here’s the thing:
No amount of love will add extra hours to the day.
So what does she recommend doing about it, when sometimes we’re juggling things that can’t be dropped?
Start simple, but start!
Dr. Holt recommends to start with a smile (yes even if, and sometimes especially when, the circumstances do not feel like they merit it), and deploy some CBT tools:
Two Hacks to Quickly Rise Above Burnout (Or Any Circumstance)
We’ve expanded on this topic here:
With a more level head on, it becomes easier to take on the next step, which creating healthy boundaries—and that doesn’t just mean with other people!
It also means slaying our own perfectionism and imposter syndrome—both things that will have us chasing our tails 36 hours per day if we let them.
See also:
- Perfectionism, And How To Make Yours Work For You
- Imposter Syndrome (And Why Almost Everyone Has It)
❝Burnout is the culture of our times. A culture that expects us to do more and think our way out of everything. A culture that asks for more than the body can bear. Unfortunately, even though the situation might not be of our creation, burnout culture is our inheritance.
An inheritance we can either perpetuate—or change—depending on what we embody.❞
Source: The Embodied MD on Burnout with Dr Claudine Holt
That “embodiment” is partly our choices and actions that we bring and own just as we bring and own our body—and it’s partly our relationship with our body itself, and learning to love it, and work with it to achieve wonderful things, instead of just getting through the day.
Which yes, does also mean making space for good diet, exercise, sleep and so forth, per:
These Top Five Things Make The Biggest Difference To Health
Want to know more?
You might like to check out Dr. Holt’s website:
The Embodied M.D. | Burnout Coach
…where she also offers resources such as a blog and a podcast.
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: