Semaglutide’s Surprisingly Unexamined Effects
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Semaglutide’s Surprisingly Big Research Gap
GLP-1 receptor agonists like Ozempic, Wegovy, and other semaglutide drugs. are fast becoming a health industry standard go-to tool in the weight loss toolbox. When it comes to recommending that patients lose weight, “Have you considered Ozempic?” is the common refrain.
Sometimes, this may be a mere case of kicking the can down the road with regard to some other treatment that it can be argued (sometimes even truthfully) would go better after some weight loss:
How weight bias in health care can harm patients with obesity: Research
…which we also covered in fewer words in the second-to-last item here:
But GLP-1 agonists work, right?
Yes, albeit there’s a litany of caveats, top of which are usually:
- there are often adverse gastrointestinal side effects
- if you stop taking them, weight regain generally ensues promptly
For more details on these and more, see:
…but now there’s another thing that’s come to light:
The dark side of semaglutide’s weight loss
In academia, “dark” is often used to describe “stuff we don’t have much (or in some cases, any) direct empirical evidence of, but for reasons of surrounding things, we know it’s there”.
Well-known examples include “dark matter” in physics and the Dark Ages in (European) history.
In the case of semaglutide and weight loss, a review by a team of researchers (Drs. Sandra Christenen, Katie Robinson, Sara Thomas, and Dominique Williams) has discovered how little research has been done into a certain aspect of GLP-1 agonist’s weight loss effects, namely…
Dietary changes!
There’s been a lot of popular talk about “people taking semaglutide eat less”, but it’s mostly anecdotal and/or presumed based on parts of the mechanism of action (increasing insulin production, reducing glucagon secretions, modulating dietary cravings).
Where studies have looked at dietary changes, it’s almost exclusively been a matter of looking at caloric intake (which has been found to be a 16–39% reduction), and observations-in-passing that patients reported reduction in cravings for fatty and sweet foods.
This reduction in caloric intake, by the way, is not significantly different to the reduction brought about by counselling alone (head-to-head studies have been done; these are also discussed in the research review).
However! It gets worse. Very few studies of good quality have been done, even fewer (two studies) actually had a registered dietitian nutritionist on the team, and only one of them used the “gold standard” of nutritional research, the 24-hour dietary recall test. Which, in case you’re curious, you can read about what that is here:
Dietary Assessment Methods: What Is A 24-Hour Recall?
Of the four studies that actually looked at the macros (unlike most studies), they found that on average, protein intake decreased by 17.1%. Which is a big deal!
It’s an especially big deal, because while protein’s obviously important for everyone, it’s especially important for anyone trying to lose weight, because muscle mass is a major factor in metabolic base rate—which in turn is much important for fat loss/maintenance than exercise, when it comes to how many calories we burn by simply existing.
A reasonable hypothesis, therefore, is that one of the numerous reasons people who quit GLP-1 agonists immediately put fat back on, is because they probably lost muscle mass in amongst their weight loss, meaning that their metabolic base rate will have decreased, meaning that they end up more disposed to put on fat than before.
And, that’s just a hypothesis and it’s a hypothesis based on very few studies, so it’s not something to necessarily take as any kind of definitive proof of anything, but it is to say—as the researchers of this review do loudly say—more research needs to be done into this, because this has been a major gap in research so far!
Any other bad news?
While we’re talking research gaps, guess how many studies looked into micronutrient intake changes in people taking GLP-1 agonists?
If you guessed zero, you guessed correctly.
You can find the paper itself here:
What’s the main take-away here?
On a broad, scoping level: we need more research!
On a “what this means for individuals who want to lose weight” level: maybe we should be more wary of this still relatively new (less than 10 years old) “wonder drug”. And for most of those 10 years it’s only been for diabetics, with weight loss use really being in just the past few years (2021 onwards).
In other words: not necessarily any need to panic, but caution is probably not a bad idea, and natural weight loss methods remain very reasonable options for most people.
See also: How To Lose Weight (Healthily!)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

5 Ways To Make Your Smoothie Blood Sugar Friendly (Avoid the Spike!)

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
At 10almonds, we are often saying “eat whole fruit; don’t drink your calories”. Whole fruit is great for blood sugars; fruit juices and many smoothies on the other hand, not so much. Especially juices, being near-completely or perhaps even completely stripped of fiber, but even smoothies have had a lot of the fiber broken down and are still a liquid, meaning they are very quickly and easily digestible, and thus their sugars (whatever carbs are in there) can just zip straight into your veins.
However, there are ways to mitigate this…
Slow it down
The theme here is “give the digestive process something else to do”; some things are more quickly and easily digestible than others, and if it’s working on breaking down some of the slower things, it’s not waving sugars straight on through; they have to wait their turn.
To that end, recommendations include:
- Full-fat Greek yogurt which provides both protein and fat, helping to slow down the absorption of sugar. Always choose unsweetened versions to avoid added sugars, though!
- Coconut milk (canned) which is low in sugar and carbs, high in fat. This helps reduce blood sugar spikes, as she found through personal experimentation too.
- Avocado which is rich in healthy fats that help stabilize blood sugar. As a bonus, it blends well into smoothies without affecting the taste much.
- Coconut oil which contains medium-chain triglycerides (MCTs) that are quickly absorbed for energy without involving glucose, promoting fat-burning and reducing blood sugar spikes.
- Collagen powder which is a protein that helps lower blood sugar spikes while also supporting muscle growth, skin, and joints.
For more on all of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Take care!
Share This Post
-
How To Get Strong Feet & Glutes (At The Same Time)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When it comes to whole-body musculoskeletal wellbeing and freedom from pain (especially when it comes to avoiding back pain), a remarkable lot depends on our feet and glutes.
So here’s how to help them to help the rest of your body:
A firm foundation
All physical goals—speed, strength, muscle growth, or skill—depend on good quality movement, which, in turn, depends on having a strong foundation.
The feet and glutes provide the physical base for movement. Specifically, the glutes and hips provide much of the movement’s strength and control, while the feet provide load-bearing directional support.
Standing barefoot on one leg tests both of these things. If you can’t balance for a minute or lose control during motion, your foundational stability is weak. This is, by the way, a reflection of functional strength— walking involves being on one leg 60–70% of the time, and running relies entirely on single-leg support, since at most one foot is on the ground at any given instant.
Common causes of weakness:
- For glutes: prolonged sitting shuts them off, tightens hip flexors, and leads to anterior pelvic tilt and atrophy. Without targeted training, everything in that general region of the body weakens.
- For feet: rigid, narrow shoes restrict motion, deform toe alignment, reduce foot stability, and create bunions. Shoes should be flexible and foot-shaped; spending more time barefoot is good too, which advice you might expect from a channel named “barefoot strength”.
Now, some exercises to improve strength in all the relevant parts:
- Squat-to-knee exercise: begin in a squat on your toes, move one knee outwards and lower it towards the ground, keeping the foot from collapsing. Then lift your hips by squeezing your glutes to feel a hip and quad stretch. This builds foot and glute strength together.
- Banded side-step variation: place a resistance band around your ankles (not knees) to raise glute activity by about 25%. This setup also challenges the arches to resist pronation, strengthening both your feet and glutes.
- Single-leg balance progression: start by balancing barefoot for a minute, then close your eyes to focus on just the physical feedback. Progress by adding hip hinges or hip rotations, ensuring motion comes from your hips, not your spine. Doing these on a narrow beam further intensifies foot engagement, but do stay safe, please, and only consider progressing to that if you’ve mastered the previous exercises, are feeling confident, and don’t have a pressing reason why falling would be catastrophic for you (e.g. osteoporosis or such). If in doubt, don’t do it.
For more on all of this plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
The Secret To Better Squats: Foot, Knee, & Ankle Mobility
Take care!
Share This Post
-

Activate Your Brain – by Scott G. Halford
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve reviewed a number of “improve your brain health” books over time, and this one’s quite different. How?
Most of the books we’ve reviewed have been focused on optimizing diet and exercise for brain health with a nod to other factors… This one focuses more on those other factors.
While this book does reference a fair bit of hard science, much of it is written more like a pop psychology book. As a result, most of the actionable advices, of which there are many, pertain to cognitive and behavioral adjustments.
And no, this is not a book of Cognitive Behavioral Therapy. It just happened to also address those two aspects.
We learn, for example, how our neurochemistry influences us—but also how we can influence our neurochemistry.
We also learn the oft-neglected (in other books!) social factors that influence brain health. Not just for our happiness, but for our productivity and peak cognitive performance too. Halford talks us through optimizing these such that we and those around us all get to enjoy the best brain benefits available to each of us.
The format of the book is that each chapter explains what you need to know for a given “activation” as the author calls it, and then an exercise to try out. With fifteen such chapters, every reader is bound to find at least something new.
Bottom line: if you want to grease those synapses in more ways than just eating some nuts and berries and getting good sleep and exercise, this book is a great resource.
Click here to check out “Activate Your Brain” and find your next level of cognitive performance!
Share This Post

Related Posts
-

Apple Cider Vinegar vs Apple Cider Vinegar Gummies – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing apple cider vinegar (bottled) to apple cider vinegar (gummies), we picked the bottled.
Why?
There are several reasons!
The first reason is about dosage. For example, the sample we picked for apple cider vinegar gummies, boasts:
❝2 daily chewable gummies deliver 800 mg of Apple Cider Vinegar a day, equivalent to a teaspoon of liquid apple cider vinegar❞
That sounds good until you note that it’s recommended to take 1–2 tablespoons (not teaspoons) of apple vinegar. So this would need more like 4–8 gummies to make the dose. Suddenly, either that bottle of gummies is running out quickly, or you’re just not taking a meaningful dose and your benefits will likely not exceed placebo.
The other is reason about sugar. Most apple cider vinegar gummies are made with some kind of sugar syrup, often even high-fructose corn syrup, which is one of the least healthy foodstuffs (in the loosest sense of the word “foodstuffs”) known to science.
The specific brand we picked today was the best we can find; it used maltitol syrup.
Maltitol syrup, a corn derivative (and technically a sugar alcohol), has a Glycemic Index of 52, so it does raise blood sugars but not as much as sucrose would. However (and somewhat counterproductive to taking apple cider vinegar for gut health) it can cause digestive problems for many people.
And remember, you’re taking 4–8 gummies, so this is amounting to several tablespoons of the syrup by now.
On the flipside, apple cider vinegar itself has two main drawbacks, but they’re much less troublesome issues:
- many people don’t like the taste
- its acidic nature is not good for teeth
To this the common advice for both is to dilute it with water, thus diluting the taste and the acidity.
(this writer shoots hers from a shot glass, thus not bathing the teeth since it passes them “without touching the sides”; as for the taste, well, I find it invigorating—I do chase it with water, though to be sure of not leaving vinegar in my mouth)
Want to check them out for yourself?
Here they are:
Apple cider vinegar | Apple cider vinegar gummies
Want to know more about apple cider vinegar?
Check out:
- An Apple (Cider Vinegar) A Day…
- 10 Ways To Balance Blood Sugars
- How To Recover Quickly From A Stomach Bug
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Don’t Get Caught Out By These “Nontraditional” Stroke Risk Factors
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Some stroke risk factors are modifiable (meaning: we can do something about them); others, not so much.
So let’s do a quick rundown of the main ones:
Modifiable risk factors
- High blood pressure (hypertension): the single most important risk factor for stroke.
- Smoking: bad for everything and this is no different; smoking damages blood vessels, which significantly increases stroke risk.
- Diabetes: high blood sugars can damage blood vessels too, cumulatively over time.
- High cholesterol: commonly leads to plaque buildup in arteries (atherosclerosis), which then creates hypertension, which we mentioned up top.
- Obesity: increases the risks of hypertension and diabetes, thus indirectly increasing stroke risk.
- Physical inactivity: again increases the risks of hypertension and diabetes, thus indirectly increasing stroke risk.
- Excessive alcohol use: once again increases the risks of hypertension and diabetes, thus indirectly increasing stroke risk.
- Poor diet: increases the risk of all of the above except for smoking (yes, poor diet also increases the risk of physical inactivity, since one who does not eat well will rarely exercise well).
Non-modifiable risk factors
- Age: risk increases significantly after age 55. Technically avoidable by dying young, but we don’t recommend that.
- Sex*: men have a higher risk of having a stroke, but women are more likely to die from it. So, not easy to escape this one.
- Family history: inheritable genetic factors seem to play a part, though this is not yet well-explored (there is no established “stroke gene”, for example).
- Ethnicity: most non-white populations have an increased stroke risk compared to white people—since this is based on US data, though, it’s unclear how much of this is due to genetic factors, and how much is due to structural racism (including: disparity of generational wealth/poverty) resulting in worse medical care.
- Previous stroke or TIA (transient ischemic attack): strong predictor of future strokes. It may seem a bit of a statement of the obvious that “the kind of person who has a stroke is the kind of person who is likely to have a stroke”, but it’d be remiss to not mention it.
*Ok, since the risk factors for sex are predicted based on hormones (which affect cardiovascular disease risk and thus, indirectly, stroke risk), technically this is modifiable, but we’ll bet very few people are going to trans their gender just to get the opposite stroke risk!
So what’s this about nontraditional risk factors?
Recent research looked at over 1,000 Europeans aged 18–49, approximately half of whom (523, to be precise) had experienced a cryptogenic ischemic stroke (that’s a fancy way of saying an ischemic stroke with no clear cause).
Specifically, they looked at the following “nontraditional” risk factors:
- Chronic multisystem disorder
- Inflammatory bowel disease
- Chronic kidney disease
- Chronic liver disease
- Autoimmune disease
- Hematologic disease or thrombophilia
- History of venous thrombosis
- History of malignancy
- Migraine with aura
- Current illicit drug use
Even more specifically, they weighed these against having (or not having) a congenital heart defect, a patent foramen ovale (PFO), colloquially called a “hole in the heart“. They found:
- Nontraditional risks had the strongest association with stroke in people with a PFO.
- Nevertheless, for those without a PFO, each nontraditional factor increased stroke risk by 70%, compared to a 41% increase per traditional risk factor.
- Female-centric risks outside of hormones (e.g. pregnancy complications, gestational diabetes) raised stroke risk by 70%, independently of other factors.
- Migraine with aura was the top nontraditional risk, accounting for 46% of strokes in PFO patients and 23% in those without.
You can read the paper itself here: Burden of Modifiable Risk Factors in Young-Onset Cryptogenic Ischemic Stroke by High-Risk Patent Foramen Ovale
Since migraines themselves are much-misunderstood, you might want to check out:
Migraine Mythbusting ← which also includes resources for managing this condition
Chronic kidney disease was also a top contender for increasing stroke risk, so check out:
Are your Kidneys Ok? Detect Early To Protect Kidney Health (Here’s How)
…and also:
Keeping Your Kidneys Healthy (Especially After 60) ← it’s about a lot more than just hydration!
Want to learn more?
Check out:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
A new treatment for Huntington’s disease is genuinely promising – but here’s why we still need caution
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Imagine knowing in your 20s or 30s that you carry a gene which will cause your mind and body to slowly unravel. Huntington’s disease is inherited, relentless and fatal, and there is no cure. Families live with the certainty of decline stretching across generations.
Now, a new treatment is being widely reported as a breakthrough.
Last week, gene therapy company uniQure announced that a one-time brain infusion appeared to slow the disease in a small clinical study.
If confirmed, this would not only be a landmark for Huntington’s disease but potentially the first time a gene therapy has shown promise in any adult-onset neurodegenerative disorder.
But the results, which were announced in a press release, are early, unreviewed and based on external comparisons. So, while these findings offer families hope after decades of failure, we need to remain cautious.

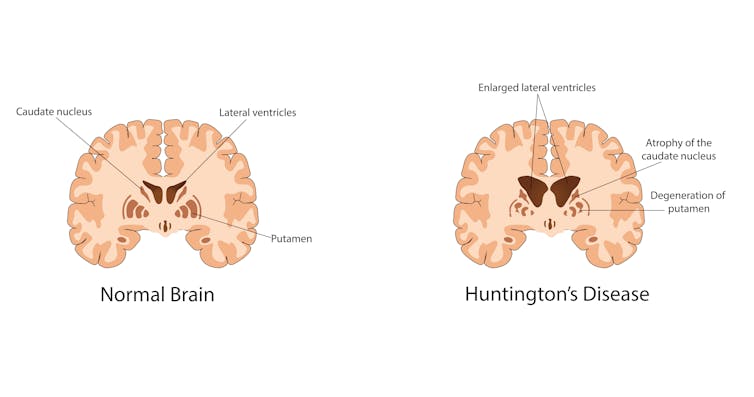
Krisada tepkulmanont/Getty What is Huntington’s disease?
Huntington’s is a rare but devastating disease, affecting around five to ten people in 100,000 in Western countries. That means thousands in Australia and hundreds of thousands worldwide.
Symptoms usually start in mid-life. They include involuntary movements, depression, irritability and progressive decline in thinking and memory. People lose the ability to work, manage money, live independently and eventually care for themselves. Most die ten to 20 years after onset.
The disease is caused by an expanded stretch of certain DNA repeats (CAG) in the huntingtin gene. The number of repeats strongly influences when symptoms begin, with longer expansions usually linked to earlier onset.
While rare, Huntington’s disease is inherited and fatal. Izuchukwu Onyeka/Getty Looking for a treatment
The gene that causes Huntington’s disease was identified in 1993, 32 years ago. Soon afterwards, mouse studies showed that switching off the mutant huntingtin protein even after symptoms had begun could reverse signs and improve behaviour.
This suggested lowering the toxic protein might slow or even partly reverse the disease. Yet for three decades, every attempt to develop a therapy for people has failed to show convincing clinical benefit. Trials of huntingtin-lowering drugs and other approaches did not slow progression.
What is the new treatment?
The one-time gene therapy, called AMT-130, involves brain surgery guided by MRI. Surgeons infuse an engineered virus directly into the caudate and putamen brain regions, which are heavily affected in Huntington’s.
The virus carries a short genetic “microRNA” designed to reduce production of the affected huntingtin protein.
By delivering it straight into the brain, the treatment bypasses the blood–brain barrier. This natural wall usually prevents medicines from entering the central nervous system. That barrier helps explain why so many brain-targeted drugs have failed.
What did they find?
Some 29 patients received treatment, with 12 in each group (one low-dose, and one high-dose) followed for three years. According to uniQure, those given the higher dose declined much slower than expected.
The study compared how much participants’ movement, thinking and daily function declined, compared to a matched external group from a global Huntington’s registry (meaning they weren’t part of the study). The company claimed those given the higher dose had a 75% slowing in their decline.
On a functional scale focused on independence, the company reported a 60% slowing in decline for the higher dose group.
Other tests of movement and thinking also favoured treatment. Nerve-cell damage in spinal fluid was lower for study participants than would be expected for untreated patients.
Why should we be cautious?
These findings are an early snapshot of results reported by the company, not yet peer-reviewed. The study compared treated patients to an external matched control group, not people randomised to placebo at the same time. This design can introduce bias. The numbers are also small – only 12 patients at the three-year mark – so we can’t draw solid conclusions.
The company reports the therapy was generally well tolerated, with no new serious adverse events related to the drug since late 2022. Most problems were related to the neurosurgical infusion itself, and resolved. But in a disease that already causes such severe symptoms, it is often hard to know what counts as a side effect.
The company uniQure has said it plans to seek regulatory approval in 2026 on the basis of this dataset.
Regulators will face difficult decisions: whether to allow access sooner before all the questions and uncertainties are addressed – based on the needs of a community with no effective options – and wait for further data while people are being treated, or to insist on larger trials that confirm results before approval.
What does it mean?
If upheld, these results represent the first convincing signs that a gene-targeted therapy can slow Huntington’s disease. They may also be the first evidence of benefit from a gene therapy in any adult-onset neurodegenerative disorder. That would be a milestone after decades of failure.
But these results do not prove success. Only larger, longer and fully peer-reviewed studies will show whether this treatment truly changes lives. Even if approved, a complex neurosurgical gene therapy may not be easily accessible to all patients.
The company has said the drug’s price would be similar to other gene therapies – which can cost over A$3 million per patient – and will have the added cost of brain surgery.
The takeaway
For families who carry this gene, the hope is profound. But caution is just as important.
We may be witnessing the first credible step toward slowing an inherited adult-onset neurodegenerative disease, or just an early signal that may not hold up.
Ultimately, only time and rigorous science will show whether this treatment delivers the benefits so urgently needed.
Bryce Vissel, Cojoint Professor, School of Clinical Medicine, UNSW Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: