Some women’s breasts can’t make enough milk, and the effects can be devastating
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Many new mothers worry about their milk supply. For some, support from a breastfeeding counsellor or lactation consultant helps.
Others cannot make enough milk no matter how hard they try. These are women whose breasts are not physically capable of producing enough milk.
Our recently published research gives us clues about breast features that might make it difficult for some women to produce enough milk. Another of our studies shows the devastating consequences for women who dream of breastfeeding but find they cannot.
Some breasts just don’t develop
Unlike other organs, breasts are not fully developed at birth. There are key developmental stages as an embryo, then again during puberty and pregnancy.
At birth, the breast consists of a simple network of ducts. Usually during puberty, the glandular (milk-making) tissue part of the breast begins to develop and the ductal network expands. Then typically, further growth of the ductal network and glandular tissue during pregnancy prepares the breast for lactation.
But our online survey of women who report low milk supply gives us clues to anomalies in how some women’s breasts develop.
We’re not talking about women with small breasts, but women whose glandular tissue (shown in this diagram as “lobules”) is underdeveloped and have a condition called breast hypoplasia.
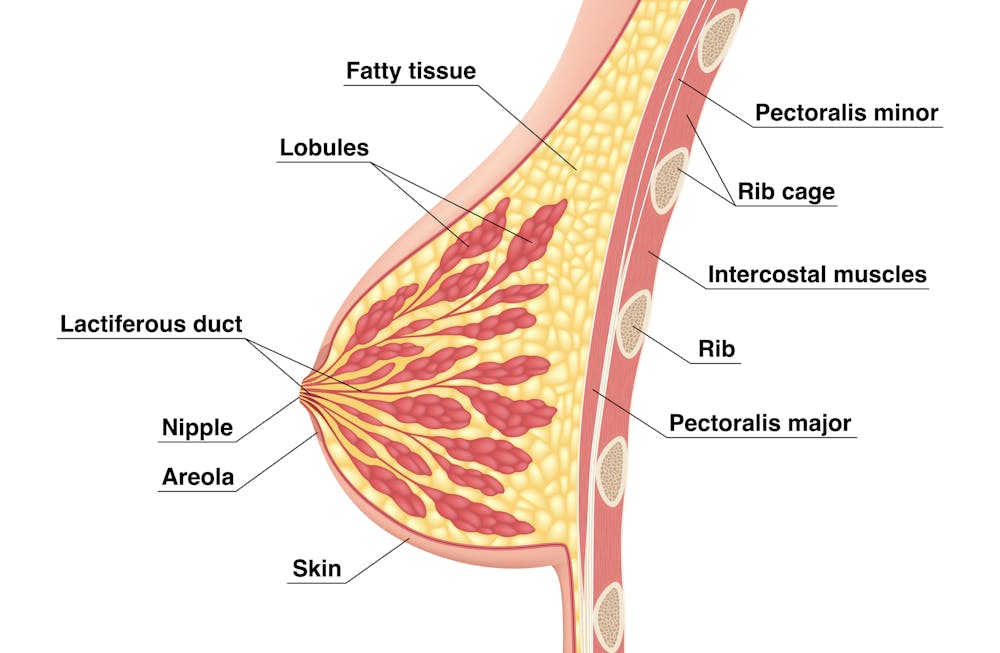
Tsuyna/Shutterstock
We don’t know how common this is. But it has been linked with lower rates of exclusive breastfeeding.
We also don’t know what causes it, with much of the research conducted in animals and not humans.
However, certain health conditions have been associated with it, including polycystic ovary syndrome and other endocrine (hormonal) conditions. A high body-mass index around the time of puberty may be another indicator.
Could I have breast hypoplasia?
Our survey and other research give clues about who may have breast hypoplasia.
But it’s important to note these characteristics are indicators and do not mean women exhibiting them will definitely be unable to exclusively breastfeed.
Indicators include:
- a wider than usual gap between the breasts
- tubular-shaped (rather than round) breasts
- asymmetric breasts (where the breasts are different sizes or shapes)
- lack of breast growth in pregnancy
- a delay in or absence of breast fullness in the days after giving birth
In our survey, 72% of women with low milk supply had breasts that did not change appearance during pregnancy, and about 70% reported at least one irregular-shaped breast.
The effects
Mothers with low milk supply – whether or not they have breast hyoplasia or some other condition that limits their ability to produce enough milk – report a range of emotions.
Research, including our own, shows this ranges from frustration, confusion and surprise to intense or profound feelings of failure, guilt, grief and despair.
Some mothers describe “breastfeeding grief” – a prolonged sense of loss or failure, due to being unable to connect with and nourish their baby through breastfeeding in the way they had hoped.
These feelings of failure, guilt, grief and despair can trigger symptoms of anxiety and depression for some women.

Bricolage/Shutterstock
One woman told us:
[I became] so angry and upset with my body for not being able to produce enough milk.
Many women’s emotions intensified when they discovered that despite all their hard work, they were still unable to breastfeed their babies as planned. A few women described reaching their “breaking point”, and their experience felt “like death”, “the worst day of [my] life” or “hell”.
One participant told us:
I finally learned that ‘all women make enough milk’ was a lie. No amount of education or determination would make my breasts work. I felt deceived and let down by all my medical providers. How dare they have no answers for me when I desperately just wanted to feed my child naturally.
Others told us how they learned to accept their situation. Some women said they were relieved their infant was “finally satisfied” when they began supplementing with formula. One resolved to:
prioritise time with [my] baby over pumping for such little amounts.
Where to go for help
If you are struggling with low milk supply, it can help to see a lactation consultant for support and to determine the possible cause.
This will involve helping you try different strategies, such as optimising positioning and attachment during breastfeeding, or breastfeeding/expressing more frequently. You may need to consider taking a medication, such as domperidone, to see if your supply increases.
If these strategies do not help, there may be an underlying reason why you can’t make enough milk, such as insufficient glandular tissue (a confirmed inability to make a full supply due to breast hypoplasia).
Even if you have breast hypoplasia, you can still breastfeed by giving your baby extra milk (donor milk or formula) via a bottle or using a supplementer (which involves delivering milk at the breast via a tube linked to a bottle).
More resources
The following websites offer further information and support:
- Australian Breastfeeding Association
- Lactation Consultants of Australia and New Zealand
- Royal Women’s Hospital, Melbourne
- Supply Line Breastfeeders Support Group of Australia Facebook support group
- IGT And Low Milk Supply Support Group Facebook support group
- Breastfeeding Medicine Network Australia/New Zealand
- Supporting breastfeeding grief (a collection of resources).
Shannon Bennetts, a research fellow at La Trobe University, contributed to this article.![]()
Renee Kam, PhD candidate and research officer, La Trobe University and Lisa Amir, Professor in Breastfeeding Research, La Trobe University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Natural Facelift – by Sophie Perry

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First, what this book isn’t: it’s mostly not about beauty, and it’s certainly not about ageist ideals of “hiding” aging.
The author herself discusses the privilege that is aging (not everyone gets to do it) and the importance of taking thankful pride in our lived-in bodies.
The title and blurb belie the contents of the book rather. Doubtlessly the publisher felt that extrinsic beauty would sell better than intrinsic wellbeing. As for what it’s actually more about…
Ever splashed your face in cold water to feel better? This book’s about revitalising the complex array of facial muscles (there are anatomical diagrams) and the often-tired and very diverse tissues that cover them, complete with the array of nerve endings very close to your CNS (not to mention the vagus nerve running just behind your jaw), and some of the most important blood vessels of your body, serving your brain.
With all that in mind, this book, full of useful therapeutic techniques, is a very, very far cry from “massage like this and you’ll look like you got photoshopped”.
The style varies, as some parts of explanation of principles, or anatomy, and others are hands-on (literally) guides to the exercises, but it is all very clear and easy to understand/follow.
Bottom line: aspects of conventional beauty may be a side-effect of applying the invigorating exercises described in this book. The real beauty is—literally—more than skin-deep.
Click here to check out The Natural Facelift, and order yours!
Share This Post
-

Eating Disorders: More Varied (And Prevalent) Than People Think
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Disordered Eating Beyond The Stereotypes
Around 10% of Americans* have (or have had) an eating disorder. That might not seem like a high percentage, but that’s one in ten; do you know 10 people? If so, it might be a topic that’s near to you.
*Source: Social and economic cost of eating disorders in the United States of Americ
Our hope is that even if you yourself have never had such a problem in your life, today’s article will help arm you with knowledge. You never know who in your life might need your support.
Very misunderstood
Eating disorders are so widely misunderstood in so many ways that we nearly made this a Friday Mythbusting edition—but we preface those with a poll that we hope to be at least somewhat polarizing or provide a spectrum of belief. In this case, meanwhile, there’s a whole cluster of myths that cannot be summed up in one question. So, here we are doing a Psychology Sunday edition instead.
“Eating disorders aren’t that important”
Eating disorders are the second most deadly category of mental illness, second only to opioid addiction.
Anorexia specifically has the highest case mortality rate of any mental illness:
Source: National Association of Anorexia Nervosa & Associated Disorders: Eating Disorder Statistics
So please, if someone needs help with an eating disorder (including if it’s you), help them.
“Eating disorders are for angsty rebellious teens”
While there’s often an element of “this is the one thing I can control” to some eating disorders (including anorexia and bulimia), eating disorders very often present in early middle-age, very often amongst busy career-driven individuals using it as a coping mechanism to have a feeling of control in their hectic lives.
13% of women over 50 report current core eating disorder symptoms, and that is probably underreported.
Source: as above; scroll to near the bottom!
“Eating disorders are a female thing”
Nope. Officially, men represent around 25% of people diagnosed with eating disorders, but women are 5x more likely to get diagnosed, so you can do the math there. Women are also 1.5% more likely to receive treatment for it.
By the time men do get diagnosed, they’ve often done a lot more damage to their bodies because they, as well as other people, have overlooked the possibility of their eating being disordered, due to the stereotype of it being a female thing.
Source: as above again!
“Eating disorders are about body image”
They can be, but that’s far from the only kind!
Some can be about control of diet, not just for the sake of controlling one’s body, but purely for the sake of controlling the diet itself.
Still yet others can be not about body image or control, like “Avoidant/Restrictive Food Intake Disorder”, which in lay terms sometimes gets dismissed as “being a picky eater” or simply “losing one’s appetite”, but can be serious.
For example, a common presentation of the latter might be a person who is racked with guilt and/or anxiety, and simply stops eating, because either they don’t feel they deserve it, or “how can I eat at a time like this, when…?” but the time is an ongoing thing so their impromptu fast is too.
Still yet even more others might be about trying to regulate emotions by (in essence) self-medicating with food—not in the healthy “so eat some fruit and veg and nuts etc” sense, but in the “Binge-Eating Disorder” sense.
And that latter accounts for a lot of adults.
You can read more about these things here:
Psychology Today | Types of Eating Disorder ← it’s pop-science, but it’s a good overview
Take care! And if you have, or think you might have, an eating disorder, know that there are organizations that can and will offer help/support in a non-judgmental fashion. Here’s the ANAD’s eating disorder help resource page, for example.
Share This Post
-

Cognitive Distortions: How To Stop Believing The Lies Your Brain Tells You
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Tracey Marks, psychiatrist, explains:
Unreliable narrator
You can’t reasonably trust everything you think! This is because your brain sometimes invents false alarms when faced with uncertainty, leading you to believe negative thoughts that aren’t consistent with external reality.
You may be wondering why it does this: the answer is that the brain uses shortcuts for efficiency, but under stress the amygdala (alarm system) overrides rational thinking from the prefrontal cortex, reinforcing negative loops through neuroplasticity.
Four common distortions:
- Catastrophizing (jumping to worst outcomes)
- All-or-nothing thinking (assuming mutually exclusive extremes)
- Mindreading (assuming others think negatively of you)
- Personalization (blaming yourself for things beyond your control).
During distorted thinking, the worry feels like realism, making them powerful and damaging if unquestioned.
What to do about it: pause and ask “what’s the evidence for this thought?” to separate facts from fears, as in the example of a delayed text reply.
Then, it’s good to practise self-compassion, and acknowledge distortions kindly instead of judging yourself, seeing them as clumsy attempts by the brain to protect you.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
CBT, DBT, & Radical Acceptance ← including what to do if you examine the evidence and conclude that your fears are, in fact, justified and probably correct
Take care!
Share This Post

-
Take Care Of Your “Unwanted” Parts Too!
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Meet The Family…
If you’ve heard talk of “healing your inner child” or similar ideas, then today’s featured type of therapy takes that to several extra levels, in a way that helps many people.
It’s called Internal Family Systems therapy, often “IFS” for short.
Here’s a quick overview:
Psychology Today | Internal Family Systems Therapy
Note: if you are delusional, paranoid, schizophrenic, or have some other related disorder*, then IFS would probably be a bad idea for you as it could worsen your symptoms, and/or play into them badly.
*but bipolar disorder, in its various forms, is not usually a problem for IFS. Do check with your own relevant healthcare provider(s), of course, to be sure.
What is IFS?
The main premise of IFS is that your “self” can be modelled as a system, and its constituent parts can be examined, questioned, given what they need, and integrated into a healthy whole.
For example…
- Exile is the name given to parts that could be, for example, the “inner child” referenced in a lot of pop-psychology, but it could also be some other ignored and pushed-down part of oneself, often from some kind of trauma. The defining characteristic of an exile is that it’s a part of ourself that we don’t consciously allow ourselves to see as a current part of ourself.
- Protector is the name given to a part of us that looks to keep us safe, and can do this in an adaptive (healthy) or maladaptive (unhealthy) way, for example:
- Firefighter is the name given to a part of us that will do whatever is necessary in the moment to deal with an exile that is otherwise coming to the surface—sometimes with drastic actions/reactions that may not be great for us.
- Manager is the name given to a part of us that has a more nurturing protective role, keeping us from harm in what’s often a more prophylactic manner.
To give a simple illustration…
A person was criticized a lot as a child, told she was useless, and treated as a disappointment. Consequently, as an adult she now has an exile “the useless child”, something she strives to leave well behind in her past, because it was a painful experience for her. However, sometimes when someone questions and/or advises her, she will get defensive as her firefighter “the hero” will vigorously speak up for her competence, like nobody did when she was a child. This vigor, however, manifests as rude abrasiveness and overcompensation. Finally, she has a manager, “the advocate”, who will do the same job, but in a more quietly confident fashion.
This person’s therapy will look at transferring the protector job from the firefighter to the manager, which will involve examining, questioning, and addressing all three parts.
The above example is fictional and created for simplicity and clarity; here’s a real-world case study if you’d like a more in-depth overview of how it can work:
How it all fits together in practice
IFS looks to make sure all the parts’ needs are met, even the “bad” ones, because they all have their functions.
Good IFS therapy, however, can make sure a part is heard, and then reassure that part in a way that effectively allows that part to “retire”, safe and secure in the knowledge that it has done what it needed to, and/or the job is being done by another part now.
That can involve, for example, thanking the firefighter for looking after our exile for all these years, but that our exile is safe and in good hands now, so it can put that fire-axe away.
See also: On Being Reactive vs Being Responsive
Questions you might ask yourself
While IFS therapy is best given by a skilled practitioner, we can take some of the ideas of it for self-therapy too. For example…
- What is a secret about yourself that you will take to the grave? And now, why did that part of you (now an exile) come to exist?
- What does that exile need, that it didn’t get? What parts of us try to give it that nowadays?
- What could we do, with all that information in mind, to assign the “protection” job to the part of us best-suited to healthy integration?
Want to know more?
We’ve only had the space of a small article to give a brief introduction to Family Systems therapy, so check out the “resources” tab at:
IFS Institute | What Is Internal Family Systems Therapy?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
How Your Emotions Affect GLP-1 Drug Results!
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
GLP-1 receptor agonist drugs (such as Ozempic, Wegovy, Mounjaro, and others) have a good reputation for working well, and the most talked-about downside is that they often have unpleasant side effects:
Most People Who Start GLP-1 RAs Quit Them Within A Year (Here’s Why) ← there are 4 main reasons
…and of course, some do work better than others: Better Than Ozempic?
As with almost any drug, some people are simply “non-responders”, meaning that for some reason (often a genetic factor, often not known for sure why), the drug will simply not work as it does for most people.
For GLP-1 receptor agonists, there is a portion of the general population for whom they simply will not work, and so far there is no known way of predicting it (probably at someone point it’ll be figured out, and this writer’s money would be on it being either a SNP mutation or a microbiome thing). So, you roll the dice, you take the GLP-1 drug, you wait and see, and there’s a 15% chance (that doesn’t sound like a lot, but it’s about 1 in 6, in other words, the same probability as rolling a “1” on a fair, six-sided die).
You can read about how that can go, here: Ozempic didn’t work for me. I was furious—and ashamed
But why?
The key is in why you are overeating in the first place (and if you’re looking to lose weight and/but are not overeating, then probably GLP-1 drugs are not for you, since that is primarily how they work).
In few words:
- If you are overeating in response to the sight and/or smell of tasty food, then probably you will benefit well from GLP-1 RAs in the long-term
- If you are overeating for emotional reasons (e.g. because of depression, or as a coping strategy to deal with stress/anxiety, for example) then probably GLP-1 RAs cannot be replied on to help you.
By “cannot be relied on” does not mean you will necessarily be a “non-responder” as described above, but it does mean that it’s likely your results will be intermittent at best. Which, after all, is not a big improvement on regular yo-yo dieting, an approach that is famously Not Good™.
Indeed, per the categories in the study we’re about to cite:
- Emotional eaters (eating due to negative feelings, not hunger) responded best to glp-1 drugs, showing greater weight loss and better blood sugar improvements
- External eaters (eating because food looks or smells appealing) were less likely to benefit in the long term
- Restrained eaters (deliberately restricting diet to lose weight) exercised more restraint temporarily, but returned to baseline by 12 months
Notably, all three categories of eaters here were people with type 2 diabetes—in other words, the very people that GLP-1 drugs were first developed to help, before they took off as weight-loss drugs.
So in theory, these should be the people for whom GLP-1 RAs work best—and yet, as we see, it’s still not always so, and is highly dependent on what goes on between one’s ears.
You can read this paper in full, here: Association between eating behavior patterns and the therapeutic efficacy of GLP-1 receptor agonists in individuals with type 2 diabetes: a multicenter prospective observational study
Want a different approach?
It is possible to get many of the effects of GLP-1 RAs without taking GLP-1 RAs, by enjoying foods that increase incretin, a hormone group (the most well-known of which is GLP-1) that slows down stomach emptying, which means a gentler blood sugar curve and feeling fuller for longer. It also acts on the hypothalamus, controlling appetite via the brain too (signalling fullness and reducing hunger).
For what foods to focus on, see: 5 Ways To Naturally Boost The “Ozempic Effect” ← this is from Dr. Jason Fung, who is perhaps most well-known for his work in functional medicine for reversing diabetes, and he’s once again giving us sound advice about metabolic hormone-hacking with dietary tweaks!
Or to curb emotional eating specifically, check out: Emotional Eating And The Five Pillars Of Craving Control
Or for a deeper dive, you might like this book we reviewed not long back:
Breaking Free from Emotional Eating – by Geneen Roth
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Celeriac vs Lettuce – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing celeriac to lettuce, we picked the lettuce.
Why?
In terms of macros, the celeriac has more fiber, carbs, and protein, making it the “more food per food” winning option in this category.
In the category of vitamins, celeriac has more of vitamins B3, B5, B6, and E, while lettuce has more of vitamins B1, B2, B9, and K, for a 4:4 tie here.
Looking at minerals, celeriac has more calcium, copper, magnesium phosphorus, potassium, selenium, and zinc, while lettuce has more iron and manganese, yielding a 7:2 win to celeriac.
In other considerations, celeriac has slightly more polyphenols, not a huge amount, but enough for a slender nominal win in this round too.
Adding up the sections makes for a clear overall win for celeriac, but by all means enjoy either or both, as diversity is good!
Want to learn more?
You might like:
Why You’re Probably Not Getting Enough Fiber (And How To Fix It)
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: