The Beetroot Benefits That Depend On Your Age
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve written before about beetroot’s considerable health benefits: Beetroot For More Than Just Your Blood Pressure
We even covered how to make it better in a surprising way: Beetroot Juice & Caffeine Work Better Than Either Alone
But what’s this about age differences?
Different for younger and older people
Researchers (Dr. Anni Vanhatalo et al.) investigated this, and wondered how much of beetroot’s beneficial effect is due to boosting nitric oxide (NO) production, something that aging typically reduces, but that nitrate-rich beetroot improves.
To test this, they did a randomized, placebo-controlled, double-blind crossover trial with young adults (18–30) and older adults (67–79). They excluded participants with cardiovascular, metabolic, pulmonary, or oral disease; smokers; anyone with high blood pressure (here defined as >140/90, notwithstanding that the usual standard is >130/90), and anyone who had recently used antibiotics.
The interventions were:
- nitrate-rich beetroot juice (2 × 70 ml/day, ~595 mg nitrate each)
- nitrate-depleted beetroot juice (same quantity of juice, no nitrate, functioning as placebo)
- antiseptic mouthwash (because they suspected that oral bacteria played a role)
These they tested with two-week treatment phases, with washout periods between (since the groups switched roles, being as it was a crossover trial, it was important to ensure that each group was not still being affected by the previous intervention).
What they measured: they did tongue swabs for microbiome sequencing, they checked plasma nitrate/nitrite for NO bioavailability, they also recorded blood pressure (brachial and central), endothelial function (flow-mediated dilation), and arterial stiffness.
What they found:
- Endothelial function and arterial stiffness remained unchanged in all groups. It seems this is simply not something that beetroot juice affects.
- The older adults had higher baseline blood pressure, and/but nitrate-rich beetroot juice lowered brachial mean arterial pressure in older adults while it had no significant effect in younger adults.
- In the category of oral microbiome changes, they found that in older adults, beetroot juice reduced Prevotella-dominated bacterial linked with DNRA (which diverts nitrite away from NO production), and that reduction in Prevotella correlated with higher plasma nitrite and lower blood pressure; nitrate-rich beetroot juice increased nitrate-reducing genera Neisseria and Rothia, especially in older adults, having only modest benefits for younger adults. Antiseptic mouthwash reduced microbial diversity (shocking nobody) and impaired vascular function.
- Nitrate-depleted juice still raised plasma nitrate/nitrite modestly and had a small lowering effect on blood pressure in older adults. This may have been because of:
- placebo effect doing its thing
- imperfect depletion of nitrates
- other unknown factors
- a combination of the above
In summary: in older adults, beetroot juice improves the oral microbiome and, partly because of that, lowers blood pressure. Younger adults get only marginal benefits at best, and use of antiseptic mouthwash completely wipes out the benefits.
You can read the paper itself, here: Ageing modifies the oral microbiome, nitric oxide bioavailability and vascular responses to dietary nitrate supplementation
Before you get juicing, there are some things you should be aware of: 3 Day Juice Fasting? Not So Fast! ← this isn’t even just about the glycemic index issue (juices being stripped of fiber), and is rather mostly about the microbiome problems juices can cause without sufficient dietary fiber (so, not so much a problem if, for example, you have a juice after a fibrous meal).
Not a fan of juices? This writer doesn’t love juices most of the time either, but we can enjoy: Hearty Healthy Ukrainian Borscht ← from our recipes archive!
Remember when…
…we talked about Dr. Ellie Phillips’ advices with regard to oral health?
In few words, Dr. Phillips promotes protecting oral microbial diversity by avoiding antibacterial mouthwashes; the study we talked about today also validated that, showing how antiseptic mouthwash (unsurprisingly) reduced microbial diversity and (importantly and relevantly) impaired vascular function.
Now, she often points to imbalances where certain bacteria overgrow; this study showed Prevotella dominance (i.e., harmful bacteria being too plentiful) diverts nitrite away from NO production, worsening cardiovascular function—a good example of how oral imbalances have systemic effects.
So, how to kill the bad bacteria without harming the good ones? Critically, diet can feed the protective oral bacteria; here, nitrate-rich beetroot juice improved blood pressure by shifting the oral microbiome towards beneficial nitrate-reducing genera (e.g. the Neisseria and Rothia in this study). As for the rest, Dr. Phillips advocates simple, natural methods (xylitol, remineralizing foods, protective rinses) instead of harsh chemicals. As we’ve learned today, dietary strategies (like beetroot juice) can also play their part as a natural, safe way to help your oral microbiome to help you.
For research on this by a third source, see: Make Your Saliva Better For Your Health
Want to learn more?
With regard to nitrates and health, you might like:
The Nitric Oxide (NO) Solution – by Dr. Nathan Bryan & Janet Zand
…and, with a focus on beets (roots and leaves):
Beet The Odds – by Dr. Nathan Bryan & Carolyn Pierini
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Cooling Bulgarian Tarator

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The “Bulgarian” qualifier is important here because the name “tarator” is used to refer to several different dishes from nearby-ish countries, and they aren’t the same. Today’s dish (a very healthy and deliciously cooling cucumber soup) isn’t well-known outside of Bulgaria, but it should be, and with your help we can share it around the world. It’s super-easy and takes only about 10 minutes to prepare:
You will need
- 1 large cucumber, cut into small (¼” x ¼”) cubes or small (1″ x ⅛”) batons (the size is important; any smaller and we lose texture; any larger and we lose the balance of the soup, and also make it very different to eat with a spoon)
- 2 cups plain unsweetened yogurt (your preference what kind; live-cultured of some kind is best, and yes, vegan is fine too)
- 1½ cup water, chilled but not icy (fridge-temperature is great)
- ½ cup chopped walnuts (substitutions are not advised; omit if allergic)
- ½ bulb garlic, minced
- 3 tbsp fresh dill, chopped
- 2 tbsp extra virgin olive oil
- 1 tsp black pepper, coarse ground
- ½ tsp MSG* or 1 tsp low-sodium salt
Method
(we suggest you read everything at least once before doing anything)
1) Mix the cucumber, garlic, 2 tbsp of the dill, oil, MSG-or-salt and pepper in a big bowl
2) Add the yogurt and mix it in too
3) Add the cold water slowly and stir thoroughly; it may take a minute to achieve smooth consistency of the liquid—it should be creamy but thin, and definitely shouldn’t stand up by itself
4) Top with the chopped nuts, and the other tbsp of dill as a garnish
5) Serve immediately, or chill in the fridge until ready to serve. It’s perfect as a breakfast or a light lunch, by the way.
Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- How To Really Look After Your Joints ← this is about how cucumber has phytochemicals that outperform glucosamine and chondroitin by 200%, at 1/135th of the dose
- Making Friends With Your Gut (You Can Thank Us Later)
- Is Dairy Scary? ← short answer in terms of human health is “not if it’s fermented”
- Why You Should Diversify Your Nuts!
- The Many Health Benefits Of Garlic
- Is “Extra Virgin” Worth It?
- Black Pepper’s Impressive Anti-Cancer Arsenal (And More)
- Monosodium Glutamate: Sinless Flavor-Enhancer Or Terrible Health Risk? ← *for those who are worried about the health aspects of MSG; it is healthier and safer than table salt
Take care!
Share This Post
-

Dealing With Waking Up In The Night
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝I’m now in my sixties and find that I invariably wake up at least once during the night. Is this normal? Even if it is, I would still like, once in a while, to sleep right through like a teenager. How might this be achieved, without pills?❞
Most people wake up briefly between sleep cycles, and forget doing so. But waking up for more than a brief moment is indeed best avoided. In men of your age, if you’re waking to pee (especially if it’s then not actually that easy to pee), it can be a sign of an enlarged prostate. Which is again a) normal b) not optimal.
By “without pills” we’ll assume you mean “without sleeping pills”. There are options to treat an enlarged prostate, including well-established supplements. We did a main feature on this:
Prostate Health: What You Should Know
If the cause of waking up is something else, then again this is common for everyone as we get older, and again it’s not optimal. But since there are so many possible causes (and thus solutions), it’s more than we can cover in less than a main feature, so we’ll have to revisit this later.
Meanwhile, take care!
Share This Post
-

What is PMDD?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Premenstrual dysphoric disorder (PMDD) is a mood disorder that causes significant mental health changes and physical symptoms leading up to each menstrual period.
Unlike premenstrual syndrome (PMS), which affects approximately three out of four menstruating people, only 3 percent to 8 percent of menstruating people have PMDD. However, some researchers believe the condition is underdiagnosed, as it was only recently recognized as a medical diagnosis by the World Health Organization.
Read on to learn more about its symptoms, the difference between PMS and PMDD, treatment options, and more.
What are the symptoms of PMDD?
People with PMDD typically experience both mood changes and physical symptoms during each menstrual cycle’s luteal phase—the time between ovulation and menstruation. These symptoms typically last seven to 14 days and resolve when menstruation begins.
Mood symptoms may include:
- Irritability
- Anxiety and panic attacks
- Extreme or sudden mood shifts
- Difficulty concentrating
- Depression and suicidal ideation
Physical symptoms may include:
- Fatigue
- Insomnia
- Headaches
- Changes in appetite
- Body aches
- Bloating
- Abdominal cramps
- Breast swelling or tenderness
What is the difference between PMS and PMDD?
Both PMS and PMDD cause emotional and physical symptoms before menstruation. Unlike PMS, PMDD causes extreme mood changes that disrupt daily life and may lead to conflict with friends, family, partners, and coworkers. Additionally, symptoms may last longer than PMS symptoms.
In severe cases, PMDD may lead to depression or suicide. More than 70 percent of people with the condition have actively thought about suicide, and 34 percent have attempted it.
What is the history of PMDD?
PMDD wasn’t added to the Diagnostic and Statistical Manual of Mental Disorders until 2013. In 2019, the World Health Organization officially recognized it as a medical diagnosis.
References to PMDD in medical literature date back to the 1960s, but defining it as a mental health and medical condition initially faced pushback from women’s rights groups. These groups were concerned that recognizing the condition could perpetuate stereotypes about women’s mental health and capabilities before and during menstruation.
Today, many women-led organizations are supportive of PMDD being an official diagnosis, as this has helped those living with the condition access care.
What causes PMDD?
Researchers don’t know exactly what causes PMDD. Many speculate that people with the condition have an abnormal response to fluctuations in hormones and serotonin—a brain chemical impacting mood— that occur throughout the menstrual cycle. Symptoms fully resolve after menopause.
People who have a family history of premenstrual symptoms and mood disorders or have a personal history of traumatic life events may be at higher risk of PMDD.
How is PMDD diagnosed?
Health care providers of many types, including mental health providers, can diagnose PMDD. Providers typically ask patients about their premenstrual symptoms and the amount of stress those symptoms are causing. Some providers may ask patients to track their periods and symptoms for one month or longer to determine whether those symptoms are linked to their menstrual cycle.
Some patients may struggle to receive a PMDD diagnosis, as some providers may lack knowledge about the condition. If your provider is unfamiliar with the condition and unwilling to explore treatment options, find a provider who can offer adequate support. The International Association for Premenstrual Disorders offers a directory of providers who treat the condition.
How is PMDD treated?
There is no cure for PMDD, but health care providers can prescribe medication to help manage symptoms. Some medication options include:
- Selective serotonin reuptake inhibitors (SSRIs), a class of antidepressants that regulate serotonin in the brain and may improve mood when taken daily or during the luteal phase of each menstrual cycle.
- Hormonal birth control to prevent ovulation-related hormonal changes.
- Over-the-counter pain medication like Tylenol, which can ease headaches, breast tenderness, abdominal cramping, and other physical symptoms.
Providers may also encourage patients to make lifestyle changes to improve symptoms. Those lifestyle changes may include:
- Limiting caffeine intake
- Eating meals regularly to balance blood sugar
- Exercising regularly
- Practicing stress management using breathing exercises and meditation
- Having regular therapy sessions and attending peer support groups
For more information, talk to your health care provider.
If you or anyone you know is considering suicide or self-harm or is anxious, depressed, upset, or needs to talk, call the Suicide & Crisis Lifeline at 988 or text the Crisis Text Line at 741-741. For international resources, here is a good place to begin.
This article first appeared on Public Good News and is republished here under a Creative Commons license.

Share This Post


Related Posts
-
Can Walking Really Burn Belly Fat? What Science Says
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Visceral belly fat is harmful and increases risks of heart disease, diabetes, and metabolic issues in general. Can walking get rid of it, or are more extreme measures needed? Science does have the answer:
Steps for good health
Contrary to popular belief, you don’t need extreme workouts or diets to lose belly fat—walking can indeed be highly effective.
Per studies, brisk walking (30–60 minutes, 3–5 times per week) significantly reduces visceral fat and waist circumference. And, shocking nobody, combining walking with healthy eating accelerates results. To be clear, because the video isn’t, that doesn’t mean you have to walk and eat at the same time; just, eat healthily and also walk regularly 😉
To maximize fat loss from walking:
- Be consistent (walk most days of the week).
- Walk briskly (able to talk, but not sing).
- If practical, include hills to challenge muscles and boost fat burn.
- Aim for 8,000–10,000 steps a day.
As for walking vs more targeted things like ab excesses: spot reduction is a myth—ab exercises alone won’t reduce belly fat, but walking promotes full-body reduction in excess fat.
Bonus: walking also improves mood, reduces stress, and supports heart health!
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Over-50s Physio: What My 5 Oldest Patients (Average Age 92) Do Right
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
What’s the difference between miscarriage and stillbirth?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What’s the difference? is a new editorial product that explains the similarities and differences between commonly confused health and medical terms, and why they matter.
Former US First Lady Michelle Obama revealed in her memoir she had a miscarriage. UK singer-songwriter and actor Lily Allen has gone on the record about her stillbirth.
Both miscarriage and stillbirth are sadly familiar terms for pregnancy loss. They can be traumatic life events for the prospective parents and family, and their impacts can be long-lasting. But the terms can be confused.
Here are some similarities and differences between miscarriage and stillbirth, and why they matter.
christinarosepix/Shutterstock Let’s start with some definitions
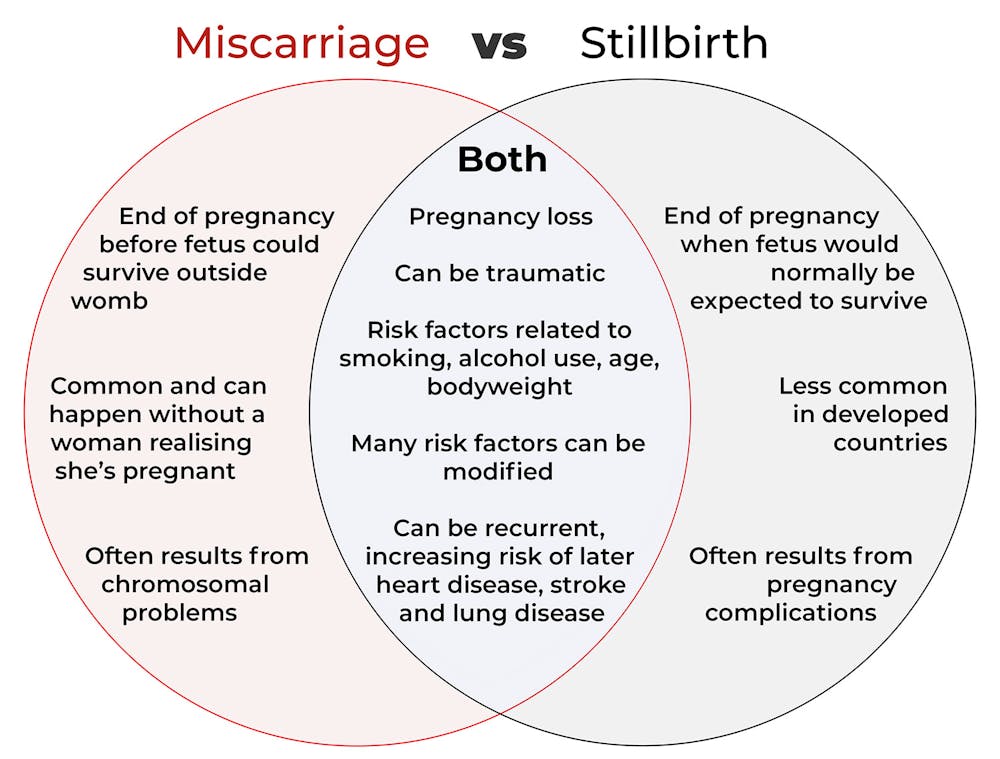
In broad terms, a miscarriage is when a pregnancy ends while the fetus is not yet viable (before it could survive outside the womb).
This is the loss of an “intra-uterine” pregnancy, when an embryo is implanted in the womb to then develop into a fetus. The term miscarriage excludes ectopic pregnancies, where the embryo is implanted outside the womb.
However, stillbirth refers to the end of a pregnancy when the fetus is normally viable. There may have been sufficient time into the pregnancy. Alternatively, the fetus may have grown large enough to be normally expected to survive, but it dies in the womb or during delivery.
The Australian Institute of Health and Welfare defines stillbirth as a fetal death of at least 20 completed weeks of gestation or with a birthweight of at least 400 grams.
Internationally, definitions of stillbirth vary depending on the jurisdiction.
How common are they?
It is difficult to know how common miscarriages are as they can happen when a woman doesn’t know she is pregnant. There may be no obvious symptoms or something that looks like a heavier-than-normal period. So miscarriages are likely to be more common than reported.
Studies from Europe and North America suggest a miscarriage occurs in about one in seven pregnancies (15%). More than one in eight women (13%) will have a miscarriage at some time in her life.
Around 1–2% of women have recurrent miscarriages. In Australia this is when someone has three or more miscarriages with no pregnancy in between.
Australia has one of the lowest rates of stillbirth in the world. The rate has been relatively steady over the past 20 years at 0.7% or around seven per 1,000 pregnancies.
Who’s at risk?
Someone who has already had a miscarriage or stillbirth has an increased risk of that outcome again in a subsequent pregnancy.
Compared with women who have had a live birth, those who have had a stillbirth have double the risk of another. For those who have had recurrent miscarriages, the risk of another miscarriage is four-fold higher.
Some factors have a u-shaped relationship, with the risk of miscarriage and stillbirth lowest in the middle.
For instance, maternal age is a risk factor for both miscarriage and stillbirth, especially if under 20 years old or older than 35. Increasing age of the male is only a risk factor for stillbirth, especially for fathers over 40.
An older dad can be a risk factor for stillbirth, but not miscarriage. Elizaveta Galitckaia/Shutterstock Similarly for maternal bodyweight, women with a body mass index or BMI in the normal range have the lowest risk of miscarriage and stillbirth compared with those in the obese or underweight categories.
Lifestyle factors such as smoking and heavy alcohol drinking while pregnant are also risk factors for both miscarriage and stillbirth.
So it’s important to not only avoid smoking and alcohol while pregnant, but before getting pregnant. This is because early in the pregnancy, women may not know they have conceived and could unwittingly expose the developing fetus.
Why do they happen?
Miscarriage often results from chromosomal problems in the developing fetus. However, genetic conditions or birth defects account for only 7-14% of stillbirths.
Instead, stillbirths often relate directly to pregnancy complications, such as a prolonged pregnancy or problems with the umbilical cord.
Maternal health at the time of pregnancy is another contributing factor in the risk of both miscarriage and stillbirths.
Chronic diseases, such as high blood pressure, diabetes, hypothyroidism (underactive thyroid), polycystic ovary syndrome, problems with the immune system (such as an autoimmune disorder), and some bacterial and viral infections are among factors that can increase the risk of miscarriage.
Similarly mothers with diabetes, high blood pressure, and untreated infections, such as malaria or syphilis, face an increased risk of stillbirth.
In many cases, however, the specific cause of pregnancy loss is not known.
How about the long-term health risks?
Miscarriage and stillbirth can be early indicators of health issues later in life.
For instance, women who have had recurrent miscarriages or recurrent stillbirths are at higher risk of cardiovascular disease (such as heart disease or stroke).
Our research has also looked at the increased risk of stroke. Compared with women who had never miscarried, we found women with a history of three or more miscarriages had a 35% higher risk of non-fatal stroke and 82% higher risk of fatal stroke.
Women who had a stillbirth had a 31% higher risk of a non-fatal stroke, and those who had had two or more stillbirths were at a 26% higher risk of a fatal stroke.
We saw similar patterns in chronic obstructive pulmonary disease or COPD, a progressive lung disease with respiratory symptoms such as breathlessness and coughing.
Our data showed women with a history of recurrent miscarriages or stillbirths were at a 36% or 67% higher risk of COPD, respectively, even after accounting for a history of asthma.
Long-term health risks of recurrent miscarriages or stillbirths include developing lung disease later in life. PRPicturesProduction/Shutterstock Why is all this important?
Being well-informed about the similarities and differences between these two traumatic life events may help explain what has happened to you or a loved one.
Where risk factors can be modified, such as smoking and obesity, this information can be empowering for individuals who wish to reduce their risk of miscarriage and stillbirth and make lifestyle changes before they become pregnant.
More information and support about miscarriage and stillbirth is available from SANDS and Pink Elephants.
Gita Mishra, Professor of Life Course Epidemiology, Faculty of Medicine, The University of Queensland; Chen Liang, PhD student, reproductive history and non-communicable diseases in women, The University of Queensland, and Jenny Doust, Clinical Professorial Research Fellow, School of Public Health, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Longevity Code – by Dr. Kris Verburgh
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Notwithstanding the subtitle claim of “secrets from the leading edge of science”, we’ll note up front that this book was published in 2015, and what was new then, isn’t now. However, what was new then is still important now, so we think the book merits attention just the same.
The book examines why certain creatures (like humans) seem programmed to grow old and die, and why others (few others, but enough to make a list) either simply do not age, or else do age but can become younger when they hit a certain point. If this is the first you’re hearing of biologically immortal creatures, we’ll mention: they can and do die, just, their cause of death is usually by being eaten. But on a cellular and structural level, they don’t age. They grow to maturity and then just stay that way until one day they get eaten (or fall to some similar external circumstance).
Tackling the question of “why do we age?” (not as a philosophical question, but rather as an engineering question) is important to tackle the critical question of “…and could we not?”, and that’s what much of this book is about.
The real reason that compared to other mammals, humans live (for example) slightly longer than bats but not as long as naked mole rats, comes down mostly to genes, which makes it sound like things are set in stone, but rather, even without outright gene-editing technologies like CRISPR, gene expression is often quite modifiable, and often modifiable not just by drugs, but also by supplements, and indeed by nutraceuticals, which means also by diet, plus diet-adjacent things like fasting.
While this is mostly an explanatory book rather than a how-to, there’s enough to make practical use of, and even a recipes section.
The style is very gripping pop-science—or at least, if you’re anything like this reviewer, you’ll find it a page-turner. While being light on citations as we go (not like some authors who will mark several citations per page, or in the extreme, for every declarative sentence made), there is a reassuring bibliography at the back.
Bottom line: if you’re interested in the “under the hood” of aging, then you will love this book.
Click here to check out The Longevity Code, and slow down the aging process to live well for longer!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: