Get Better Sleep: Beyond “Sleep Hygiene”
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Better Sleep, Better Life!
This is Arianna Huffington. Yes, that Huffington, of the Huffington Post. But! She’s also the CEO of Thrive Global, a behavior change tech company with the mission of changing the way we work and live—in particular, by challenging the idea that burnout is the required price of success.
The power of better sleep
Sleep is a very important, but most often neglected, part of good health. Here are some of Huffington’s top insights from her tech company Thrive, and as per her “Sleep Revolution” initiative.
Follow your circadian rhythm
Are you a night owl or a morning lark? Whichever it is, roll with it, and plan around that if your lifestyle allows for such. While it is possible to change from one to the other, we do have a predisposition towards one or the other, and will generally function best when not fighting it.
This came about, by the way, because we evolved to have half of us awake in the mornings and half in the evenings, to keep us all safe. Socially we’ve marched onwards from that point in evolutionary history, but our bodies are about a hundred generations behind the times, and that’s just what we have to work with!
Don’t be afraid (or ashamed!) to take naps
Naps, done right, can be very good for the health—especially if we had a bad night’s sleep the previous night.
Thrive found that workers are more productive when they have nap rooms, and (following on a little from the previous point) are allowed to sleep in or work from home.
See also: How To Nap Like A Pro (No More “Sleep Hangovers”!)
Make sure you have personal space available in bed
The correlation between relationship satisfaction and sleeping close to one’s partner has been found to be so high that it’s even proportional: the further away a couple sleeps from each other, the less happy they are. But…
Partners who got good sleep the previous night, will be more likely to want intimacy on any given night—at a rate of an extra 14% per extra hour of sleep the previous night. So, there’s a trade-off, as having more room in bed tends to result in better sleep. Time to get a bigger bed?
What gets measured, gets done
This goes for sleep, too! Not only does dream-journaling in the morning cue your subconscious to prepare to dream well the following night, but also, sleep trackers and sleep monitoring apps go a very long way to improving sleep quality, even if no extra steps are consciously taken to “score better”.
We’ve previously reviewed some of the most popular sleep apps; you can check out for yourself how they measured up:
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Biggest Lie About Arthritis

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Alyssa Kuhn, arthritis specialist, wishes more people knew this common belief isn’t true:
Move on from this myth
Contrary to popular belief, movement does not worsen arthritis—avoiding movement does. Inactivity reduces what your body is capable of, and accelerates stiffness, weakness, and pain.
In fact, by the science, exercise ranks as the most effective arthritis treatment, matching or exceeding popular drug-based pain relief, without the side effects. And as for ibuprofen and friends, a 2024 study found regular use of NSAIDs (like ibuprofen) was linked to worse symptoms and a threefold increase in total knee replacement risk:
The biggest problem is that medications mask pain, but don’t address the underlying problem, and so deterioration can be accelerated by wear and tear while the body isn’t paying attention.
But, doesn’t movement make the wear and tear worse?
It can, if you overdo it and/or do it very wrong. However, done gently and correctly, movement actually helps, because cartilage behaves like a sponge—moving a joint compresses and releases it, allowing nutrients to circulate. Without movement, cartilage is underfed, increasing irritation, inflammation, and pain.
Three strategies for getting it right:
- Start simple: focus on two or three exercises at a time, rather than trying to do everything at once.
- Warm up: give your body time to prepare before walking, stairs, sports, or lifting. Warm-ups are not just for intentional exercise sessions! They’re useful before any change in physical activity.
- Adapt rather than quitting: modify movements instead of abandoning them. For example, you could raise a chair for squats, use your arms to assist you, change how you use the stairs, or briefly reset your movement during a walk.
Lastly, Dr. Kuhn wants us to know that arthritis is not a binary of “can” or “can’t.”
The more useful question is: “how can I do this differently right now?”
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
For a much more comprehensive guide to ideal exercises, consider:
Yoga Therapy for Arthritis – by Dr. Steffany Moonaz & Erin Byron
…which is a particularly good book, much better than most of its kind, because:
- One of the problems with arthritis and exercise is that arthritis can often impede exercise.
- Another of the problems with arthritis and exercise is that some kinds of exercise can exacerbate arthritis.
This book deals with both of those issues, by providing yoga specifically tailored to living with arthritis. Indeed, the first-listed author’s PhD in public health was the result of 8 years of study developing an evidence-based yoga program for people with arthritis, including osteoarthritis and rheumatoid arthritis.
The authors take the view that arthritis is a whole-person disease (i.e. it affects all parts of you), and so addressing it requires a whole-person approach, which is what this book delivers, and so that’s why we highly recommend it.
Take care!
Share This Post
-

Diet Tips for Crohn’s Disease
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝Doctors are great at saving lives like mine. I’m a two time survivor of colon cancer and have recently been diagnosed with Chron’s disease at 62. No one is the health system can or is prepared to tell me an appropriate diet to follow or what to avoid. Can you?❞
Congratulations on the survivorship!
As to Crohn’s, that’s indeed quite a pain, isn’t it? In some ways, a good diet for Crohn’s is the same as a good diet for most other people, with one major exception: fiber
…and unfortunately, that changes everything, in terms of a whole-foods majority plant-based diet.
What stays the same:
- You still ideally want to eat a lot of plants
- You definitely want to avoid meat and dairy in general
- Eating fish is still usually* fine, same with eggs
- Get plenty of water
What needs to change:
- Consider swapping grains for potatoes or pasta (at least: avoid grains)
- Peel vegetables that are peelable; discard the peel or use it to make stock
- Consider steaming fruit and veg for easier digestion
- Skip spicy foods (moderate spices, like ginger, turmeric, and black pepper, are usually fine in moderation)
Much of this latter list is opposite to the advice for people without Crohn’s Disease.
*A good practice, by the way, is to keep a food journal. There are apps that you can get for free, or you can do it the old-fashioned way on paper if prefer.
But the important part is: make a note not just of what you ate, but also of how you felt afterwards. That way, you can start to get a picture of patterns, and what’s working (or not) for you, and build up a more personalized set of guidelines than anyone else could give to you.
We hope the above pointers at least help you get going on the right foot, though!
Share This Post
-

Is Cutting Calories The Key To Healthy Long Life?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Caloric Restriction with Optimal Nutrition

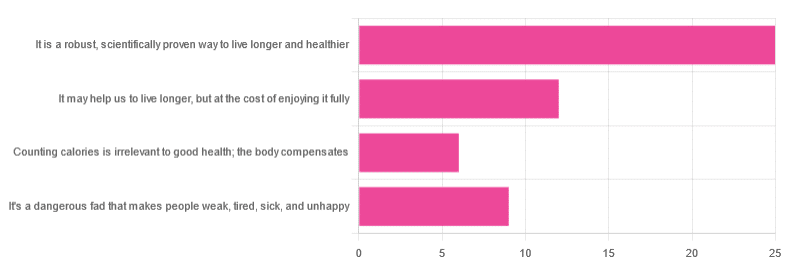
Yesterday, we asked you “What is your opinion of caloric restriction as a health practice?” and got the above-depicted, below-described spread of responses:
- 48% said “It is a robust, scientifically proven way to live longer and healthier”
- 23% said “It may help us to live longer, but at the cost of enjoying it fully”
- 17% said “It’s a dangerous fad that makes people weak, tired, sick, and unhealthy”
- 12% said “Counting calories is irrelevant to good health; the body compensates”
So… What does the science say?
A note on terms, first
“Caloric restriction” (henceforth: CR), as a term, sees scientific use to mean anything from a 25% reduction to a 50% reduction, compared to metabolic base rate.
This can also be expressed the other way around, “dropping to 60% of the metabolic base rate” (i.e., a 40% reduction).
Here we don’t have the space to go into much depth, so our policy will be: if research papers consider it CR, then so will we.
A quick spoiler, first
The above statements about CR are all to at least some degree True in one way or another.
However, there are very important distinctions, so let’s press on…
CR is a robust, scientifically proven way to live longer and healthier: True or False?
True! This has been well-studied and well-documented. There’s more science for this than we could possibly list here, but here’s a good starting point:
❝Calorie restriction (CR), a nutritional intervention of reduced energy intake but with adequate nutrition, has been shown to extend healthspan and lifespan in rodent and primate models.
Accumulating data from observational and randomized clinical trials indicate that CR in humans results in some of the same metabolic and molecular adaptations that have been shown to improve health and retard the accumulation of molecular damage in animal models of longevity.
In particular, moderate CR in humans ameliorates multiple metabolic and hormonal factors that are implicated in the pathogenesis of type 2 diabetes, cardiovascular diseases, and cancer, the leading causes of morbidity, disability and mortality❞
Source: Ageing Research Reviews | Calorie restriction in humans: an update
See also: Caloric restriction in humans reveals immunometabolic regulators of health span
We could devote a whole article (or a whole book, really) to this, but the super-short version is that it lowers the metabolic “tax” on the body and allows the body to function better for longer.
CR may help us to live longer, but at the cost of enjoying it fully: True or False?
True or False, contingently, depending on what’s important to you. And that depends on psychology as much as physiology, but it’s worth noting that there is often a selection bias in the research papers; people ill-suited to CR drop out of the studies and are not counted in the final data.
Also, relevant for a lot of our readers, most (human-based) studies recruit people over 18 and under 60. So while it is reasonable to assume the same benefits will be carried over that age, there is not nearly as much data for it.
Studies into CR and Health-Related Quality of Life (HRQoL) have been promising, and/but have caveats:
❝In non-obese adults, CR had some positive effects and no negative effects on HRQoL.❞
❝We do not know what degree of CR is needed to achieve improvements in HRQoL, but we do know it requires an extraordinary amount of support.
Therefore, the incentive to offer this intervention to a low-risk, normal or overweight individual is lacking and likely not sustainable in practice.❞
CR a dangerous fad that makes people weak, tired, sick, and unhealthy: True or False?
True if it is undertaken improperly, and/or without sufficient support. Many people will try CR and forget that the idea is to reduce metabolic load while still getting good nutrition, and focus solely on the calorie-counting.
So for example, if a person “saves” their calories for the day to have a night out in a bar where they drink their calories as alcohol, then this is going to be abysmal for their health.
That’s an extreme example, but lesser versions are seen a lot. If you save your calories for a pizza instead of a night of alcoholic drinks, then it’s not quite so woeful, but for example the nutrition-to-calorie ratio of pizza is typically not great. Multiply that by doing it as often as not, and yes, someone’s health is going to be in ruins quite soon.
Counting calories is irrelevant to good health; the body compensates: True or False?
True if by “good health” you mean weight loss—which is rarely, if ever, what we mean by “good health” here at 10almonds (unless we clarify such), but it’s a very common association and indeed, for some people it’s a health goal. You cannot sustainably and healthily lose weight by CR alone, especially if you’re not getting optimal nutrition.
Your body will notice that you are starving, and try to save you by storing as much fat as it can, amongst other measures that will similarly backfire (cortisol running high, energy running low, etc).
For short term weight loss though, yes, it’ll work. At a cost. That we don’t recommend.
❝By itself, decreasing calorie intake will have a limited short-term influence.❞
Source: Reducing Calorie Intake May Not Help You Lose Body Weight
See also…
❝Caloric restriction is a commonly recommended weight-loss method, yet it may result in short-term weight loss and subsequent weight regain, known as “weight cycling”, which has recently been shown to be associated with both poor sleep and worse cardiovascular health❞
Source: Dieting Behavior Characterized by Caloric Restriction
In summary…
Caloric restriction is a well-studied area of health science. We know:
- Practised well, it can extend not only lifespan, but also healthspan
- Practised well, it can improve mood, energy, sexual function, and the other things people fear losing
- Practised badly, it can be ruinous to the health—it is critical to practise caloric restriction with optimal nutrition.
- Practised badly, it can lead to unhealthy weight loss and weight regain
One final note…
If you’ve tried CR and hated it, and you practised it well (e.g., with optimal nutrition), then we recommend just not doing it.
You could also try intermittent fasting instead, for similar potential benefits. If that doesn’t work out either, then don’t do that either!
Sometimes, we’re just weird. It can often be because of a genetic or epigenetic quirk. There are usually workarounds, and/but not everything that’s right for most people will be right for all of us.
Take care!
Share This Post

Related Posts
-
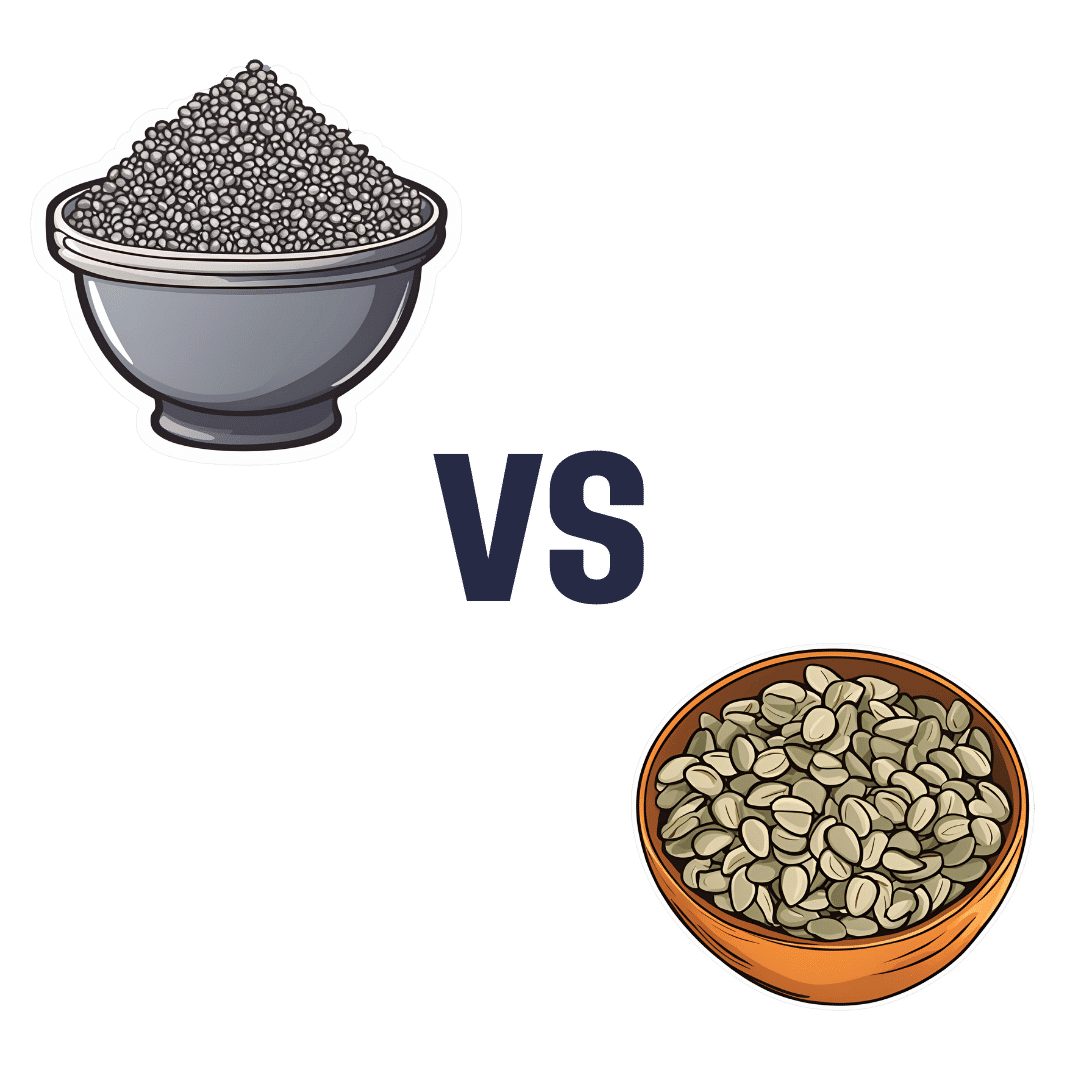
Chia Seeds vs Pumpkin Seeds – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing chia seeds to pumpkin seeds, we picked the chia.
Why?
Both are great! But chia is best.
Note: we’re going to abbreviate them both to “chia” and “pumpkin”, respectively, but we’ll still be referring to the seeds throughout.
In terms of macros, pumpkin has a little more protein and notably higher carbs, whereas chia has nearly 2x the fiber, as well as more fat, and/but they are famously healthy fats. We’ll call this category a subjective win for chia, though you might disagree if you want to prioritize an extra 2g of protein per 100g (for pumpkin) over an extra 16g of fiber per 100g (for chia). Chia is also vastly preferable for omega-3.
When it comes to vitamins, pumpkin is marginally higher in vitamin A, while chia is a lot higher in vitamins B1, B2, B3, B9, C, and E. An easy win for chia.
In the category of minerals, for which pumpkin seeds are so famously a good source, chia has a lot more calcium, copper, iron, magnesium, manganese, phosphorus, and selenium. On the other hand, pumpkin has more potassium and zinc. Still, that’s a 7:2 win for chia.
Adding up the categories makes for a very compelling win for the humble chia seed.
Want to learn more?
You might like to read:
If You’re Not Taking Chia, You’re Missing Out: The Tiniest Seeds With The Most Value
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Relationships: When To Stick It Out & When To Call It Quits
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Like A Ship Loves An Anchor?
Today’s article may seem a little bit of a downer to start with, but don’t worry, it picks up again too. Simply put, we’ve written before about many of the good parts of relationships, e.g:
Only One Kind Of Relationship Promotes Longevity This Much!
…but what if that’s not what we have?
Note: if you have a very happy, secure, fulfilling, joyous relationship, then, great! Or if you’re single and happy, then, also great! Hopefully you will still find today’s feature of use if you find yourself advising a friend or family member one day. So without further ado, let’s get to it…
You may be familiar with the “sunk cost fallacy”; if not: it’s what happens when a person or group has already invested into a given thing, such that even though the thing is not going at all the way they hoped, they now want to continue trying to make that thing work, lest their previous investment be lost. But the truth is: if it’s not going to work, then the initial investment is already lost, and pouring out extra won’t help—it’ll just lose more.
That “investment” in a given thing could be money, time, energy, or (often the case) a combination of the above.
In the field of romance, the “sunk cost fallacy” keeps a lot of bad relationships going for longer than perhaps they should, and looking back (perhaps after a short adjustment period), the newly-single person says “why did I let that go on?” and vows to not make the same mistake again.
But that prompts the question: how can we know when it’s right to “keep working on it, because relationships do involve work”, as perfectly reasonable relationship advice often goes, and when it’s right to call it quits?
Should I stay or should I go?
Some questions for you (or perhaps a friend you might find yourself advising) to consider:
- What qualities do you consider the most important for a partner to have—and does your partner have them?
- If you described the worst of your relationship to a close friend, would that friend feel bad for you?
- Do you miss your partner when they’re away, or are you glad of the break? When they return, are they still glad to see you?
- If you weren’t already in this relationship, would you seek to enter it now? (This takes away sunk cost and allows a more neutral assessment)
- Do you feel completely safe with your partner (emotionally as well as physically), or must you tread carefully to avoid conflict?
- If your partner decided tomorrow that they didn’t want to be with you anymore and left, would that be just a heartbreak, or an exciting beginning of a new chapter in your life?
- What things would you generally consider dealbreakers in a relationship—and has your partner done any of them?
The last one can be surprising, by the way. We often see or hear of other people’s adverse relationship situations and think “I would never allow…” yet when we are in a relationship and in love, there’s a good chance that we might indeed allow—or rather, excuse, overlook, and forgive.
And, patience and forgiveness certainly aren’t inherently bad traits to have—it’s just good to deploy them consciously, and not merely be a doormat.
Either way, reflect (or advise your friend/family member to reflect, as applicable) on the “score” from the above questions.
- If the score is good, then maybe it really is just a rough patch, and the tools we link at the top and bottom of this article might help.
- If the score is bad, the relationship is bad, and no amount of historic love or miles clocked up together will change that. Sometimes it’s not even anyone’s fault; sometimes a relationship just ran its course, and now it’s time to accept that and turn to a new chapter.
“At my age…”
As we get older, it’s easy for that sunk cost fallacy to loom large. Inertia is heavy, the mutual entanglement of lives is far-reaching, and we might not feel we have the same energy for dating that we did when we were younger.
And there may sometimes be a statistical argument for “sticking it out” at least for a while, depending on where we are in the relationship, per this study (with 165,039 participants aged 20–76), which found:
❝Results on mean levels indicated that relationship satisfaction decreased from age 20 to 40, reached a low point at age 40, then increased until age 65, and plateaued in late adulthood.
As regards the metric of relationship duration, relationship satisfaction decreased during the first 10 years of the relationship, reached a low point at 10 years, increased until 20 years, and then decreased again.❞
Source: Development of Relationship Satisfaction Across the Life Span: A Systematic Review and Meta-Analysis
And yet, when it comes to prospects for a new relationship…
- If our remaining life is growing shorter, then it’s definitely too short to spend in an unhappy relationship
- Maybe we really won’t find romance again… And maybe that’s ok, if w’re comfortable making our peace with that and finding joy in the rest of life (this widowed writer (hi, it’s me) plans to remain single now by preference, and her life is very full of purpose and beauty and joy and yes, even love—for family, friends, etc, plus the memory of my wonderful late beloved)
- Nevertheless, the simple fact is: many people do find what they go on to describe as their best relationship yet, late in life ← this study is with a small sample size, but in this case, even anecdotal evidence seems sufficient to make the claim reasonable; probably you personally know someone who has done so. If they can, so can you, if you so wish.
- Adding on to that last point… Later life relationships can also offer numerous significant advantages unique to such (albeit some different challenges too—but with the right person, those challenges are just a fun thing to tackle together). See for example:
An exploratory investigation into dating among later‐life women
And about those later-life relationships that do work? They look like this:
this one looks like the title says it all, but it really doesn’t, and it’s very much worth at least reading the abstract, if not the entire paper—because it talks a lot about the characteristics that make for happy or unhappy relationships, and the effect that those things have on people. It really is very good, and quite an easy read.
See again: Healthy Relationship, Healthy Life
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Families including someone with mental illness can experience deep despair. They need support
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In the aftermath of the tragic Bondi knife attack, Joel Cauchi’s parents have spoken about their son’s long history of mental illness, having been diagnosed with schizophrenia at age 17. They said they were “devastated and horrified” by their son’s actions. “To you he’s a monster,” said his father. “But to me he was a very sick boy.”
Globally, one out of every eight people report a mental illness. In Australia, one in five people experience a mental illness in their lifetime.
Mental illness and distress affects not only the person living with the condition, but family members and communities. As the prevalence of mental health problems grows, the flow-on effect to family members, including caregivers, and the impact on families as a unit, is also rising.
While every family is different, the words of the Cauchis draw attention to how families can experience distress, stress, fear, powerlessness, and still love, despite the challenges and trauma. How can they help a loved one? And who can they turn to for support?
The role of caregivers
Informal caregivers help others within the context of an existing relationship, such as a family member. The care they provide goes beyond the usual expectations or demands of such relationships.
Around 2.7 million Australians provide informal care. For almost a third of these the person’s primary medical diagnosis is psychological or psychiatric.
It has long been acknowledged that those supporting a family member with ongoing mental illness need support themselves.
In the 1980s, interest grew in caregiving dynamics within families of people grappling with mental health issues. Subsequent research recognised chronic health conditions not only affect the quality of life and wellbeing of the people experiencing them, but also impose burdens that reverberate within relationships, caregiving roles, and family dynamics over time.
Past studies have shown families of those diagnosed with chronic mental illness are increasingly forced to manage their own depression, experience elevated levels of emotional stress, negative states of mind and decreased overall mental health.
Conditions such as depression, anxiety disorders, bipolar disorder, and schizophrenia can severely impact daily functioning, relationships, and overall quality of life. Living with mental illness is often accompanied by a myriad of challenges. From stigma and discrimination to difficulty accessing adequate health care and support services. Patients and their families navigate a complex and often isolating journey.
The family is a system
The concept of family health acknowledges the physical and psychological wellbeing of a person is significantly affected by the family.
Amid these challenges, family support emerges as a beacon of hope. Research consistently demonstrates strong familial relationships and support systems play a pivotal role in mitigating the adverse effects of mental illness. Families provide emotional support, practical assistance, and a sense of belonging that are vital for people struggling with mental illness.
My recent research highlights the profound impact of mental illness on family dynamics, emphasising the resilience and endurance shown by participants. Families struggling with mental illness often experience heightened emotional fluctuations, with extreme highs and lows. The enduring nature of family caregiving entails both stress and adaptation over an extended period. Stress associated with caregiving and the demands on personal resources and coping mechanisms builds and builds.
Yet families I’ve interviewed find ways to live “a good life”. They prepare for the peaks and troughs, and show endurance and persistence. They make space for mental illness in their daily lives, describing how it spurs adaptation, acceptance and inner strength within the family unit.
When treating a person with mental illness, health practitioners need to consider the entire family’s needs and engage with family members. By fostering open and early dialogue and providing comprehensive support, health-care professionals can empower families to navigate the complexities of mental illness while fostering resilience and hope for the future. Family members express stories of an inner struggle, isolation and exhaustion.

Family bonds can be a cornerstone of wellbeing. Gorodenkoff/Shutterstock Shifting the focus
There is a pressing need for a shift in research priorities, from illness-centered perspectives to a strengths-based focus when considering families “managing” mental illness.
There is transformative potential in harnessing strengths to respond to challenges posed by mental illnesses, while also supporting family members.
For people facing mental health challenges, having loved ones who listen without judgement and offer empathy can alleviate feelings of despair. Beyond emotional support, families often serve as crucial caregivers, assisting with daily tasks, medication management and navigating the health-care system.
As the Cauchi family so painfully articulated, providing support for a family member with mental illness is intensely challenging. Research shows caregiver burnout, financial strain and strained relationships are common.
Health-care professionals should prioritise support for family members at an early stage. In Australia, there are various support options available for families living with mental illness. Carer Gateway provides information, support and access to services. Headspace offers mental health services and supports to young people and their families.
Beyond these national services, GPs, nurses, nurse practitioners and local community health centres are key to early conversations. Mental health clinics and hospitals often target family involvement in treatment plans.
While Australia has made strides in recognising the importance of family support, challenges persist. Access to services can vary based on geographic location and demand, leaving some families under-served or facing long wait times. And the level of funding and resources allocated to family-oriented mental health support often does not align with the demand or complexity of need.
In the realm of mental illness, family support serves as a lifeline for people navigating the complexities of their conditions.
If this article has raised issues for you, or if you’re concerned about someone you know, call Lifeline on 13 11 14.
Amanda Cole, Lead, Mental Health, Edith Cowan University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: