Is TikTok right? Can adding a teaspoon of cinnamon to your coffee help you burn fat?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cinnamon has been long used around the world in both sweet and savoury dishes and drinks.
But a new TikTok trend claims adding a teaspoon of cinnamon to your daily coffee (and some cocoa to make it more palatable) for one week can help you burn fat. Is there any truth to this?

Not all cinnamon is the same
There are two types of cinnamon, both of which come from grinding the bark of the cinnamomum tree and may include several naturally occurring active ingredients.
Cassia cinnamon is the most common type available in grocery stores. It has a bitter taste and contains higher levels of one of the active ingredient cinnamaldehyde, a compound that gives cinnamon its flavour and odour. About 95% of cassia cinnamon is cinnamaldehyde.
The other is Ceylon cinnamon, which tastes sweeter. It contains about 50-60% cinnamaldehyde.
Does cinnamon burn fat? What does the research say?
A review of 35 studies examined whether consuming cinnamon could affect waist circumference, which is linked to increased body fat levels. It found cinnamon doses below 1.5 grams per day (around half a teaspoon) decreased waist circumference by 1.68cm. However, consuming more than 1.5g/day did not have a significant effect.
A meta-analysis of 21 clinical trials with 1,480 total participants found cinnamon also reduced body mass index (BMI) by 0.40kg/m² and body weight by 0.92kg. But it did not change the participants’ composition of fat or lean mass.
Another umbrella review, which included all the meta-analyses, found a small effect of cinnamon on weight loss. Participants lost an average of 0.67kg and reduced their BMI by 0.45kg/m².

So overall, the weight loss we see from these high-quality studies is very small, ranging anywhere from two to six months and mostly with no change in body composition.
The studies included people with different diseases, and most were from the Middle East and/or the Indian subcontinent. So we can’t be certain we would see this effect in people with other health profiles and in other countries. They were also conducted over different lengths of time from two to six months.
The supplements were different, depending on the study. Some had the active ingredient extracted from cinnamon, others used cinnamon powder. Doses varied from 0.36g to 10g per day.
They also used the two different types of cinnamon – but none of the studies used cinnamon from the grocery store.
How could cinnamon result in small amounts of weight loss?
There are several possible mechanisms.
It appears to allow blood glucose (sugar) to enter the body’s cells more quickly. This lowers blood glucose levels and can make insulin work more effectively.
It also seems to improve the way we break down fat when we need it for energy.
Finally, it may make us feel fuller for longer by slowing down how quickly the food is released from our stomach into the small intestine.
What are the risks?
Cinnamon is generally regarded as safe when used as a spice in cooking and food.
However, in recent months the United States and Australia have issued health alerts about the level of lead and other heavy metals in some cinnamon preparations.
Lead enters as a contaminant during growth (from the environment) and in harvesting. In some cases, it has been suggested there may have been intentional contamination.
Some people can have side effects from cinnamon, including gastrointestinal pain and allergic reactions.
One of the active ingredients, coumarin, can be toxic for some people’s livers. This has prompted the European Food Authority to set a limit of 0.1mg/kg of body weight.
Cassia cinnamon contains up to 1% of coumarin, and the Ceylon variety contains much less, 0.004%. So for people weighing above 60kg, 2 teaspoons (6g) of cassia cinnamon would bring them over the safe limit.
What about the coffee and cocoa?
Many people may think coffee can also help us lose weight. However there isn’t good evidence to support this yet.
An observational study found drinking one cup of regular coffee was linked to a reduction in weight that is gained over four years, but by a very small amount: an average of 0.12kg.
Good-quality cocoa and dark chocolate have also been shown to reduce weight. But again, the weight loss was small (between 0.2 and 0.4kg) and only after consuming it for four to eight weeks.
So what does this all mean?
Using cinnamon may have a very small effect on weight, but it’s unlikely to deliver meaningful weight loss without other lifestyle adjustments.
We also need to remember these trials used products that differ from the cinnamon we buy in the shops. How we store and how long we keep cinnamon might also impact or degrade the active ingredients.
And consuming more isn’t going to provide additional benefit. In fact, it could increase your risk of side effects.
So if you enjoy the taste of cinnamon in your coffee, continue to add it, but given its strong taste, you’re likely to only want to add a little.
And no matter how much we’d like this to be true, we certainly won’t gain any fat-loss benefits by consuming cinnamon on doughnuts or in buns, due to their high kilojoule count.
If you want to lose weight, there are evidence-backed approaches that won’t spoil your morning coffee.
Evangeline Mantzioris, Program Director of Nutrition and Food Sciences, Accredited Practising Dietitian, University of South Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Chemically Imbalanced – by Dr. Joanna Moncrieff

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The author, a professor of psychiatry, challenges the prevailing consensus that depression is often caused by a neurotransmitter imbalance, and as such, she further challenges the most popularly-prescribed class of antidepressants, SSRIs (selective serotonin reuptake inhibitors, whose job is do what it says on the tin, with the end goal of your brain having more serotonin in it because you’re keeping the serotonin you do make for longer).
Her position is that depression is only caused by—and can only be fixed by—external factors, and that any benefit from antidepressants is placebo (in contrast, at 10almonds we wrote a while back about the more widely-accepted explanation of the hit-and-miss nature of whether antidepressants help someone is that often people are simply taking the wrong class of antidepressants for their specific depression; see: Antidepressants: Personalization Is Key!).
She asserts that depression is not even a real medical condition, and is simply a social phenomenon, and she hopes that one day her colleagues in the profession will agree.
It’s worth noting that a more moderate version of the first part of her assertions (that personal life conditions are often a major causal factor) is a common view by prescribers in the author’s native UK, where doctors have coined a colorful name for this condition. However, SSRIs are usually still the first recourse, on a “try it and see” basis.
Dr. Moncrieff devotes several chapters to the unwanted side effects that can be experienced, and considers the incidence of such to be important enough—and persistent enough, sometimes lasting for a while after discontinuation—to be a violation of the “first, do no harm” principle.
The style is… confident, let’s say. The author accepts that there are a plurality of views—hers, and the wrong ones held by most people in her profession. She also encourages us as readers to make our own decisions—avoid antidepressants (and, in fact, psychiatric meds of any kind, especially antipsychotics for people experiencing psychosis), or destroy our health; it’s up to us. She recognizes that very many people believe antidepressants have changed their lives for the better—and she considers those now-happier people to be fools duped by Big Pharma.
Bottom line: on the one hand, this looks a lot like 288 pages of the author’s firmly-held confirmation bias; on the other hand, that doesn’t change the fact that it is worth at the very least considering, before embarking on a course of treatment, “why are we assuming that the issue is serotonin specifically?”, because (per the prevailing scientific consensus) sometimes it is, sometimes it isn’t.
Click here to check out Chemically Imbalanced, and consider the options!
Share This Post
-

A Statin-Free Life – by Dr. Aseem Malhotra
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Here at 10almonds, we’ve written before about the complexities of statins, and their different levels of risk/benefit for men and women, respectively. It’s a fascinating topic, and merits more than an article of the size we write here!
So, in the spirit of giving pointers of where to find a lot more information, this book is a fine choice.
Dr. Malhotra, a consultant cardiologist and professor of evidence-based medicine, talks genes and lifestyle, drugs and blood. He takes us on a tour of the very many risk factors for heart disease, and how cholesterol levels may be at best an indicator, but less likely a cause, of heart disease, especially for women. Further and even better, he discusses various more reliable indicators and potential causes, too.
Rather than be all doom and gloom, he does offer guidance on how to reduce each of one’s personal risk factors and—which is important—keep on top of the various relevant measures of heart health (including some less commonly tested ones, like the coronary calcium score).
The style is light reading andyet with a lot of reference to hard science, so it’s really the best of both worlds in that regard.
Bottom line: if you’re considering statins, or are on statins and are reconsidering that choice, then this book will (notwithstanding its own bias in its conclusion) help you make a more-informed decision.
Click here to check out A Statin-Free Life, and make the best choice for you!
Share This Post
-

How To Make Your Doctor’s Appointment Do More For You
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Doctor: “So, how are you today?”
Patient: “Can’t complain; how about you?”Hopefully your medical appointments don’t start quite like that, but there can be an element of being “along for the ride” when it comes to consultations. They ask questions, we answer, they prescribe something, we thank them.
In principle, the doctor should be able to handle that; ask the right questions, determine the problem, and not need too much from you. After all, they have been trained to deal with an unconscious patient, so the fact you can communicate at all is a bonus.
However, leaving it all to them isn’t really playing the field.
Before the appointment
Research your issue, as best you understand it. Some doctors will be very averse to you telling them about having done this (taking it as an affront to their expertise), but here’s the thing:
You don’t have to tell them.
You just have to understand as much as possible, so that you will be as “up to speed” as possible in the conversation, and not be quickly out of your depth.
Have an agenda, based on the above. Literally, have a little set of bullet-points to remind you what you came in to discuss, so that nothing escapes you in the moment. This should also include:
- If you have additional reasons for a particular concern (e.g. family history of a certain problem), make them known
- If you plan to request any specific tests or treatments, be able to clearly state your reasons for the specific tests or treatments
- If you plan to write off any specific tests or treatments as something to which you will not consent, have your reasons ready—in a way that makes it clear it’s something more than “don’t want it”, for example, “I’ve already decided that this treatment would make a sufficient hit to my quality of life, as to make it not worthwhile for me personally” (or whatever the reason may be for you). It needs to be something they can write on their notes instead of simply “patient refused treatment”.
Compile a record of your symptoms (as appropriate), and any previous tests/treatments (as appropriate), in chronological order. If you take all this with you, perhaps in a nice folder, you will enjoy the following advantages:
- not forgetting anything
- ability to answer questions accurately
- give the (correct) impression you take your health seriously, which means they are more likely to do so also—especially because they will now know that if they fob you off and/or mess something up, you’ll be taking a record of that to your next appointment.
Plan your outfit. No, you don’t have to dress for the red carpet, but you want to satisfy two main conditions:
- Accessibility for examination (for example, if you are going in with a knee pain, maybe don’t wear the tight jeans today; if they’re going to take blood, be either sleeveless or have sleeves that are easily moved out of the way, etc)
- General presentability (it’s a sad fact that doctors are not immune to biases, and will treat people better if they respect them more)
During the appointment
Be friendly; doctors (like most people) will respond much better to that than to grumpiness—even if you have good reason for grumpiness and even if the doctor has been trained to help grumpy patients.
Be confident: when we say “be friendly”, that doesn’t mean to necessarily be so agreeable as to not advocate for yourself. In particular:
- If they explain something and it isn’t clear to you, ask them to clarify
- If you disagree with them about a value judgement, say so. By “a value judgement” here we mean things in the realm of subjectivity. If the doctor says you are prediabetic, then you won’t get much mileage out of arguing otherwise; the numbers have the final say on that one. But if the doctor says “the side effects of the treatment you’re requesting will make it not worthwhile for you” and you have understood the side effects and you still disagree, then your opinion counts for more than theirs—it is your decision to make.
- If they dismiss a concern, ask them to put in writing that they dismissed your concern of X, despite you providing evidence that Y, and it being well-known that Z. Often, rather than doing that, they’ll just fold and actually address your concern instead.
Writer’s example in that last category: I recently made a request for a bone density scan. I expect my bone density is great, because I do all the right things, however, as both of my parents suffered from osteoporosis and assorted resultant crushed bones and the terrible consequences thereof, I a) have reasonable grounds for extra concern, and b) I believe that even if my bone density is fine now, it’s good to establish a baseline so I can know, in 5, 10, 20 years etc, whether there has been any deterioration. Now, happily the doctor I saw agreed with my assessment at first presentation and so I got the referral, but had she not been, I would have said “Could you please put in writing that I asked for a bone density scan, and you refused, on the grounds that [details about what happened with my parents], and that osteoporosis is known to have a strong genetic component is not, in your opinion, any reason to worry?”
Be honest, and/but err on the side of overstating your symptoms rather than understating. For example, if it is about a chronic condition and the doctor asks “are you able to do xyz”, take the question as meaning “are you able to do xyz on your worst days?”. You can clarify that if you like in your answer, but you need to include the information that xyz is something that your condition can and sometimes does impede you from doing.
Leave your embarrassment at the door. To the doctor (unless they are a very unprofessional one), you really are just one more patient with symptoms they have (unless your condition is very rare) seen a thousand times before. If your symptom is embarrassing, it will not faze them and you definitely should not hold back from mentioning it, for example. This goes extra in the case of discussions around sexual health, by the way, in which field the details you’d perhaps rather not share with anybody, are the details they need to adequately treat you.
After the appointment
Follow up on anything that doesn’t happen as promised (e.g. referrals, things ordered, etc), to make sure nothing got lost in a bureacratic error.
Get a second opinion if you’re not satisfied with the first one. Doctors are fallible, and as a matter of professional pride, it’s likely the second doctor will be glad to find something the first doctor missed.
See also: Make Your Negativity Work For You
Take care!
Share This Post

-

The Fascinating Truth About Aspartame, Cancer, & Neurotoxicity
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Is Aspartame’s Reputation Well-Deserved?

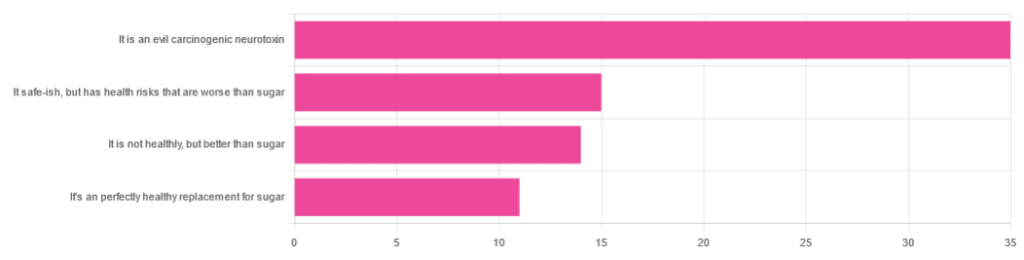
In Tuesday’s newsletter, we asked you for your health-related opinions on aspartame, and got the above-depicted, below-described, set of responses:
- About 47% said “It is an evil carcinogenic neurotoxin”
- 20% said “It is safe-ish, but has health risks that are worse than sugar”
- About 19% said “It is not healthy, but better than sugar”
- About 15% said “It’s a perfectly healthy replacement for sugar”
But what does the science say?
Aspartame is carcinogenic: True or False?
False, assuming consuming it in moderation. In excess, almost anything can cause cancer (oxygen is a fine example). But for all meaningful purposes, aspartame does not appear to be carcinogenic. For example,
❝The results of these studies showed no evidence that these sweeteners cause cancer or other harms in people.❞
~ NIH | National Cancer Institute
Source: Artificial Sweeteners and Cancer
Plenty of studies and reviews have also confirmed this; here are some examples:
- Evaluation of aspartame cancer epidemiology studies based on quality appraisal criteria
- Aspartame, low-calorie sweeteners and disease: Regulatory safety and epidemiological issues
- Aspartame: A review of genotoxicity data
Why then do so many people believe it causes cancer, despite all the evidence against it?
Well, there was a small study involving giving megadoses to rats, which did increase their cancer risk. So of course, the popular press took that and ran with it.
But those results have not been achieved outside of rats, and human studies great and small have all been overwhelmingly conclusive that moderate consumption of aspartame has no effect on cancer risk.
Aspartame is a neurotoxin: True or False?
False, again assuming moderate consumption. If you’re a rat being injected with a megadose, your experience may vary. But a human enjoying a diet soda, the aspartame isn’t the part that’s doing you harm, so far as we know.
For example, the European Food Safety Agency’s scientific review panel concluded:
❝there is still no substantive evidence that aspartame can induce such effects❞
~ Dr. Atkin et al (it was a pan-European team of 21 experts in the field)
Source: Report on the Meeting on Aspartame with National Experts
See also,
❝The data from the extensive investigations into the possibility of neurotoxic effects of aspartame, in general, do not support the hypothesis that aspartame in the human diet will affect nervous system function, learning or behavior.
The weight of existing evidence is that aspartame is safe at current levels of consumption as a nonnutritive sweetener.❞
and
❝The safety testing of aspartame has gone well beyond that required to evaluate the safety of a food additive.
When all the research on aspartame, including evaluations in both the premarketing and postmarketing periods, is examined as a whole, it is clear that aspartame is safe, and there are no unresolved questions regarding its safety under conditions of intended use.❞
Source: Regulatory Toxicology & Pharmacology | Aspartame: Review of Safety
Why then do many people believe it is a neurotoxin? This one can be traced back to a chain letter hoax from about 26 years ago; you can read it here, but please be aware it is an entirely debunked hoax:
Urban Legends | Aspartame Hoax
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Winter Wellness & The Pills That Increase Your Alzheimer’s Risk
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This week in health news…
Do not go gentle into that good night
As wildfires rage in California, snow is falling from Texas to Georgia, meaning that a lot of people are facing weather they’re not accustomed to, in houses that were not built for it. And that’s the lucky ones; there are many thousands of people who are homeless, of whom many will die.
Hopefully all our readers are safe, but it pays to watch out for the signs of hypothermia as it is a condition that really sneaks up on people and, in the process, takes away their ability to notice the hypothermia. You and your loved ones are not immune to this, so it’s good to keep an eye on each other, looking out for:
- Shivering, first ← when this stops, assuming it’s not because the temperature has risen, it is often a sign of hypothermia entering a later stage, in which the body is no longer responding appropriately to the cold
- Slurred speech or mumbling
- Slow, shallow breathing
- A weak pulse
- Clumsiness or lack of coordination
- Drowsiness or very low energy
- Confusion or memory loss
- Loss of consciousness
- In infants, bright red, cold skin
How cold is too cold? It doesn’t even have to be sub-zero. According to the CDC, temperatures of 4℃ (40℉) can be low enough to cause hypothermia.
Read in full: The warning signs to notice if someone has hypothermia
Related: Cold Weather Health Risks
Lethal lottery of pathogens
In Minnesota, hospital emergency room waiting times have skyrocketed since yesterday (at time of writing), with 40% of Minnesota’s 1,763 flu-related hospitalizations this fall and winter occurring in the same week, according to yesterday’s report. To put it further into perspective, 17 out of 20 of this season’s flu outbreaks have occurred in the past two weeks.
And that’s just the flu, without considering COVID, RSV, and Norovirus, which are also all running rampant in MN right now.
The advice presently is:
❝Go to the ER if you are super-sick. If you are not super-sick, go to urgent care, go to your clinic, schedule a virtual appointment.❞
And if you’re not in Minneapolis? These stats won’t apply, but definitely consider, before going to the hospital, whether you might leave sicker than you arrived, and plan accordingly, making use of telehealth where reasonably possible.
Read in full: Minnesota ERs stressed by “quad-demic” of COVID, flu, RSV, norovirus
Related: Move over, COVID and Flu! We Have “Hybrid Viruses” To Contend With Now
Sleep, but at what cost?
This was a study looking at the effects of sleeping pills on the brain, specifically zolpidem (most well-known by its brand name of Ambien).
What they found is that while it does indeed effectively induce sleep, part of how it does that is suppressing norepinephrine oscillations (which might otherwise potentially wake you up, though in healthy people these oscillations and the micro-arousals that they cause shouldn’t disrupt sleep at all, and are just considered part of our normal sleep cycles), which oscillations are necessary to generate the pumping action required to move cerebrospinal fluid through the glymphatic system while asleep.
This is a big problem, because the glymphatic system is almost entirely responsible for keeping the brain free from waste products such as beta-amyloids (whose build-up is associated with Alzheimer’s disease and is considered to be a significant part of Alzheimer’s pathogensesis) and alpha-synuclein (same but for Parkinson’s disease), amongst others:
Read in full: Common sleeping pill may pave way for disorders like Alzheimer’s
Related: How To Clean Your Brain (Glymphatic Health Primer)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What is Ryeqo, the recently approved medicine for endometriosis?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
For women diagnosed with endometriosis it is often a long sentence of chronic pain and cramping that impacts their daily life. It is a condition that is both difficult to diagnose and treat, with many women needing either surgery or regular medication.
A medicine called Ryeqo has just been approved for marketing specifically for endometriosis, although it was already available in Australia to treat a different condition.
Women who want the drug will need to consult their local doctor and, as it is not yet on the Pharmaceutical Benefits Scheme, they will need to pay the full cost of the script.
What does Ryeqo do?
Endometriosis affects 14% of women of reproductive age. While we don’t have a full understanding of the cause, the evidence suggests it’s due to body tissue that is similar to the lining of the uterus (called the endometrium) growing outside the uterus. This causes pain and inflammation, which reduces quality of life and can also affect fertility.
Ryeqo is a tablet containing three different active ingredients: relugolix, estradiol and norethisterone.
Relugolix is a drug that blocks a particular peptide from releasing other hormones. It is also used in the treatment of prostate cancer. Estradiol is a naturally occurring oestrogen hormone in women that helps regulate the menstrual cycle and is used in menopausal hormone therapy. Norethisterone is a synthetic hormone commonly used in birth control medications and to delay menstruation and help with heavy menstrual bleeding.
All three components work together to regulate the levels of oestrogen and progesterone in the body that contribute to endometriosis, alleviating its symptoms.
Relugolix reduces the overall levels of oestrogen and progesterone in the body. The estradiol compensates for the loss of oestrogen because low oestrogen levels can cause hot flushes (also called hot flashes) and bone density loss. And norethisterone blocks the effects of estradiol on the uterus (where too much tissue growth is unwanted).
Is it really new?
The maker of Ryeqo claims it is the first new drug for endometriosis in Australia in 13 years.
But individually, all three active ingredients in Ryeqo have been in use since 2019 or earlier.
Ryeqo has been available in Australia since 2022, but until now was not specifically indicated for endometriosis. It was originally approved for the treatment of uterine fibroids, which share some common symptoms with endometriosis and have related causes.
In addition to Ryeqo, current medical guidance lists other drugs that are suitable for endometriosis and some reformulations of these have also only been recently approved.
The oral medicine Dienogest was approved in 2021, and there have been a number of injectable drugs for endometriosis recently approved, such as Sayana Press which was approved in a smaller dose form for self-injection in 2023.

You can’t take the contraceptive pill with Ryeqo but the endometriosis drug could replace it.
ShutterstockHow to take it and what not to do
Ryeqo is a once-a-day tablet. You can take it with, or without food, but it should be taken about the same time each day.
It is recommended you start taking Ryeqo within the first five days after the start of your next period. If you start at another time during your period, you may experience initial irregular or heavier bleeding.
Because it contains both synthetic and natural hormones, you can’t use the contraceptive pill and Ryeqo together. However, because Ryeqo does contain norethisterone it can be used as your contraception, although it will take at least one month of use to be effective. So, if you are on Ryeqo, you should use a non-hormonal contraceptive – such as condoms – for a month when starting the medicine.
Ryeqo may be incompatible with other medicines. It might not be suitable for you if you take medicines for epilepsy, HIV and AIDS, hepatitis C, fungal or bacterial infections, high blood pressure, irregular heartbeat, angina (chest pain), or organ rejection. You should also not take Ryeqo if you have a liver tumour or liver disease.
The possible side effects of Ryeqo are similar to those of oral contraceptives. Blood clots are a risk with any medicine that contains an oestrogen or a progestogen, which Ryeqo does. Other potential side effects include bone loss, a reduction in menstrual blood loss or loss of your period.
It’s costly for now
Ryeqo can now be prescribed in Australia, so you should discuss whether Ryeqo is right for you with the doctor you usually consult for your endometriosis.
While the maker has made a submission to the Pharmaceutical Benefits Advisory Committee, it is not yet subsidised by the Australian government. This means that rather than paying the normal PBS price of up to A$31.60, it has been reported it may cost as much as $135 for a one-month supply. The committee will make a decision on whether to subsidise Ryeqo at its meeting next month.
Correction: this article has been updated to clarify the recent approval of specific formulations of drugs for endometriosis.

Nial Wheate, Associate Professor of the School of Pharmacy, University of Sydney and Jasmine Lee, Pharmacist and PhD Candidate, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: