Sunflower Oil vs Canola Oil – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing sunflower oil to canola oil, we picked the sunflower oil.
Why?
Sunflower oil is marketed as being higher in polyunsaturated fats, which it is, albeit not by much.
Canola oil has been linked to heart disease, while sunflower oil has a weaker association with same, to the point that it can even be heart-positive if used sparingly, on account of its lipids ratio of 64% monounsaturated, 28% polyunsaturated, 7% saturated.
However, it’s worth bearing in mind that this has generally been in epidemiological studies, so it’s not accounting for how the oils have been used. There is a difference between “I cook with canola oil daily” and it’s a stir-fry, and “I cook with canola oil daily” and it’s deep-fried everything. Randomized controlled trials, which invariably have small standardized doses for study purposes, have generally been more positive than “out in the real world” studies. So: a lot may depend on how you use them.
As seed oils, they are both sources of vitamin E, but you’d need to drink a cup of oil to get your daily dose, so please just eat some seeds (or nuts, or fruit, or something) instead. It can even be sunflower seeds if you like! Rapeseed* itself (the seed that canola oil is made from) isn’t really sold as a foodstuff, so that one’s less of an option.
*Fun fact: if you’re N. American and wondering what this “rapeseed” is, know that most of the rest of the Anglosphere calls canola oil “rapeseed oil”, as it’s made from rapeseed, which comes from a plant called rape, whose name is unrelated to the crime of the same name, and comes from rāpa, the Latin word for turnip. Anyway, “canola” is a portmanteau of “Canadian” and “Ola” meaning oil, and is a trademark that has made its way into generic use throughout N. America, as a less alarming name.
Back to health matters: while sunflower seeds are healthy in moderation, the ultraprocessed and refined sunflower and canola oils cannot reasonably be described as a good choice if there’s a better oil available (which is: most cooking oils, honestly).
Canola oil has also been found to be implicated in age-related cognitive decline, whereas sunflower oil has had mixed results in that regard.
In summary
Sunflower oil is relatively healthier than canola oil. Please use a healthier oil than either if you can! Olive oil is good for most things, and if you need something with a higher smoke point (and/or less distinctive flavor), consider avocado oil, which is also very healthy and whose smoke point is even higher than the seed oils we’ve been discussing today.
Want to know more?
Check out:
Avocado Oil vs Olive Oil – Which is Healthier?
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Have You Tried Cannabis Terpenes (not THC or CBD!) vs Pain?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve previously covered such topics as Do CBD Gummies Work? and How Effective Is THC Against Chronic Pain?, as well as more general perspectives along the lines of Do “Natural” Painkillers Really Work?, but what of these newly-examined cannabis compounds that are neither CBD nor THC, but may well work against pain, including fibromyalgia pain that often quite little will touch?
Fibromyalgia is generally a good test of whether a pain relief method will work, independent of treating the cause—precisely because fibromyalgia is, when we look at it through a more critical lens, basically “pain that the doctors weren’t able to attribute to anything else”.
In this way, yes, that does also mean that fibromyalgia is less of a useful diagnosis and more of a rubber stamp, much like the role historically often fulfilled by “heart failure” as an official cause of death (because certainly, that heart sure did stop beating). It’s a way of answering the question without answering the question.
It’s what doctors write down when they’ve ruled out possible causes they’re aware of, and don’t want to admit they don’t know why your body is doing what it is.
It’s saying “I diagnose you with tired hurty syndrome, good luck, that’ll be [astonishing sum of dollars for the privilege of receiving this nothingburger answer] thank you”.
To be clear, while we are disparaging fibromyalgia as a useful diagnosis, we’re not dismissing the actual effect it has on people.
So while fibromyalgia has some potential use as a placeholder descriptor, it’s not an actionable answer, and it means that if that’s the diagnosis you’re handed, it can be beneficial to keep looking for the cause (because fibromyalgia is a result, not a cause).
For more on that, see: Why Fibromyalgia Is Not An Acceptable Diagnosis (and what to look for instead)
With that in mind, let’s get on to…
Terpenes, pain, & you
Researchers (Dr. Alyssa Welborn et al.) found that four cannabis-derived terpenes* reduced post-surgical pain and fibromyalgia pain without relying on THC, the main psychoactive component of cannabis, or for that matter, CBD.
*Namely:
- geraniol
- linalool
- β-caryophyllene
- α-humulene
How they appear to work: the pain-relieving effects were blocked by istradefylline, a drug that blocks the adenosine A2A receptor, indicating that activation of this receptor is likely the mechanism of action for the terpenes’ effects.
You may be wondering: what actually are terpenes? Terpenes are aromatic compounds found in cannabis and many other plants, that contribute to their smell and flavor, and no, they don’t produce the “high” associated with THC.
So, this is all sounding pretty good so far.
Any downsides?
In a mouse model experiment, the terpenes didn’t reduce responses in a hot-plate test that measures acute pain, supporting the researchers’ earlier conclusion that terpenes appear more effective for chronic or pathological pain than for immediate injury-related pain.
However, even that isn’t entirely a downside. After all, we’ve evolved acute pain responses for a reason, and that reason is to keep us safe. Where our evolutionary responses go screwy is when it comes to chronic pain, in which case it’s often a matter of our pain pathways misfiring and/or getting caught in an unhelpful feedback loop.
You can read the latest paper in full, here: Select terpenes from Cannabis sativa are antinociceptive in mouse models of post-operative pain and fibromyalgia via adenosine A2a receptors
Want to learn more?
We’ve written quite a bit about pain management, including:
- Before You Reach For That Tylenol…
- How To Stop Pain Spreading
- How To Dial Down Your Pain
- Managing Chronic Pain (Realistically!)
- Get The Right Help For Your Pain
- The 7 Approaches To Pain Management
- Science-Based Alternative Pain Relief (When Painkillers Aren’t Helping, These Things Might)
Take care!
Share This Post
-
Do You Have Anosognosia?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.

This is Dr. Ian McDonough. He’s a postdoctoral neuroscience research fellow and psychology professor, specializing in episodic memory, aging, and biomarkers of pre-clinical Alzheimer’s disease.
What does he want us to know?
As we get older, most of us tend to have fairly accurate perceptions of our financial abilities, and this awareness tends to improve with age and experience—until cognitive decline begins.
This was brought to light by a study he led, that analyzed 10 years of data from 2,802 older adults (age 65+). Participants rated their perceived ability in tasks like making change and paying bills, then performed actual financial tasks to test their competence.
Older adults in their 70s were better able to predict their financial performance than younger “older adults”, which the researchers noted was probably because…
❝It does seem people get better with time. So, by the time you get to your 70s, as long as you maintain your cognition decently well, you’re able to predict your financial ability slightly better. It’s almost like you do learn as you get more and more experience, especially as you retire, and you’re dealing with Social Security, Medicaid, Medicare and all those types of things that have to do with finances.❞
~ Dr. Ian McDonough
However! Cognitive decline disrupts this accuracy; people with cognitive decline (especially if progressing to dementia) often lose insight into their financial abilities, believing they’re more competent than they are—due to a condition called anosognosia, where one is unaware of one’s own cognitive impairment.
Which is reasonable, really. The very mental faculties that would normally clue us in to noticing our decline in a certain area, have been hit by the cognitive decline too.
This becomes a problem, because it then leaves people more vulnerable to suffering financial losses, either by maladministration of their affairs, or by falling prey to scams.
You can find the paper here: Relationship Between Perceived and Objective Financial Abilities Among Older Adults: Results From the Advanced Cognitive Training for Independent and Vital Elderly Cohort
What should we do about it?
According to Dr. McDonough,
❝Our research suggests that there is a critical window of time after people begin to experience cognitive decline during which they are still aware of their financial abilities. We believe that this is when people can take action to secure their finances and develop systems to protect themselves from fraud❞
We wrote about this a little before, in the context of planning around an Alzheimer’s diagnosis: Alzheimer’s: The Bad News And The Good
We also covered the topic of a “Living Will”, to enact if you are no longer considered able to advocate for yourself, here: Managing Your Mortality: When Planning Is a Matter of Life and Death ← while the title does not herald a cheerful prognosis, we promise we do also talk about living wills and such too!
This may particularly important in people with Parkinson’s disease, because of The Meds That Impair Decision-Making
Delegating to others is an obvious (and often reasonable) solution, but it can come with problems, because of such things as:
- Transitions in financial autonomy and risk for financial elder abuse, and
- Coping with Age-related Threats to Role Identity: Older Couples and the Management of Household Money
However, there are other options! For example:
Short version: it works! You can read a pop-science rendering of things, here:
Wondering how good your cognitive abilities are, and what that means in terms of dementia risk?
It’s actually quite identifiable, if one knows what things “count” and what things don’t:
Is It Dementia? Spot The Signs (Because None Of Us Are Immune)
Take care!
Share This Post
-
10 Unexpected Benefits Of Slow Jogging
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Sometimes, less is more:
Slow and steady wins the race?
Here’s the rundown… Slowly:
- You burn more body fat: running at 50-60% of max heart rate primarily burns fat without having the usual compensatory metabolic slump afterwards, unless you go for a very long time.
- You can build more muscle: lower-intensity workouts improve muscle recovery, which is essential too.
- You can reduce muscle soreness: light jogging helps clear lactic acid faster (10almonds note: muscle soreness after exercise isn’t about lactic acid)
- You avoid injuries: less impact on joints reduces injury risk.
- You learn the proper form: running slowly allows better focus on technique.
- You can enjoy it more: slower pace lets you take in surroundings and boosts mood.
- You still improve your cardiorespiratory fitness: strengthens heart and lungs over time.
- You’ll burn more calories than you think: can burn 200–400 calories per 30 minutes.
- You’ll improve your mobility: gentle movement supports joint health and collagen production.
- You can improve your performance: builds endurance and strength for faster running
For more on each of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Take care!
Share This Post




Related Posts
-

The Bitter Truth About Coffee (or is it?)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The Bitter Truth About Coffee (or is it?)

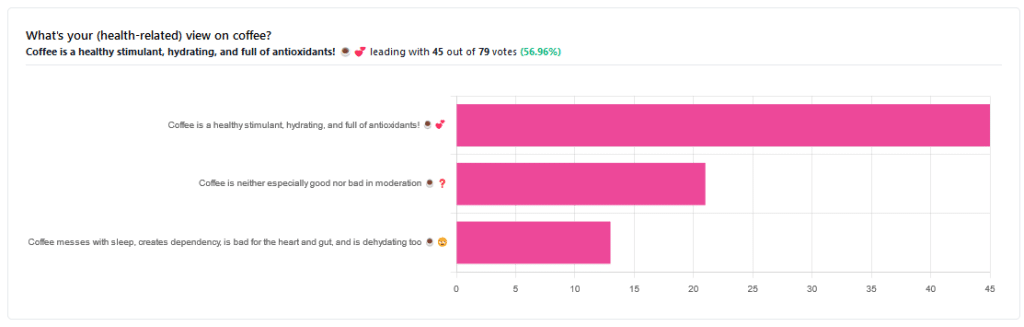
Yesterday, we asked you for your (health-related) views on coffee. The results were clear: if we assume the responses to be representative, we’re a large group of coffee-enthusiasts!
One subscriber who voted for “Coffee is a healthy stimulant, hydrating, and full of antioxidants” wrote:
❝Not so sure about how hydrating it is! Like most food and drink, moderation is key. More than 2 or 3 cups make me buzz! Just too much.❞
And that fine point brings us to our first potential myth:
Coffee is dehydrating: True or False?
False. With caveats…
Coffee, in whatever form we drink it, is wet. This may not come as a startling revelation, but it’s an important starting point. It’s mostly water. Water itself is not dehydrating.
Caffeine, however, is a diuretic—meaning you will tend to pee more. It achieves its diuretic effect by increasing blood flow to your kidneys, which prompts them to release more water through urination.
See: Effect of caffeine on bladder function in patients with overactive bladder symptoms
How much caffeine is required to have a diuretic effect? About 4.5 mg/kg.
What this means in practical terms: if you weigh 70kg (a little over 150lbs), 4.5×70 gives us 315.
315mg is about how much caffeine might be in six shots of espresso. We say “might” because while dosage calculations are an exact science, the actual amount in your shot of espresso can vary depending on many factors, including:
- The kind of coffee bean
- How and when it was roasted
- How and when it was ground
- The water used to make the espresso
- The pressure and temperature of the water
…and that’s all without looking at the most obvious factor: “is the coffee decaffeinated?”
If it doesn’t contain caffeine, it’s not diuretic. Decaffeinated coffee does usually contain tiny amounts of caffeine still, but with nearer 3mg than 300mg, it’s orders of magnitude away from having a diuretic effect.
If it does contain caffeine, then the next question becomes: “and how much water?”
For example, an Americano (espresso, with hot water added to make it a long drink) will be more hydrating than a ristretto (espresso, stopped halfway through pushing, meaning it is shorter and stronger than a normal espresso).
A subscriber who voted for “Coffee messes with sleep, creates dependency, is bad for the heart and gut, and is dehydrating too” wrote:
❝Coffee causes tachycardia for me so staying away is best. People with colon cancer are urged to stay away from coffee completely.❞
These are great points! It brings us to our next potential myth:
Coffee is bad for the heart: True or False?
False… For most people.
Some people, like our subscriber above, have an adverse reaction to caffeine, such as tachycardia. An important reason (beyond basic decency) for anyone providing coffee to honor requests for decaff.
For most people, caffeine is “heart neutral”. It doesn’t provide direct benefits or cause direct harm, provided it is enjoyed in moderation.
See also: Can you overdose on caffeine?
Some quick extra notes…
That’s all we have time for in myth-busting, but it’s worth noting before we close that coffee has a lot of health benefits; we didn’t cover them today because they’re not contentious, but they are interesting nevertheless:
- Coffee is the world’s biggest source of antioxidants
- 65% reduced risk of Alzheimer’s for coffee-drinkers
- 67% reduced risk of type 2 diabetes for coffee-drinkers
- 43% reduced risk of liver cancer for coffee-drinkers
- 53% reduced suicide risk for coffee-drinkers
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Celeriac vs Onion – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing celeriac to onion, we picked the celeriac.
Why?
In terms of macros, celeriac has slightly more fiber and protein, while onions have slightly more carbs, so this category is a nominal win for celeriac, but really it’s very close, so can just as easily be called a tie in this first round.
In the category of vitamins, celeriac has more of vitamins B1, B2, B3, B5, B6, B7, C, E, and K (in fact, 100x more vitamin K), while onions have more vitamin B9; an easy win for celeriac in this round.
Looking at minerals, celeriac has more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc, while onions are not higher in any minerals. Another overwhelming win for celeriac here.
Adding up the sections makes for a very clear overall win for celeriac, but by all means do enjoy either or both, as diversity is best!
Want to learn more?
You might like:
What’s Your Plant Diversity Score?
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
For people with ADHD, medication can reduce the risk of accidents, crime and suicide
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Attention-deficit hyperactivity disorder (ADHD) is a neurodevelopmental condition that affects around 7% of children and 2.5% of adults.
ADHD causes difficulties holding and sustaining attention over periods of time. People with ADHD also experience hyperactivity and high levels of impulsiveness and arousal. This can make it difficult to plan, coordinate and remain engaged in tasks.
ADHD is linked to problems at work, school and home, and to higher rates of mental illnesses such as anxiety. It’s also associated with higher rates of long-term harms.
Stimulant medication, such as methylphenidate and dexamphetamine, is the most common treatment for managing ADHD symptoms. Most people with ADHD will respond to at least one ADHD medication.
But, rising rates of prescriptions in recent years has prompted concern for their effectiveness and safety.
New research published today in the journal BMJ points to additional longer-term benefits. It found people with ADHD who took medication were less likely to have suicidal behaviours, transport accidents, issues with substance misuse, or be convicted of a crime.
What did the study do?
The study tracked 148,581 people who received a new diagnosis of ADHD between 2007 and 2018.
The authors used population-based data from Swedish national registers, including everyone aged six to 64 who was newly diagnosed with ADHD. The average age was 17.4 years and 41% were female.
Participants either started or did not start medication within three months of their ADHD diagnosis.
The authors examined the effects of drug treatment for ADHD on five critical outcomes: suicidal behaviours, substance misuse, accidental injuries, transport accidents and committing crime. They looked at both first-time and recurrent events.
This study used a method that uses data from health records or registries to mimic the design of a randomised controlled trial, in an attempt to reduce bias.
The researchers accounted for age, education, other mental and physical illnesses, prior history and use of other drugs, to account for factors that may influence results.
What did they find?
Within three months of receiving an ADHD diagnosis, 84,282 (56.7%) of people had started drug treatment for ADHD. Methylphenidate was the most commonly prescribed drug, accounting for 88.4% of prescriptions.
Drug treatment for ADHD was associated with reduced rates of a first occurrence for four out of the five outcomes: a 17% reduction for suicidal behaviours, 15% for substance misuse, 12% for transport accidents and 13% for committing crime.
When the researchers looked at people with recurrent events, the rate reductions associated with ADHD medication were seen for all five outcomes (including accidental injury).
The effect of medication was particularly strong when someone had a history of these events happening frequently. This means those with the most severe symptoms may benefit most.
Stimulant drugs were associated with lower rates of all five outcomes compared with non-stimulant drugs.
It’s likely these benefits are associated with improvements in attention, impulsivity and hyperactivity. People may be less likely to be distracted while driving, to self-medicate and show impacts from other mental health challenges.
What didn’t the study do?
The large sample size, use of national linked registers and sophisticated design give greater confidence that these findings are due to medication use and not due to other factors.
But the study was not able to examine medication dosages or track whether people reliably took their medication as prescribed. It also had no way to track the severity of ADHD symptoms. This means it can’t tell us if this helped most people or just some people with severe symptoms.
We know that ADHD medication helps most people, but it is not effective for everyone. So, we still need to understand why some people don’t benefit from ADHD medication, and what other treatments might also be helpful.
Finally, even though the study was rigorous in its design and adjusted for many factors, we can’t rule out that other unaccounted factors could be associated with these effects.
As prescribing increases, the size of the benefit decreases
A second study, published in June, used the same Swedish national registers and self-controlled case series design.
This study also concluded ADHD medication was associated with reduced risks for self-harm, accidental injuries, transport accidents and committing crime.
However, this study also showed that as prescribing rates increased nearly five-fold between years 2006 to 2020, the size of the observed benefits of ADHD medications reduced.
While remaining significant, the size of the associations between ADHD medication use and lower risks of unintentional injury, traffic crashes, and crime weakened over this time.
This could mean people who are less likely to need ADHD medications are now receiving them.
What are the impacts for patients and policymakers?
People need to know that if ADHD medications are helpful for them or their children, it might also improve many other areas of life.
These findings can also give governments confidence that their recent initiatives and efforts to increase access to ADHD support and treatment may have positive downstream impacts on broader social outcomes.
But medications aren’t the only ADHD treatment. Medication should only represent one part of a solution, with other psychological supports for managing emotional regulation, executive and organisational skills and problem-solving also beneficial.
Psychological therapies are effective and can be used in combination with, or separately to, medication.
Yet research shows drug treatments are relied on more frequently in more disadvantaged communities where it’s harder to access psychological supports.
Policymakers need to ensure medication does not become the only treatment people have access to. People with suspected ADHD need a high-quality diagnostic assessment to ensure they get the right diagnosis and the treatment most suitable for them.
Adam Guastella, Professor and Clinical Psychologist, Michael Crouch Chair in Child and Youth Mental Health, University of Sydney and Kelsie Boulton, Senior Research Fellow in Child Neurodevelopment, Brain and Mind Centre, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: