Swordfish vs Tuna – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing swordfish to tuna, we picked the tuna.
Why?
Today in “that which is more expensive is not necessarily the healthier”…
Considering the macros first, swordfish has more than 8x more total fat, about 9x more saturated fat, and yes, more cholesterol. On the other hand, tuna has more protein. An easy win for tuna.
In terms of vitamins, swordfish has more of vitamins A, B5, D, and E, while tuna has more of vitamins B1, B2, B3, B6, and B12. A marginal win for tuna, unless you want to weight the other vitamins more heavily, in which case, more likely a tie, or maybe even an argument for swordfish if you have a particular vitamin deficiency on that side.
When it comes to minerals, swordfish has more calcium and zinc, while tuna has more iron, magnesium, manganese, phosphorus, potassium, and selenium. A clear win for tuna.
One other thing: they’re both very rich in mercury, and while tuna is bad for that, swordfish has nearly 3x as much.
In short, both have a good spread of vitamins and minerals, and both are quite tainted with mercury, but in relative terms, there’s a clear winner even before considering the very different macros, and the winner is tuna.
Want to learn more?
You might like to read:
Farmed Fish vs Wild Caught: Important Differences
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Antihistamines for Runny Nose?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small 😎
❝Do you have any articles about using Anti-Histamines? My nose seems to be running a lot. I don’t have a cold or any allergies that I know of. I tried a Nasal spray Astepro, but it doesn’t do much.?❞
Just for you, we wrote such an article yesterday in response to this question!
The Astepro that you tried, by the way, is a brand name of the azelastine we mentioned near the end, before we got to talking about systemic corticosteroids such as beclometasone dipropionate—this latter might help you if antihistamines haven’t, and if your doctor advises there’s no contraindication (for most people it is safe for there are exceptions, such as if you are immunocompromised and/or currently fighting some infection).
You can find more details on all this in yesterday’s article, which in case you missed it, can be found at:
Antihistamines’ Generation Gap: Are You Ready For Allergy Season?
Enjoy!
Share This Post
-

Prostate Health: What You Should Know
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Prostate Health: What You Should Know
We’re aware that very many of our readers are women, who do not have a prostate.
However, dear reader: if you do have one, and/or love someone who has one, this is a good thing to know about.
The prostate gland is a (hopefully) walnut-sized gland (it actually looks a bit like a walnut too), that usually sits just under the bladder.
See also: How to Locate Your Prostate*
*The scale is not great in these diagrams, but they’ll get the job done. Besides, everyone is different on the inside, anyway. Not in a “special unique snowflake” way, but in a “you’d be surprised how much people’s insides move around” way.
Fun fact: did you ever feel like your intestines are squirming? That’s because they are.
You can’t feel it most of the time due to the paucity of that kind of nervous sensation down there, but the peristaltic motion that they use to move food along them on the inside, also causes them push against the rest of your guts, on the outside of them. This is the exact same way that many snakes move about.
If someone has to perform an operation in that region, sometimes it will be necessary to hang the intestines on a special rack, to keep them in one place for the surgery.
What can go wrong?
There are two very common things that can go wrong with the prostate:
- Benign Prostate Hyperplasia (BPH), otherwise known as an enlarged prostate
- Prostate cancer
For most men, the prostate gland continues to grow with age, which is how the former comes about so frequently.
For everyone, due to the nature of the mathematics involved in cellular mutation and replication, we will eventually get cancer if something else doesn’t kill us first.
- Prostate cancer affects 12% of men overall, and 60% of men aged 60+, with that percentage climbing each year thereafter.
- Prostate cancer can look like BPH in the early stages (and/or, an enlarged prostate can turn cancerous) so it’s important to not shrug off the symptoms of BPH.
How can BPH be avoided/managed?
There are prescription medications that can help reduce the size of the prostate, including testosterone blockers (such as spironolactone and bicalutamide) and 5α-reductase inhibitors, such as finasteride. Each have their pros and cons:
- Testosterone-blockers are the heavy-hitters, and work very well… but have more potential adverse side effects (your body is used to running on testosterone, after all)
- 5α-reductase inhibitors aren’t as powerful, but they block the conversion of free testosterone to dihydrogen testosterone (DHT), and it’s primarily DHT that causes the problems. By blocking the conversion of T to DHT, you may actually end up with higher serum testosterone levels, but fewer ill-effects. Exact results will vary depending on your personal physiology, and what else you are taking, though.
There are also supplements that can help, including saw palmetto and pumpkin seed oil. Here’s a good paper that covers both:
We have recommended saw palmetto before for a variety of uses, including against BPH:
Too much or too little testosterone? This one supplement may fix that
You might want to avoid certain medications that can worsen BPH symptoms (but not actually the size of the prostate itself). They include:
- Antihistamines
- Decongestants
- Non-steroidal anti-inflammatory drugs (NSAIDs)
- Tricyclic antidepressants (most modern antidepressants aren’t this kind; ask your pharmacist/doctor if unsure)
You also might want to reduce/skip:
- Alcohol
- Caffeine
In all the above cases, it’s because of how they affect the bladder, not the prostate, but given their neighborliness, each thing affects the other.
What if it’s cancer? How do I know and what do I do?
The creator of the Prostate Specific Antigen (PSA) test has since decried it as “a profit-driven health disaster” that is “no better than a coin toss”, but it remains the first go-to of many medical services.
However, there’s a newer, much more accurate test, called the Prostate Screening Episwitch (PSE) test, which is 94% accurate, so you might consider asking your healthcare provider whether that’s an option:
The new prostate cancer blood test with 94 per cent accuracy
As for where to go from there, we’re out of space for today, but we previously reviewed a very good book about this, Dr. Patrick Walsh’s Guide to Surviving Prostate Cancer, and we highly recommend it—it could easily be a literal lifesaver.
Share This Post
-

Simply The Pits: These Underarm Myths!
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Are We Taking A Risk To Smell Fresh As A Daisy?

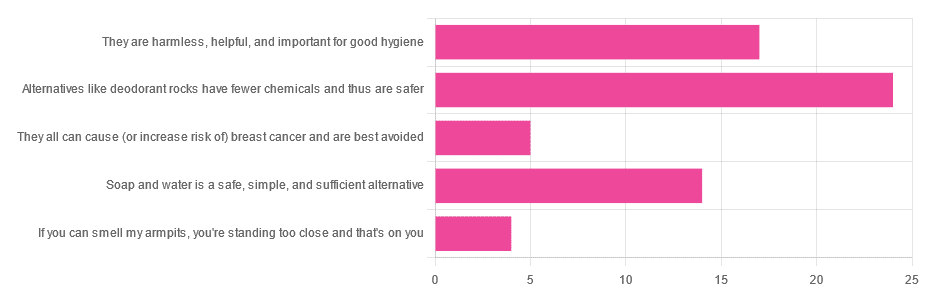
Yesterday, we asked you for your health-related view of underarm deodorants.
So, what does the science say?
They can cause (or increase risk of) cancer: True or False?
False, so far as we know. Obviously it’s very hard to prove a negative, but there is no credible evidence that deodorants cause cancer.
The belief that they do comes from old in vitro studies applying the deodorant directly to the cells in question, like this one with canine kidney tissues in petri dishes:
Antiperspirant Induced DNA Damage in Canine Cells by Comet Assay
Which means that if you’re not a dog and/or if you don’t spray it directly onto your internal organs, this study’s data doesn’t apply to you.
In contrast, more modern systematic safety reviews have found…
❝Neither is there clear evidence to show use of aluminum-containing underarm antiperspirants or cosmetics increases the risk of Alzheimer’s Disease or breast cancer.
Metallic aluminum, its oxides, and common aluminum salts have not been shown to be either genotoxic or carcinogenic.❞
(however, one safety risk it did find is that we should avoid eating it excessively while pregnant or breastfeeding)
Alternatives like deodorant rocks have fewer chemicals and thus are safer: True or False?
True and False, respectively. That is, they do have fewer chemicals, but cannot in scientific terms be qualifiably, let alone quantifiably, described as safer than a product that was already found to be safe.
Deodorant rocks are usually alum crystals, by the way; that is to say, aluminum salts of various kinds. So if it was aluminum you were hoping to avoid, it’s still there.
However, if you’re trying to cut down on extra chemicals, then yes, you will get very few in deodorant rocks, compared to the very many in spray-on or roll-on deodorants!
Soap and water is a safe, simple, and sufficient alternative: True or False?
True or False, depending on what you want as a result!
- If you care that your deodorant also functions as an antiperspirant, then no, soap and water will certainly not have an antiperspirant effect.
- If you care only about washing off bacteria and eliminating odor for the next little while, then yes, soap and water will work just fine.
Bonus myths:
There is no difference between men’s and women’s deodorants, apart from the marketing: True or False?
False! While to judge by the marketing, the only difference is that one smells of “evening lily” and the other smells of “chainsaw barbecue” or something, the real difference is…
- The “men’s” kind is designed to get past armpit hair and reach the skin without clogging the hair up.
- The “women’s” kind is designed to apply a light coating to the skin that helps avoid chafing and irritation.
In other words… If you are a woman with armpit hair or a man without, you might want to ignore the marketing and choose according to your grooming preferences.
Hopefully you can still find a fragrance that suits!
Shaving (or otherwise depilating) armpits is better for hygiene: True or False?
True or False, depending on what you consider “hygiene”.
Consistent with popular belief, shaving means there is less surface area for bacteria to live. And empirically speaking, that means a reduction in body odor:
However, shaving typically causes microabrasions, and while there’s no longer hair for the bacteria to enjoy, they now have access to the inside of your skin, something they didn’t have before. This can cause much more unpleasant problems in the long-run, for example:
❝Hidradenitis suppurativa is a chronic and debilitating skin disease, whose lesions can range from inflammatory nodules to abscesses and fistulas in the armpits, groin, perineum, inframammary region❞
Read more: Hidradenitis suppurativa: Basic considerations for its approach: A narrative review
And more: Hidradenitis suppurativa: Epidemiology, clinical presentation, and pathogenesis
If this seems a bit “damned if you do; damned if you don’t”, this writer’s preferred way of dodging both is to use electric clippers (the buzzy kind, as used for cutting short hair) to trim hers down low, and thus leave just a little soft fuzz.
What you do with yours is obviously up to you; our job here is just to give the information for everyone to make informed decisions whatever you choose 🙂
Take care!
Share This Post

Related Posts
-

Montana Eyes $30M Revamp of Mental Health, Developmental Disability Facilities
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
HELENA, Mont. — As part of a proposed revamping of the state’s behavioral health system, Republican Gov. Greg Gianforte’s administration is looking into moving a facility for people with developmental disabilities, beefing up renovations at the Montana State Hospital, and creating a Helena unit of that psychiatric hospital.
The changes, backers say, would fill gaps in services and help people better prepare for life outside of the locked, secure setting of the two state facilities before they reenter their own communities.
“I think part of the theme is responsibly moving people in and out of the state facilities so that we create capacity and have people in the appropriate places,” state Sen. Dave Fern (D-Whitefish) said of the proposed capital projects during a recent interview.
Fern served on the Behavioral Health System for Future Generations Commission, a panel created by a 2023 law to suggest how to spend $300 million to revamp the system. The law set aside the $300 million for improving state services for people with mental illness, substance abuse disorders, and developmental disabilities.
Gianforte’s proposed budget for the next two years would spend about $100 million of that fund on 10 other recommendations from the commission. The capital projects are separate ideas for using up to $32.5 million of the $75 million earmarked within the $300 million pool of funds for building new infrastructure or remodeling existing buildings.
The state Department of Public Health and Human Services and consultants for the behavioral health commission presented commission members with areas for capital investments in October. In December, the commission authorized state health department director Charlie Brereton to recommend the following projects to Gianforte:
- Move the 12-bed Intensive Behavior Center for people with developmental disabilities out of Boulder, possibly to either Helena or Butte, at an estimated cost of up to $13.3 million.
- Establish a “step-down” facility of about 16 beds, possibly on the campus of Shodair Children’s Hospital in Helena, to serve adults who have been committed to the Montana State Hospital but no longer need the hospital’s intensive psychiatric services.
- Invest $19.2 million to upgrade the Montana State Hospital’s infrastructure and buildings at Warm Springs, on top of nearly $16 million appropriated in 2023 for renovations already underway there in an effort to regain federal certification of the facility.
The state Architecture & Engineering Division is reviewing the health department’s cost estimates and developing a timeline for the projects so the information can be sent to the governor. Gianforte ultimately must approve the projects.
Health department officials have said they plan to take the proposals to legislative committees as needed. “With Commission recommendation and approval from the governor, the Department believes that it has the authority to proceed with capital project expenditures but must secure additional authority from the Legislature to fund operations into future biennia,” said department spokesperson Jon Ebelt.
The department outlined its facility plans to the legislature’s health and human services budget subcommittee on Jan. 22 as part of a larger presentation on the commission’s work and the 10 noncapital proposals in the governor’s budget. Time limits prevented in-depth discussion and public comment on the facility-related ideas.
One change the commission didn’t consider: moving the Montana State Hospital to a more populated area from its rural and relatively remote location near Anaconda, in southwestern Montana, in an attempt to alleviate staffing shortages.
“The administration is committed to continuing to invest in MSH as it exists today,” Brereton told the commission in October, referring to the Montana State Hospital.
The hospital provides treatment to people with mental illness who have been committed to the state’s custody through a civil or criminal proceeding. It’s been beset by problems, including the loss of federal Medicaid and Medicare funding due to decertification by the federal government in April 2022, staffing issues that have led to high use of expensive traveling health care providers, and turnover in leadership.
State Sen. Chris Pope (D-Bozeman) was vice chair of a separate committee that met between the 2023 and 2025 legislative sessions and monitored progress toward a 2023 legislative mandate to transition patients with dementia out of the state hospital. He agreed in a recent interview that improving — not moving — MSH is a top priority for the system right now.
“Right now, we have an institution that is failing and needs to be brought back into the modern age, where it is located right now,” he said after ticking off a list of challenges facing the hospital.
State Sen. John Esp (R-Big Timber) also noted at the October commission meeting that moving the hospital was likely to run into resistance in any community considered for a new facility.
Fern, the Whitefish senator, questioned in October whether similar concerns might exist for moving the Intensive Behavior Center out of Boulder. For more than 130 years, the town 30 miles south of Helena has been home, in one form or another, to a state facility for people with developmental disabilities. But Brereton said he believes relocation could succeed with community and stakeholder involvement.
The 12-bed center in Boulder serves people who have been committed by a court because their behaviors pose an immediate risk of serious harm to themselves or others. It’s the last residential building for people with developmental disabilities on the campus of the former Montana Developmental Center, which the legislature voted in 2015 to close.
Drew Smith, a consultant with the firm Alvarez & Marsal, told the commission in October that moving the facility from the town of 1,300 to a bigger city such as Helena or Butte would provide access to a larger labor pool, possibly allow a more homelike setting for residents, and open more opportunities for residents to interact with the community and develop skills for returning to their own communities.
Ideally, Brereton said, the center would be colocated with a new facility included in the governor’s proposed budget, for crisis stabilization services to people with developmental disabilities who are experiencing significant behavioral health issues.
Meanwhile, the proposed subacute facility with up to 16 beds for state hospital patients would provide a still secure but less structured setting for people who no longer need intensive treatment at Warm Springs but aren’t yet ready to be discharged from the hospital’s care. Brereton told the commission in October the facility would essentially serve as a less restrictive “extension” of the state hospital. He also said the agency would like to contract with a company to staff the subacute facility.
Health department officials don’t expect the new facility to involve any construction costs. Brereton has said the agency believes an existing building on the Shodair campus would be a good spot for it.
The state began leasing the building Nov. 1 for use by about 20 state hospital patients displaced by the current remodeling at Warm Springs — a different purpose than the proposed subacute facility.
Shodair CEO Craig Aasved said Shodair hasn’t committed to having the state permanently use the building as the step-down facility envisioned by the agency and the commission.
But Brereton said the option is attractive to the health department now that the building has been set up and licensed to serve adults.
“It seems like a natural place to start,” he told the commission in December, “and we don’t mind that it’s in our backyard here in Helena.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
This article first appeared on KFF Health News and is republished here under a Creative Commons license.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Longevity for the Lazy – by Dr. Richard Malish
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There are some people who devote all their resources to longevity, which can become a full-time occupation, not to mention a very expensive endeavor. This book’s for those who want to get the best possible “bang for buck” by doing the things that have the most favorable cost:worth ratio.
Dr. Malish covers what can be done easily for personal longevity, as well as what technological advances can be enjoyed that those before us didn’t have as options. He also discusses the diseases that are most likely to kill us, and how to avoid those.
He preaches a proactive approach, but one that is simple and consistent and based in good science, and good statistics. Indeed, while he’s served 20 years as an army doctor and a cardiologist, he now works as a healthcare policy consultant, so he is well-placed to advise.
The style of the book is halfway between regular pop-science and a textbook; you can either read it cover-to-cover, or skim first though the key points, highlight boxes, summaries, and the like. He also provides a time-phased task list, for those who like things to be laid out like that.
Bottom line: this is a very good, methodical guide to living longer without making it a full-time occupation.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Is fluoride really linked to lower IQ, as a recent study suggested? Here’s why you shouldn’t worry
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Fluoride is a common natural element found in water, soil, rocks and food. For the past several decades, fluoride has also been a cornerstone of dentistry and public health, owing to its ability to protect against tooth decay.
Water fluoridation is a population-based program where a precise, small amount of fluoride is added to public drinking water systems. Water fluoridation began in Australia in the 1950s. Today more than 90% of Australia’s population has access to fluoridated tap water.
But a recently published review found higher fluoride exposure is linked to lower intelligence quotient (IQ) in children. So how can we interpret the results?
Much of the data analysed in this review is poor quality. Overall, the findings don’t give us reason to be concerned about the fluoride levels in our water supplies.

TinnaPong/Shutterstock Not a new controversy
Tooth decay (also known as caries or cavities) can have negative effects on dental health, overall health and quality of life. Fluoride strengthens our teeth, making them more resistant to decay. There is scientific consensus water fluoridation is a safe, effective and equitable way to improve oral health.
Nonetheless, water fluoridation has historically been somewhat controversial.
A potential link between fluoride and IQ (and cognitive function more broadly) has been a contentious topic for more than a decade. This started with reports from studies in China and India.
But it’s important to note these studies were limited by poor methodology, and water in these countries had high levels of natural fluoride when the studies were conducted – many times higher than the levels recommended for water fluoridation programs. Also, the studies did not control for other contaminants in the water supply.
Recent reviews focusing on the level of fluoride used in water fluoridation have concluded fluoride is not linked to lower IQ.
Despite this, some have continued to raise concerns. The United States National Toxicology Program conducted a review of the potential link. However, this review did not pass the quality assessment by the US National Academies of Sciences, Engineering and Medicine due to significant limitations in the conduct of the review.
The authors followed through with their study and published it as an independent publication in the journal JAMA Paediatrics last week. This is the study which has been generating media attention in recent days.
What the study did
This study was a systematic review and meta-analysis, where the researchers evaluated 74 studies from different parts of the world.
A total of 52 studies were rated as having a high risk of bias, and 64 were cross-sectional studies, which often can’t provide evidence of causal relationship.
Most of the studies were conducted in developing countries, such as China (45), India (12), Iran (4), Mexico (4) and Pakistan (2). Only a few studies were conducted in developed countries with established public water systems, where regular monitoring and treatment of drinking water ensures it’s free from contaminants.
The vast majority of studies were conducted in populations with high to very high levels of natural fluoride and without water fluoridation programs, where fluoride levels are controlled within recommended levels.
The study concluded there was an inverse association between fluoride levels and IQ in children. This means those children who had a higher intake of fluoride had lower IQ scores than their counterparts.
Water fluoridation programs reduce the occurrence of cavities. Drazen Zigic/Shutterstock Limitations to consider
While this review combined many studies, there are several limitations that cast serious doubt over its conclusion. Scientists immediately raised concerns about the quality of the review, including in a linked editorial published in JAMA.
The low quality of the majority of included studies is a major concern, rendering the quality of the review equally low. Importantly, most studies were not relevant to the recommended levels of fluoride in water fluoridation programs.
Several included studies from countries with controlled public water systems (Canada, New Zealand, Taiwan) showed no negative effects. Other recent studies from comparable populations (such as Spain and Denmark) also have not shown any negative effect of fluoride on IQ, but they were not included in the meta-analysis.
For context, the review found there was no significant association with IQ when fluoride was measured at less than 1.5mg per litre in water. In Australia, the recommended levels of fluoride in public water supplies range from 0.6 to 1.1 mg/L.
Also, the primary outcome, IQ score, is difficult to collect. Most included studies varied widely on the methods used to collect IQ data and did not specify their focus on ensuring reliable and consistent IQ data. Though this is a challenge in most research on this topic, the significant variations between studies in this review raise further doubts about the combined results.
No cause for alarm
Although no Australian studies were included in the review, Australia has its own studies investigating a potential link between fluoride exposure in early childhood and child development.
I’ve been involved in population-based longitudinal studies investigating a link between fluoride and child behavioural development and executive functioning and between fluoride and IQ. The IQ data in the second study were collected by qualified, trained psychologists – and calibrated against a senior psychologist – to ensure quality and consistency. Both studies have provided strong evidence fluoride exposure in Australia does not negatively impact child development.
This new review is not a reason to be concerned about fluoride levels in Australia and other developed countries with water fluoridation programs. Fluoride remains important in maintaining the public’s dental health, particularly that of more vulnerable groups.
That said, high and uncontrolled levels of fluoride in water supplies in less developed countries warrant attention. There are programs underway in a range of countries to reduce natural fluoride to the recommended level.
Loc Do, Professor of Dental Public Health, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: