Scrolling on the toilet increases your risk of haemorrhoids, new study shows
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Many of us are guilty of scrolling our smartphones on the toilet. But a new study from the United States, published today, has found this habit may increase your risk of developing haemorrhoids by up to 46%.
So, what’s the link? How can time on your phone lead to these painful lumps in and around your anus? Here’s what we know.

What are haemorrhoids?
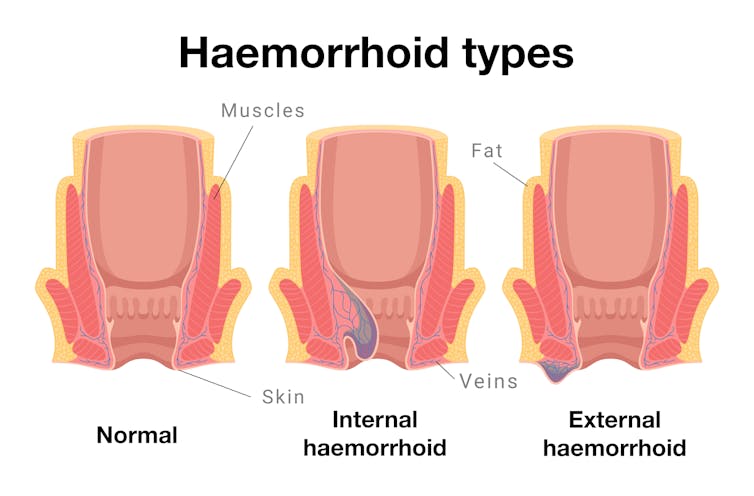
Every healthy person has haemorrhoids, sometimes called piles. They are columns of cushioned tissue and blood vessels found close to the opening of the anus.
Haemorrhoids have a really important role in maintaining bowel continence or, to put it simply, keeping your poo in.
When all is well, we don’t notice them. But haemorrhoids can get swollen and this can lead to symptoms such as pain, bleeding or feeling a lump just inside your anus (internal haemorrhoids) or protruding outside (external haemorrhoids).
So when someone “has haemorrhoids”, it means they have become inflamed or symptomatic.
This is extremely common: more than one in two of us will experience symptomatic haemorrhoids at some point in our lives.
You are more likely to get haemorrhoids if you:
- are older (over 45)
- are pregnant
- are overweight
- have persistent constipation or diarrhoea
- regularly lift heavy objects
- spend a lot of time on the toilet.
The link between toilet time and haemorrhoids
Prolonged sitting in general has not been linked to developing haemorrhoids.
However, a standard toilet seat – unlike a chair or couch – has a large internal opening that provides no support for the pelvic floor (the group of muscles and ligaments that support the bladder, bowel and uterus).
Prolonged sitting on a toilet seat is believed to increase pressure inside the pelvic floor and lead to blood pooling in the vascular cushions of the anus. This makes haemorrhoids more likely to develop.
What the new study looked at
The new US study recruited 125 adults, aged 45 and older, who were undergoing a colonoscopy at Beth Israel Deaconess Medical centre.
Researchers surveyed them about their smartphone habits while using the toilet, including how often they checked their phone and for how long. Participants also reported on other behaviours such as straining, their fibre intake, and how much physical activity they did.
The researchers recorded whether they had haemorrhoids. Since the participants were all having a colonoscopy, the presence of internal haemorrhoids could be directly confirmed visually.
What did the study show?
Two-thirds (66%) of all participants used smartphones while on the toilet. The most common activity was reading news (54.3%), followed by social media (44.4%).
Those who used their smartphones spent longer on the toilet than those who didn’t. More than one in three (37.3%) toilet smartphone users spent over five minutes on the toilet, compared to just over one in 20 (7%) of those who didn’t use their smartphones.
The smartphone users had a 46% higher risk of haemorrhoids, compared to those who didn’t use their smartphone. To calculate this, researchers took into account other known risk factors for haemorrhoids such as gender, age, body mass index, exercise activity, straining and fibre intake.
However, unlike some other research, this study did not find a link between straining and haemorrhoids.
As a result, the researchers concluded that time spent on the toilet poses a more significant risk for haemorrhoids than straining. However, we can’t rule out straining as a risk factor, based on one study.
Some other limitations to consider
The study relied on participants remembering whether or not they strained, and how long they spent on the toilet.
This kind of recall is subjective, and may also be influenced by taking part in the study. For example, if the participants thought they had haemorrhoids, they may be more likely to report straining.
The study’s small sample size and the participants’ age (all over 45) also mean it is unlikely to be representative of the broader population.
Toilet sitting time
The new study is not the first to study the link between time spent on the toilet and developing haemorrhoids. In 2020, a Turkish study found spending more than five minutes on the toilet was associated with haemorrhoids.
Another 2020 study from Italy of 52 people with diagnosed internal or external haemorrhoids noted the longer they spent on the toilet, the more severe their haemorrhoids.
So, what are we doing on the toilet?
Defaecation itself usually doesn’t take long. One study found it took healthy adults an average two minutes when sitting, but only 51 seconds when squatting.
The majority of “toilet sitting time” usually means just that – sitting on the toilet, doing other activities aside from pooing (or weeing).
One 2008 study from Israel surveyed 500 adults and found more than half (52.7%) read books or newspapers while on the toilet. It also found toilet readers spent significantly more time on the toilet.
How to avoid haemorrhoids
The usual advice is to increase the amount of fibre in your diet (eating more fruit, vegetables and wholegrains) and ensure you drink enough water. This makes it easier to pass a stool and reduces straining – which you should also try to avoid.
However, the new research confirms previous evidence that cutting down toilet sitting time may also help. So, avoiding distractions by leaving your smartphone outside the bathroom is a good idea (and as a bonus, will expose your device to fewer germs).
If you have any concerning symptoms, such as blood in your stool, a new lump in the anal region, or pain when passing a bowel motion then you should see your local doctor for further investigations and treatment.
Vincent Ho, Associate Professor and Clinical Academic Gastroenterologist, Western Sydney University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Tilapia vs Cod – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing tilapia to cod, we picked the tilapia.
Why?
Another case of “that which is more expensive is not necessarily the healthier”!
In terms of macros, tilapia has more protein and fats, as well as more omega-3 (and omega-6). On the downside, tilapia does have relatively more saturated fat, but at 0.94g/100g, it’s not exactly butter.
The vitamins category sees that tilapia has more of vitamins B1, B3, B5, B12, D, and K, while cod has more of vitamins B6, B9, and choline. A moderate win for tilapia.
When it comes to minerals, things are most divided; tilapia has more copper, iron, phosphorus, potassium, manganese, and selenium, while cod has more magnesium and zinc. An easy win for tilapia.
One other thing to note is that both of these fish contain mercury these days (and it’s worth noting: cod has nearly 10x more mercury). Mercury is, of course, not exactly a health food.
So, excessive consumption of either is not recommended, but out of the two, tilapia is definitely the one to pick.
Want to learn more?
You might like to read:
Farmed Fish vs Wild Caught: Know The Health Differences
Take care!
Share This Post
-
People with disability are dying from cancers we can actually prevent, our study shows
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
People with disability are missing out on screening programs that could help detect cancer early, and after diagnosis, are less likely to survive, our study shows.
Overall, this means people with disability are more likely to die from cancer than people without disability.
We draw together evidence showing the striking inequity at the heart of current approaches to controlling cancer.
But there are ways to improve access to the types of screening programs and cancer services many people without disability use routinely.

Chona Kasinger/Disabled and Here, CC BY-SA What we did and what we found
We reviewed evidence from 73 studies from around the world. These studies compared cancer outcomes in people with disability to those without.
Let’s start with cancer screening, one way to prevent deaths from cancer. Screening picks up early signs of cancer or can prevent it from developing into a problem if found early enough. Early detection usually means more treatment options and higher chances of a good outcome.
However, our review found people with disability are missing out on these life-saving screening programs all around the world, including for breast, cervical and bowel cancer.
In fact, some studies in our review showed these cancers are more likely to be diagnosed at an advanced stage in people with disability.
Once diagnosed, people with disability are still at a disadvantage. We found lower survival rates than cancer patients without disability.
This could be because of delayed diagnosis and inaccessible treatment, and we’d need further research to be sure. But we do have relevant evidence from some studies.
A UK study of cancer deaths in people with intellectual disability found more than a third had their cancer diagnosed after going to the emergency department. Almost half of the cancers in the study were already at an advanced stage when diagnosed.
Another review of global evidence found cancer patients with disability receive poorer quality cancer care. This included delays in treatment, being undertreated or having excessively invasive treatment. People with disability also had less access to in-hospital services and pain medication.
From diagnosis to treatment, global evidence shows people with disability are being excluded from health services that many people without disability routinely access and benefit from.
The situation is no different in Australia and it is costing lives.
In previous work, we found cancer is a leading cause of earlier deaths among Australians with disability. It’s the cause of about 20% of the extra deaths we see in people with disability compared to people without.
Why is this happening?
We clearly need to do more to improve health care for people with disability. But we also need to take action in other areas to address underlying issues.
People with disability are more likely to be poor and live in disadvantaged circumstances than the rest of the Australian population, which may put them at higher risk of cancer.
Many factors that cause cancer – for example, smoking, unaffordable healthy food, and drinking high levels of alcohol – disproportionately impact disadvantaged groups, including people with disability.
Many people with disability live with additional health conditions, which can lead to a lack of attention to routine issues. This can result in cancer screening and routine care becoming less of a priority.
Buildings where services are provided and medical diagnostic equipment is located are not always accessible for people with disability.
The health system itself can be inaccessible, with little support to help people with disability access services. For instance, navigating cancer care can be overwhelming, especially for people who need support for daily activities, transport or communication.
People with disability, especially with intellectual disability, need extra time and support to give informed consent to screening, treatment or procedures – resources and time particularly overstretched in public health systems.
People with disability can also experience both direct and indirect discrimination in health care, which lead to poorer outcomes. This includes discriminatory attitudes towards people with disability and their carers, and making assumptions about a patient based on their disability.
Health systems need to allow for extra time to get informed consent. Media_Photos/Shutterstock What can we do about it?
For cancer control to be inclusive and work for people with disability, we need to look at:
- prevention – public health interventions, such as quit smoking or healthy lifestyle programs, need to be co-designed with and tailored to people with disability
- early detection – national screening programs must develop strategies and take active steps to include people with disability. Clinics need to be physically accessible, information needs to be available in a range of accessible formats, and extra time needs to be allocated to get genuine informed consent
- ensuring people with disability have a voice – cancer care needs to be tailored to an individual person, as everyone’s needs are different. We need to support and include people with disability in conversations about their care so they can make informed decisions. This means providing information in ways that work for them, and allowing time to understand and ask questions
- training health professionals to understand and respond to the needs of people with disability and make the adjustments required for optimal cancer care, particularly for people with an intellectual disability.
Yi Yang, Research Fellow, Social Epidemiology, Melbourne Disability Institute, Melbourne School of Population and Global Health, The University of Melbourne; George Disney, Research Fellow, Social Epidemiology, The University of Melbourne, and Kirsten Deane, Deputy Director, Melbourne Disability Institute, The University of Melbourne
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-
Superfood Pesto Pizza
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Not only is this pizza full of foods that punch above their weight healthwise, there’s no kneading and no waiting when it comes to the base, either. Homemade pizzas made easy!
You will need
For the topping:
- 1 zucchini, sliced
- 1 red bell pepper, cut into strips
- 3 oz mushrooms, sliced
- 3 shallots, cut into quarters
- 6 sun-dried tomatoes, roughly chopped
- ½ bulb garlic (paperwork done, but cloves left intact, unless they are very large, in which case halve them)
- 1 oz pitted black olives, halved
- 1 handful arugula
- 1 tbsp extra virgin olive oil
- 2 tsp black pepper, coarse ground
- ½ tsp MSG or 1 tsp low-sodium salt
For the base:
- ½ cup chickpea flour (also called besan or gram flour)
- 2 tsp extra virgin olive oil
- ½ tsp baking powder
- ⅛ tsp MSG or ¼ tsp low-sodium salt
For the pesto sauce:
- 1 large bunch basil, chopped
- ½ avocado, pitted and peeled
- 1 oz pine nuts
- ¼ bulb garlic, crushed
- 2 tbsp nutritional yeast
- 1 tsp black pepper
- Juice of ½ lemon
Method
(we suggest you read everything at least once before doing anything)
1) Preheat the oven to 400℉ / 200℃.
2) Toss the zucchini, bell pepper, mushrooms, shallots, and garlic cloves in 1 tbsp olive oil, ensuring an even coating. Season with the black pepper and MSG/salt, and put on a baking tray lined with baking paper, to roast for about 20 minutes, until they are slightly charred.
3) When the vegetables are in the oven, make the pizza base by combining the dry ingredients in a bowl, making a pit in the middle of it, adding the olive oil and whisking it in, and then slowly (i.e., a little bit at a time) whisking in 1 cup cold water. This should take under 5 minutes.
4) Don’t panic when this doesn’t become a dough; it is supposed to be a thick batter, so that’s fine. Pour it into a 9″ pizza pan, and bake for about 15 minutes, until firm. Rotate it if necessary partway through; whether it needs this or not will depend on your oven.
5) While the pizza base is in the oven, make the pesto sauce by blending all the pesto sauce ingredients in a high-speed blender until smooth.
6) When the base and vegetables are ready (these should be finished around the same time), spread the pesto sauce on the base, scatter the arugula over it followed by the vegetables and then the olives and sun-dried tomatoes.
7) Serve, adding any garnish or other final touches that take your fancy.

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Which Bell Peppers To Pick? A Spectrum Of Specialties
- Ergothioneine In Mushrooms: “The Longevity Vitamin” (That’s Not A Vitamin)
- Black Olives vs Green Olives – Which is Healthier
- Lycopene’s Benefits For The Gut, Heart, Brain, & More
- Coconut vs Avocado – Which is Healthier?
- Herbs for Evidence-Based Health & Healing
- Spermidine For Longevity
Take care!
Share This Post





Related Posts
-
Are You Taking PIMs?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Getting Off The Overmedication Train
The older we get, the more likely we are to be on more medications. It’s easy to assume that this is because, much like the ailments they treat, we accumulate them over time. And superficially at least, that’s what happens.
And yet, almost half of people over 65 in Canada are taking “potentially inappropriate medications”, or PIMs—in other words, medications that are not needed and perhaps harmful. This categorization includes medications where the iatrogenic harms (side effects, risks) outweigh the benefits, and/or there’s a safer more effective medication available to do the job.
You may be wondering: what does this mean for the US?
Well, we don’t have the figures for the US because we’re working from Canadian research today, but given the differences between the two country’s healthcare systems (mostly socialized in Canada and mostly private in the US), it seems a fair hypothesis that if it’s almost half in Canada, it’s probably more than half in the US. Socialized healthcare systems are generally quite thrifty and seek to spend less on healthcare, while private healthcare systems are generally keen to upsell to new products/services.
The three top categories of PIMs according to the above study:
- Gabapentinoids (anticonvulsants also used to treat neuropathic pain)
- Proton pump inhibitors (PPIs)
- Antipsychotics (especially, to people without psychosis)
…but those are just the top of the list; there are many many more.
The list continues: opioids, anticholinergics, sulfonlyurea, NSAIDs, benzodiazepines and related rugs, and cholinesterase inhibitors. That’s where the Canadian study cuts off (although it also includes “others” just before NSAIDs), but still, you guessed it, there are more (we’re willing to bet statins weigh heavily in the “others” section, for a start).
There are two likely main causes of overmedication:
The side effect train
This is where a patient has a condition and is prescribed drug A, which has some undesired side effects, so the patient is prescribed drug B to treat those. However, that drug also has some unwanted side effects of its own, so the patient is prescribed drug C to treat those. And so on.
For a real-life rundown of how this can play out, check out the case study in:
The Hidden Complexities of Statins and Cardiovascular Disease (CVD)
The convenience factor
No, not convenient for you. Convenient for others. Convenient for the doctor if it gets you out of their office (socialized healthcare) or because it was easy to sell (private healthcare). Convenient for the staff in a hospital or other care facility.
This latter is what happens when, for example, a patient is being too much trouble, so the staff give them promazine “to help them settle down”, notwithstanding that promazine is, besides being a sedative, also an antipsychotic whose common side effects include amenorrhea, arrhythmias, constipation, drowsiness and dizziness, dry mouth, impotence, tiredness, galactorrhoea, gynecomastia, hyperglycemia, insomnia, hypotension, seizures, tremor, vomiting and weight gain.
This kind of thing (and worse) happens more often towards the end of a patient’s life; indeed, sometimes precipitating that end, whether you want it or not:
Mortality, Palliative Care, & Euthanasia
How to avoid it
Good practice is to be “open-mindedly skeptical” about any medication. By this we mean, don’t reject it out of hand, but do ask questions about it.
Ask your prescriber not only what it’s for and what it’ll do, but also what the side effects and risks are, and an important question that many people don’t think to ask, and for which doctors thus don’t often have a well-prepared smooth-selling reply, “what will happen if I don’t take this?”
And look up unbiased neutral information about it, from reliable sources (Drugs.com and The BNF are good reference guides for this—and if it’s important to you, check both, in case of any disagreement, as they function under completely different regulatory bodies, the former being American and the latter being British. So if they both agree, it’s surely accurate, according to best current science).
Also: when you are on a medication, keep a journal of your symptoms, as well as a log of your vitals (heart rate, blood pressure, weight, sleep etc) so you know what the medication seems to be helping or harming, and be sure to have a regular meds review with your doctor to check everything’s still right for you. And don’t be afraid to seek a second opinion if you still have doubts.
Want to know more?
For a more in-depth exploration than we have room for here, check out this book that we reviewed not long back:
To Medicate or Not? That is the Question! – by Dr. Asha Bohannon
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

It’s Not A Diet – by Davinia Taylor
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A lot of diet books claim “it’s not a diet”, even when the titles are things like “The Such-and-Such Diet”.
This time, we get to see the claim as the title itself, so, how does it measure up?
Honestly, we’ll agree it’s not a diet. Yes, there is nutritional advice, and nothing that will be too shocking to regular 10almonds readers. Avoid processed foods, get plenty of fruit and veg, skip the alcohol. She leans towards keto, but isn’t evangelical about it despite selling a line of keto products herself. All in all, it can be called dietary guidance, but not reasonably “a diet” in any meaningful sense of the word.
The only counterpoint is that there is, for those who like that sort of thing, a “two-week reset programme”, which we might consider a diet, given it is clearly prescriptive with its meal plan.
She also talks sleep, hydration, stress management, movement, and so forth. Again, nothing that will surprise the well-informed reader. So, what does this book have to offer that we’re not assuming knowledge of?
Informationally, very little. But inspirationally, rather more, and a lot is about integrating healthier changes into your life and making them actually stick—and that’s where the real value of the book lies.
The style is, as with her other book “Futureproof” that we reviewed all so recently, again very direct and personable, and/but has a normal British amount of casual swearing that might shock some American readers. There’s a lot less science in this book than her other one, so there’s no bibliography per se, just an “acknowledgements” section at the back.
Bottom line: if you know what you need to do but struggle more with actually doing it, this book can help with that.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Kindness Method – by Shahroo Izadi
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Shahroo Izadi here covers everything from alcohol addiction to procrastination to weight loss. It’s a catch-all handbook for changing your habits—in general, and/or in whatever area of your life you most feel you want or need to.
She herself went from yo-yo dieting to a stable healthy lifestyle, and wants to share with us how she did it. So she took what worked for her, organized and dilstilled it, and named it “the kindness method”, which…
- promotes positivity not in a “head in the sand” sense but rather: you have strengths, let’s find them and use them
- offers many exploratory exercises to help you figure out what’s actually going to be best for you
- plans support in advance—you’re going to be your own greatest ally here
Basically it’s about:
- being kind to yourself rather than setting yourself up to fail, and “judging a fish by how well it can climb a tree”
- being kind to yourself by being compassionate towards your past self and moving on with lessons learned
- being kind to yourself by getting things in order for your future self, because you need to treat your future self like a loved one
In fact, why not buy a copy of this book as a gift for your future self?
Click Here To Order Your Copy of “The Kindness Method” on Amazon Today!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: