The Best Exercise to Stop Your Legs From Giving Out
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Doug Weiss, seniors-specialist physio, has an exercise that stops your knees from being tricked into collapsing (which is very common) by a misfiring (also common) reflex.
Step up…
Setup to step up thus:
- Use a sturdy support like a countertop or chair.
- Have an aerobic step or similar firm surface to step onto.
When you’re ready:
- Stand facing away from the step.
- Place one hand on the support for stability.
- Step backwards up onto the step with your right leg, then your left leg, so both feet are on the step.
- Step forward to come back down.
Once you’re confident of the series of movements, do it without the support, and do it for a few minutes each day. Don’t worry about how easy it becomes; this is not, first and foremost, a strength-training exercise; you don’t have to start adding weights or anything (although of course you can if you want).
How it works: there’s a part of you called the Golgi tendon organ, and it can trigger a Golgi tendon reflex, which is one of the body’s equivalents of a steam valve. However, instead of letting off steam to avoid a boiler explosion, it collapses a joint to save it from overload. However, if not exercised regularly, it can get overly sensitive, causing it to mistake your mere bodyweight for an overload. So, it collapses, thinking it is saving you from snapping a tendon, but it’s not. By exercising in the way described, the Golgi tendon reflex will go back to only being triggered by an actual overload, not the mere act of stepping.
Writer’s note: this one’s interesting to me as I have a) a strong lower body b) hypermobile joints that thus occasionally just fold like laundry regardless. Could it be that this will fix that? I guess I’ll find out 🙂
Meanwhile, for more on all of the above plus a visual demonstration, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
What Nobody Teaches You About Strengthening Your Knees
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What will aged care look like for the next generation? More of the same but higher out-of-pocket costs

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Aged care financing is a vexed problem for the Australian government. It is already underfunded for the quality the community expects, and costs will increase dramatically. There are also significant concerns about the complexity of the system.
In 2021–22 the federal government spent A$25 billion on aged services for around 1.2 million people aged 65 and over. Around 60% went to residential care (190,000 people) and one-third to home care (one million people).
The final report from the government’s Aged Care Taskforce, which has been reviewing funding options, estimates the number of people who will need services is likely to grow to more than two million over the next 20 years. Costs are therefore likely to more than double.
The taskforce has considered what aged care services are reasonable and necessary and made recommendations to the government about how they can be paid for. This includes getting aged care users to pay for more of their care.
But rather than recommending an alternative financing arrangement that will safeguard Australians’ aged care services into the future, the taskforce largely recommends tidying up existing arrangements and keeping the status quo.
No Medicare-style levy
The taskforce rejected the aged care royal commission’s recommendation to introduce a levy to meet aged care cost increases. A 1% levy, similar to the Medicare levy, could have raised around $8 billion a year.
The taskforce failed to consider the mix of taxation, personal contributions and social insurance which are commonly used to fund aged care systems internationally. The Japanese system, for example, is financed by long-term insurance paid by those aged 40 and over, plus general taxation and a small copayment.
Instead, the taskforce puts forward a simple, pragmatic argument that older people are becoming wealthier through superannuation, there is a cost of living crisis for younger people and therefore older people should be required to pay more of their aged care costs.
Separating care from other services
In deciding what older people should pay more for, the taskforce divided services into care, everyday living and accommodation.
The taskforce thought the most important services were clinical services (including nursing and allied health) and these should be the main responsibility of government funding. Personal care, including showering and dressing were seen as a middle tier that is likely to attract some co-payment, despite these services often being necessary to maintain independence.
The task force recommended the costs for everyday living (such as food and utilities) and accommodation expenses (such as rent) should increasingly be a personal responsibility.

Aged care users will pay more of their share for cooking and cleaning.
Lizelle Lotter/ShutterstockMaking the system fairer
The taskforce thought it was unfair people in residential care were making substantial contributions for their everyday living expenses (about 25%) and those receiving home care weren’t (about 5%). This is, in part, because home care has always had a muddled set of rules about user co-payments.
But the taskforce provided no analysis of accommodation costs (such as utilities and maintenance) people meet at home compared with residential care.
To address the inefficiencies of upfront daily fees for packages, the taskforce recommends means testing co-payments for home care packages and basing them on the actual level of service users receive for everyday support (for food, cleaning, and so on) and to a lesser extent for support to maintain independence.
It is unclear whether clinical and personal care costs and user contributions will be treated the same for residential and home care.
Making residential aged care sustainable
The taskforce was concerned residential care operators were losing $4 per resident day on “hotel” (accommodation services) and everyday living costs.
The taskforce recommends means tested user contributions for room services and everyday living costs be increased.
It also recommends that wealthier older people be given more choice by allowing them to pay more (per resident day) for better amenities. This would allow providers to fully meet the cost of these services.
Effectively, this means daily living charges for residents are too low and inflexible and that fees would go up, although the taskforce was clear that low-income residents should be protected.
Moving from buying to renting rooms
Currently older people who need residential care have a choice of making a refundable up-front payment for their room or to pay rent to offset the loans providers take out to build facilities. Providers raise capital to build aged care facilities through equity or loan financing.
However, the taskforce did not consider the overall efficiency of the private capital market for financing aged care or alternative solutions.
Instead, it recommended capital contributions be streamlined and simplified by phasing out up-front payments and focusing on rental contributions. This echoes the royal commission, which found rent to be a more efficient and less risky method of financing capital for aged care in private capital markets.
It’s likely that in a decade or so, once the new home care arrangements are in place, there will be proportionally fewer older people in residential aged care. Those who do go are likely to be more disabled and have greater care needs. And those with more money will pay more for their accommodation and everyday living arrangements. But they may have more choice too.
Although the federal government has ruled out an aged care levy and changes to assets test on the family home, it has yet to respond to the majority of the recommendations. But given the aged care minister chaired the taskforce, it’s likely to provide a good indication of current thinking.

Hal Swerissen, Emeritus Professor, La Trobe University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Get Better Sleep: Beyond “Sleep Hygiene”
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Better Sleep, Better Life!

This is Arianna Huffington. Yes, that Huffington, of the Huffington Post. But! She’s also the CEO of Thrive Global, a behavior change tech company with the mission of changing the way we work and live—in particular, by challenging the idea that burnout is the required price of success.
The power of better sleep
Sleep is a very important, but most often neglected, part of good health. Here are some of Huffington’s top insights from her tech company Thrive, and as per her “Sleep Revolution” initiative.
Follow your circadian rhythm
Are you a night owl or a morning lark? Whichever it is, roll with it, and plan around that if your lifestyle allows for such. While it is possible to change from one to the other, we do have a predisposition towards one or the other, and will generally function best when not fighting it.
This came about, by the way, because we evolved to have half of us awake in the mornings and half in the evenings, to keep us all safe. Socially we’ve marched onwards from that point in evolutionary history, but our bodies are about a hundred generations behind the times, and that’s just what we have to work with!
Don’t be afraid (or ashamed!) to take naps
Naps, done right, can be very good for the health—especially if we had a bad night’s sleep the previous night.
Thrive found that workers are more productive when they have nap rooms, and (following on a little from the previous point) are allowed to sleep in or work from home.
See also: How To Nap Like A Pro (No More “Sleep Hangovers”!)
Make sure you have personal space available in bed
The correlation between relationship satisfaction and sleeping close to one’s partner has been found to be so high that it’s even proportional: the further away a couple sleeps from each other, the less happy they are. But…
Partners who got good sleep the previous night, will be more likely to want intimacy on any given night—at a rate of an extra 14% per extra hour of sleep the previous night. So, there’s a trade-off, as having more room in bed tends to result in better sleep. Time to get a bigger bed?
What gets measured, gets done
This goes for sleep, too! Not only does dream-journaling in the morning cue your subconscious to prepare to dream well the following night, but also, sleep trackers and sleep monitoring apps go a very long way to improving sleep quality, even if no extra steps are consciously taken to “score better”.
We’ve previously reviewed some of the most popular sleep apps; you can check out for yourself how they measured up:
Share This Post
-
Shame and blame can create barriers to vaccination
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Understanding the stigma surrounding infectious diseases like HIV and mpox may help community health workers break down barriers that hinder access to care.
Looking back in history can provide valuable lessons to confront stigma in health care today, especially toward Black, Latine, LGBTQ+, and other historically underserved communities disproportionately affected by COVID-19 and HIV.
Public Good News spoke with Sam Brown, HIV prevention and wellness program manager at Civic Heart, a community-based organization in Houston’s historic Third Ward, to understand the effects of stigma around sexual health and vaccine uptake.
Brown shared more about Civic Heart’s efforts to provide free confidential testing for sexually transmitted infections, counseling and referrals, and information about COVID-19, flu, and mpox vaccinations, as well as the lessons they’re learning as they strive for vaccine equity.
Here’s what Brown said.
[Editor’s note: This content has been edited for clarity and length.]
PGN: Some people on social media have spread the myth that vaccines cause AIDS or other immune deficiencies when the opposite is true: Vaccines strengthen our immune systems to help protect against disease. Despite being frequently debunked, how do false claims like these impact the communities you serve?
Sam Brown: Misinformation like that is so hard to combat. And it makes the work and the path to overall community health hard because people will believe it. In the work that we do, 80 percent of it is changing people’s perspective on something they thought they knew.
You know, people don’t even transmit AIDS. People transmit HIV. So, a vaccine causing immunodeficiency doesn’t make sense.
With the communities we serve, we might have a person that will believe the myth, and because they believe it, they won’t get vaccinated. Then later, they may test positive for COVID-19.
And depending on social determinants of health, it can impact them in a whole heap of ways: That person is now missing work, they’re not able to provide for their family—if they have a family. It’s this mindset that can impact a person’s life, their income, their ability to function.
So, to not take advantage of something like a vaccine that’s affordable, or free for the most part, just because of misinformation or a misunderstanding—that’s detrimental, you know.
For example, when we talk to people in the community, many don’t know that they can get mpox from their pet, or that it’s zoonotic—that means that it can be transferred between different species or different beings, from animals to people. I see a lot of surprise and shock [when people learn this].
It’s difficult because we have to fight the misinformation and the stigma that comes with it. And it can be a big barrier.
People misunderstand. [They] think that “this is something that gay people or the LGBTQ+ community get,” which is stigmatizing and comes off as blaming. And blaming is the thing that leads us to be misinformed.
PGN: In the last couple years, your organization’s HIV Wellness program has taken on promoting COVID-19, flu, and mpox vaccines to the communities you serve. How do you navigate conversations between sexual health and infectious diseases? Can you share more about your messaging strategies?
S.B.: As we promoted positive sexual health and HIV prevention, we saw people were tired of hearing about HIV. They were tired of hearing about how PrEP works, or how to prevent HIV.
But, when we had an outbreak of syphilis in Houston just last year, people were more inclined to test because of the severity of the outbreak.
So, what our team learned is that sometimes you have to change the message to get people what they need.
We changed our message to highlight more syphilis information and saw that we were able to get more people tested for HIV because we correlated how syphilis and HIV are connected and how a person can be susceptible to both.
Using messages that the community wants and pairing them with what the community needs has been better for us. And we see that same thing with COVID-19, the flu, and RSV. Sometimes you just can’t be married to a message. We’ve had to be flexible to meet our clients where they are to help them move from unsafe practices to practices that are healthy and good for them and their communities.
PGN: You’ve mentioned how hard it is to combat stigma in your work. How do you effectively address it when talking to people one-on-one?
S.B.: What I understand is that no one wants to feel shame. What I see people respond to is, “Here’s an opportunity to do something different. Maybe there was information that you didn’t know that caused you to make a bad decision. And now here’s an opportunity to gain information so that you can make a better decision.”
People want to do what they want to do; they want to live how they want to live. And we all should be able to do that as long as it’s not hurting anyone, but also being responsible enough to understand that, you know, COVID-19 is here.
So, instead of shaming and blaming, it’s best to make yourself aware and understand what it is and how to treat it. Because the real enemy is the virus—it’s the infection, not the people.
When we do our work, we want to make sure that we come from a strengths-based approach. We always look at what a client can do, what that client has. We want to make sure that we’re empowering them from that point. So, even if they choose not to prioritize our message right now, we can’t take that personally. We’ll just use it as a chance to try a new way of framing it to help people understand what we’re trying to say.
And sometimes that can be difficult, even for organizations. But getting past that difficulty comes with a greater opportunity to impact someone else.
This article first appeared on Public Good News and is republished here under a Creative Commons license.
Share This Post



Related Posts
-

From Dr. Oz to Heart Valves: A Tiny Device Charted a Contentious Path Through the FDA
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In 2013, the FDA approved an implantable device to treat leaky heart valves. Among its inventors was Mehmet Oz, the former television personality and former U.S. Senate candidate widely known as “Dr. Oz.”
In online videos, Oz has called the process that brought the MitraClip device to market an example of American medicine firing “on all cylinders,” and he has compared it to “landing a man on the moon.”
MitraClip was designed to spare patients from open-heart surgery by snaking hardware into the heart through a major vein. Its manufacturer, Abbott, said it offered new hope for people severely ill with a condition called mitral regurgitation and too frail to undergo surgery.
“It changed the face of cardiac medicine,” Oz said in a video.
But since MitraClip won FDA approval, versions of the device have been the subject of thousands of reports to the agency about malfunctions or patient injuries, as well as more than 1,100 reports of patient deaths, FDA records show. Products in the MitraClip line have been the subject of three recalls. A former employee has alleged in a federal lawsuit that Abbott promoted the device through illegal inducements to doctors and hospitals. The case is pending, and Abbott has denied illegally marketing the device.
The MitraClip story is, in many ways, a cautionary tale about the science, business, and regulation of medical devices.
Manufacturer-sponsored research on the device has long been questioned. In 2013, an outside adviser to the FDA compared some of the data marshaled in support of its approval to “poop.”
The FDA expanded its approval of MitraClip to a wider set of patients in 2019, based on a clinical trial in which Abbott was deeply involved and despite conflicting findings from another study.
In the three recalls, the first of which warned of potentially deadly consequences, neither the manufacturer nor the FDA withdrew inventory from the market. The company told doctors it was OK for them to continue using the recalled products.
In response to questions for this article, both Abbott and the FDA described MitraClip as safe and effective.
“With MitraClip, we’re addressing the needs of people with MR who often have no other options,” Abbott spokesperson Brent Tippen said. “Patients suffering from mitral regurgitation have severely limited quality of life. MitraClip can significantly improve survival, freedom for hospitalization and quality of life via a minimally invasive, now common procedure.”
An FDA spokesperson, Audra Harrison, said patient safety “is the FDA’s highest priority and at the forefront of our work in medical device regulation.”
She said reports to the FDA about malfunctions, injuries, and deaths that the device may have caused or contributed to are “consistent” with study results the FDA reviewed for its 2013 and 2019 approvals.
In other words: They were expected.
Inspiration in Italy
When a person has mitral regurgitation, blood flows backward through the mitral valve. Severe cases can lead to heart failure.
With MitraClip, flaps of the valve — known as “leaflets” — are clipped together at one or more points to achieve a tighter seal when they close. The clips are deployed via a catheter threaded through a major vein, typically from an incision in the groin. The procedure offers an alternative to connecting the patient to a heart-lung machine and repairing or replacing the mitral valve in open-heart surgery.
Oz has said in online videos that he got the idea after hearing a doctor describe a surgical technique for the mitral valve at a conference in Italy. “And on the way home that night, on a plane heading back to Columbia University, where I was on the faculty, I wrote the patent,” he told KFF Health News.
A patent obtained by Columbia in 2001, one of several associated with MitraClip, lists Oz first among the inventors.
But a Silicon Valley-based startup, Evalve, would develop the device. Evalve was later acquired by Abbott for about $400 million.
“I think the engineers and people at Evalve always cringe a little bit when they see Mehmet taking a lot of, you know, basically claiming responsibility for what was a really extraordinary team effort, and he was a small to almost no player in that team,” one of the company’s founders, cardiologist Fred St. Goar, told KFF Health News.
Oz did not respond to a request for comment on that statement.
As of 2019, the MitraClip device cost $30,000 per procedure, according to an article in a medical journal. According to the Abbott website, more than 200,000 people around the world have been treated with MitraClip.
Oz filed a financial disclosure during his unsuccessful run for the U.S. Senate in 2022 that showed him receiving hundreds of thousands of dollars in annual MitraClip royalties.
Abbott recently received FDA approval for TriClip, a variation of the MitraClip system for the heart’s tricuspid valve.
Endorsed ‘With Trepidation’
Before the FDA said yes to MitraClip in 2013, agency staffers pushed back.
Abbott had originally wanted the device approved for “patients with significant mitral regurgitation,” a relatively broad term. After the FDA objected, the company narrowed its proposal to patients at too-high risk for open-heart surgery.
Even then, in an analysis, the FDA identified “fundamental” flaws in Abbott’s data.
One example: The data compared MitraClip patients with patients who underwent open-heart surgery for valve repair — but the comparison might have been biased by differences in the expertise of doctors treating the two groups, the FDA analysis said. While MitraClip was implanted by a highly select, experienced group of interventional cardiologists, many of the doctors doing the open-heart surgeries had performed only a “very low volume” of such operations.
FDA “approval is not appropriate at this time as major questions of safety and effectiveness, as well as the overall benefit-risk profile for this device, remain unanswered,” the FDA said in a review prepared for a March 2013 meeting of a committee of outside advisers to the agency.
Some committee members expressed misgivings. “If your right shoe goes into horse poop and your left shoe goes into dog poop, it’s still poop,” cardiothoracic surgeon Craig Selzman said, according to a transcript.
The committee voted 5-4 against MitraClip on the question of whether it proved effective. But members voted 8-0 that they considered the device safe and 5-3 that the benefits of the device outweighed its risks.
Selzman voted yes on the last question “with trepidation,” he said at the time.
In October 2013, the FDA approved the MitraClip Clip Delivery System for a narrower group of patients: those with a particular type of mitral regurgitation who were considered a surgery risk.
“The reality is, there is no perfect procedure,” said Jason Rogers, an interventional cardiologist and University of California-Davis professor who is an Abbott consultant. The company referred KFF Health News to Rogers as an authority on MitraClip. He called MitraClip “extremely safe” and said some patients treated with it are “on death’s door to begin with.”
“At least you’re trying to do something for them,” he said.
Conflicting Studies
In 2019, the FDA expanded its approval of MitraClip to a wider set of patients.
The agency based that decision on a clinical trial in the United States and Canada that Abbott not only sponsored but also helped design and manage. It participated in site selection and data analysis, according to a September 2018 New England Journal of Medicine paper reporting the trial results. Some of the authors received consulting fees from Abbott, the paper disclosed.
A separate study in France reached a different conclusion. It found that, for some patients who fit the expanded profile, the device did not significantly reduce deaths or hospitalizations for heart failure over a year.
The French study, which appeared in the New England Journal of Medicine in August 2018, was funded by the government of France and Abbott. As with the North American study, some of the researchers disclosed they had received money from Abbott. However, the write-up in the journal said Abbott played no role in the design of the French trial, the selection of sites, or in data analysis.
Gregg Stone, one of the leaders of the North American study, said there were differences between patients enrolled in the two studies and how they were medicated. In addition, outcomes were better in the North American study in part because doctors in the U.S. and Canada had more MitraClip experience than their counterparts in France, Stone said.
Stone, a clinical trial specialist with a background in interventional cardiology, acknowledged skepticism toward studies sponsored by manufacturers.
“There are some people who say, ‘Oh, well, you know, these results may have been manipulated,’” he said. “But I can guarantee you that’s not the truth.”
‘Nationwide Scheme’
A former Abbott employee alleges in a lawsuit that after MitraClip won approval, the company promoted the device to doctors and hospitals using inducements such as free marketing support, the chance to participate in Abbott clinical trials, and payments for participating in “sham speaker programs.”
The former employee alleges that she was instructed to tell referring physicians that if they observed mitral regurgitation in their patients to “just send it” for a MitraClip procedure because “everything can be clipped.” She also alleges that, using a script, she was told to promote the device to hospital administrators based on financial advantages such as “growth opportunities through profitable procedures, ancillary tests, and referral streams.”
The inducements were part of a “nationwide scheme” of illegal kickbacks that defrauded government health insurance programs including Medicare and Medicaid, the lawsuit claims.
The company denied doing anything illegal and said in a court filing that “to help its groundbreaking therapy reach patients, Abbott needed to educate cardiologists and other healthcare providers.”
Those efforts are “not only routine, they are laudable — as physicians cannot use, or refer a patient to another doctor who can use, a device that they do not understand or in some cases even know about,” the company said in the filing.
Under federal law, the person who filed the suit can receive a share of any money the government recoups from Abbott. The suit was filed by a company associated with a former employee in Abbott’s Structural Heart Division, Lisa Knott. An attorney for the company declined to comment and said Knott had no comment.
Reports to the FDA
As doctors started using MitraClip, the FDA began receiving reports about malfunctions and cases in which the product might have caused or contributed to a death or an injury.
According to some reports, clips detached from valve flaps. Flaps became damaged. Procedures were aborted. Mitral leakage worsened. Doctors struggled to control the device. Clips became “entangled in chordae” — cord-like structures also known as heartstrings that connect the valve flaps to the heart muscle. Patients treated with MitraClip underwent corrective operations.
As of March 2024, the FDA had received more than 17,000 reports documenting more than 22,000 “events” involving mitral valve repair devices, FDA data shows. All but about 200 of those reports mention one iteration of MitraClip or another, a KFF Health News review of FDA data found.
Almost all the reports came from Abbott. The FDA requires manufacturers to submit reports when they learn of mishaps potentially related to their devices.
The reports are not proof that devices caused problems, and the same event might be reported multiple times. Other events may go unreported.
Despite the reports’ limitations, the FDA provides an analysis of them for the public on its website.
MitraClip’s risks weren’t a surprise.
Like the rapid-fire fine print in television ads for prescription drugs, the original product label for the device listed more than 60 types of potential complications.
Indeed, during clinical research on the device, about 6% of patients implanted with MitraClip died within 30 days, according to the label. Almost 1 in 4 — 23.6% – were dead within a year.
The FDA spokesperson, Harrison, pointed to a study originally published in 2021 in The Annals of Thoracic Surgery, based on a central registry of mitral valve procedures, that found lower rates of death after MitraClip went on the market.
“These data confirmed that the MitraClip device remains safe and effective in the real-world setting,” Harrison said.
But the study’s authors, several of whom disclosed financial or other connections to Abbott, said data was missing for more than a quarter of patients one year after the procedure.
A major measure of success would be the proportion of MitraClip patients who are alive “with an acceptable quality of life” a year after undergoing the procedure, the study said. Because such information was available for fewer than half of the living patients, “we have omitted those outcomes from this report,” the authors wrote.
If you’ve had an experience with MitraClip or another medical device and would like to tell KFF Health News about it, click here to share your story with us.
KFF Health News audience engagement producer Tarena Lofton contributed to this report.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

It Didn’t Start with You – by Mark Wolynn
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There is a trend in psychology to “blame the parents” for “childhood trauma” that can result in problems later in life. Sometimes fairly, sometimes not. This book’s mostly not about that.
It does touch on our own childhood trauma, if applicable. But mostly, it’s about epigenetic trauma inheritance. In other words, not just trauma that’s passed on in terms of “the cycle of abuse”, but trauma that’s passed on in terms of “this generation experienced trauma x, developed trauma response y, encoded it epigenetically, and passed it on to their offspring”.
So, how does one heal from a trauma one never directly experienced, and just inherited the response to it? That’s what most of this book is about, after establishing how epigenetic trauma inheritance works.
The author, a therapist, provides practical advice for how to do the things that can be done to rewrite the epigenetic code we inherited. Better late than never!
Bottom line: it is well-established that trauma is inheritable. But unlike one’s eye color or the ability to smell asparagus metabolites in urine, we can rewrite epigenetic things, to a degree. This book explains how.
Click here to check out It Didn’t Start With You, and put things to rest!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

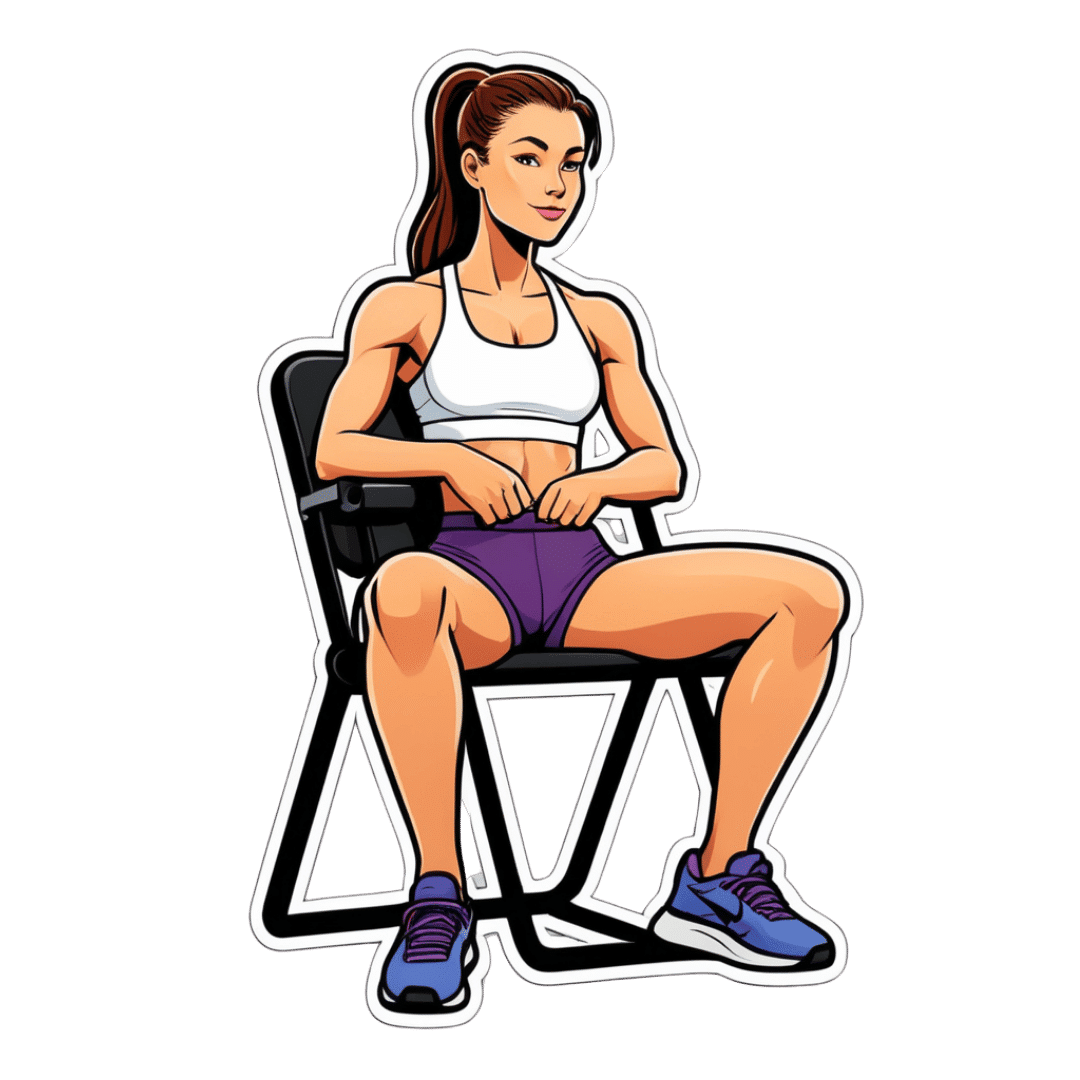
How To Reduce Knee Pain After Sitting
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Sitting is bad for the health, and doubly so if you have arthritis, as a lack of regular movement can cause joints to “seize up”. So, what to do about it if you have to sit for an extended time?
Dr. Alyssa Kuhn, arthritis specialist, explains:
Movement remains key
The trick is to continue periodically moving, notwithstanding that you may need to remain seated. So…
- Heel slides
- Straighten and bend your leg by sliding or lifting your heel.
- Promotes blood flow and reduces fluid buildup in the knee.
- Helps lubricate the joint, making standing up easier.
- Heel lifts
- Lift your heels up and down while keeping feet on the ground.
- This one’s ideal for tight spaces, such as when riding in a car or airplane.
- Improves blood circulation and can reduce ankle swelling and leg heaviness.
Do 20–30 repetitions every now and again, to keep your joints moving.
Note: if you are a wheelchair user whose legs lack the strength and/or motor function to do this, in this case it’s the movement of the leg that counts, not where that movement originated from. So, if you use one hand to lift your leg slightly and the other to push it like a swing, that will also be sufficient to give the joint the periodic movement it needs.
For more on all of this plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Stand Up For Your Health (Or Don’t) ← our main feature on this also includes more things you can do if you must sit, to make sitting less bad!
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
- Heel slides