Rewire Your OCD Brain – by Dr. Catherine Pittman & Dr. William Youngs
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
OCD is just as misrepresented in popular media as many other disorders, and in this case, it’s typically not “being a neat freak” or needing to alphabetize things, so much as having uncontrollable obsessive intrusive thoughts, and often in response to those, unwanted compulsions. This can come from unchecked spiralling anxiety, and/or PTSD, for example.
What Drs. Pittman & Young offer is an applicable set of solutions, to literally rewire the brain (insofar as synapses can be considered neural wires). Leveraging neuroplasticity to work with us rather than against us, the authors talk us through picking apart the crossed wires, and putting them back in more helpful ways.
This is not, by the way, a book of CBT, though it does touch on that too.
Mostly, the book explains—clearly and simply and sometimes with illustrations—what is going wrong for us neurologically, and how to neurologically change that.
Bottom line: whether you have OCD or suffer from anxiety or just need help dealing with obsessive thoughts, this book can help a lot in, as the title suggests, rewiring that.
Click here to check out Rewire Your OCD Brain, and banish obsessive thoughts!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Longevity for the Lazy – by Dr. Richard Malish

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There are some people who devote all their resources to longevity, which can become a full-time occupation, not to mention a very expensive endeavor. This book’s for those who want to get the best possible “bang for buck” by doing the things that have the most favorable cost:worth ratio.
Dr. Malish covers what can be done easily for personal longevity, as well as what technological advances can be enjoyed that those before us didn’t have as options. He also discusses the diseases that are most likely to kill us, and how to avoid those.
He preaches a proactive approach, but one that is simple and consistent and based in good science, and good statistics. Indeed, while he’s served 20 years as an army doctor and a cardiologist, he now works as a healthcare policy consultant, so he is well-placed to advise.
The style of the book is halfway between regular pop-science and a textbook; you can either read it cover-to-cover, or skim first though the key points, highlight boxes, summaries, and the like. He also provides a time-phased task list, for those who like things to be laid out like that.
Bottom line: this is a very good, methodical guide to living longer without making it a full-time occupation.
Share This Post
-

Benefits of Different Tropical Fruits
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝Would very much like your views of the benefits of different tropical fruits. I do find papaya is excellent for settling the digestion – but keen to know if others have remarkable qualities.❞
Definitely one for a main feature sometime soon! As a bonus while you wait, pineapple has some unique and powerful properties:
❝Its properties include: (1) interference with growth of malignant cells; (2) inhibition of platelet aggregation*; (3) fibrinolytic activity; (4) anti-inflammatory action; (5) skin debridement properties. These biological functions of bromelain, a non-toxic compound, have therapeutic values in modulating: (a) tumor growth; (b) blood coagulation; (c) inflammatory changes; (d) debridement of third degree burns; (e) enhancement of absorption of drugs.❞
*so do be aware of this if you are on blood thinners or otherwise have a bleeding disorder, as you might want to skip the pineapple in those cases!
Source: Bromelain, the enzyme complex of pineapple (Ananas comosus) and its clinical application. An update
Enjoy!
Share This Post
-

Beetroot Juice & Caffeine Work Better Than Either Alone
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Beetroot has many beneficial properties, which we’ve written about before:
Beetroot For More Than Just Your Blood Pressure
…and as for caffeine, it’s a mixed bag but for most people, the benefits of moderate caffeine use outweigh the risks:
Caffeine: Cognitive Enhancer Or Brain-Wrecker?
Now, caffeine’s less desirable effects can be mitigated somewhat by pairing it with l-theanine, as we’ve also discussed before:
L-Theanine: What’s The Tea? ← l-theanine also has many wonderful properties of its own, aside from its complementary effects when taken alongside caffeine
So, what’s the deal with caffeine and beetroot juice?
A performance-enhancing balancing act
Caffeine raises blood pressure, while beetroot lowers it, but there’s a lot more to it than that.
Researchers looked into the effects of caffeine and beetroot juice, together or separately, on athletic performance (in a 1000m run) in non-athletes.
They found:
- Caffeine alone enhanced second-run performance but not the first.
- Beetroot juice alone improved first-run performance but led to a performance decline after recovery.
- The caffeine + BJ combo resulted in the best initial and repeated 1000m run performances.
Specifically, they also noted:
- Caffeine alone caused higher blood lactate levels post-exercise.
- Beetroot juice increased muscle oxygenation by 25% during runs.
- The caffeine + BJ combo led to the highest post-exercise heart rate improvements.
You can read the paper in full here:
Caffeine and Beetroot Juice Optimize 1,000-m Performance: Shapley Additive Explanations Analysis
Now, maybe you don’t have a 1000m run to do, let alone multiple ones back-to-back, but most of us could sometimes do with an energy boost during the day, and this seems like an excellent way to get it.
That said, caffeine timing can be important too; midday is generally the best time for it, because:
- of course it should not be too late in the day, because the elimination half-life of caffeine (4–8 hours to eliminate just half of the caffeine, depending on genes, call it 6 hours as an average though honestly for most people it will either be 4 or 8, not 6) is such that it can easily interfere with sleep for most people
- because caffeine is an adenosine blocker, not an adenosine inhibitor, taking caffeine in the morning means either there’s no adenosine to block, or it’ll just “save” that adenosine for later, i.e. when the caffeine is eliminated, then the adenosine will kick in, meaning that your morning sleepiness has now been deferred to the afternoon, rather than eliminated.
Another reminder that caffeine is the “payday loan” of energy. So, midday it is. No morning sleepiness to defer, and yet also not so late as to interfere with sleep.
See also: Calculate (And Enjoy) The Perfect Night’s Sleep
Want to learn more?
Check out:
The Best Form Of Sugar For Energy During Exercise
Enjoy!
Share This Post

-
Can apps and digital resources support your child with autism or ADHD?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Neurodevelopmental conditions such as attention deficit hyperactivity disorder (ADHD) and autism affect about one in ten children. These conditions impact development, behaviour and wellbeing.
But children with these conditions and their caregivers often can’t get the support they need. Families report difficulties accessing health-care providers and experience long wait lists to receive care.
Digital tools, such as apps and websites, are often viewed as a solution to these gaps. With a single click or a download, families might be able to access information to support their child.
There are lots of digital tools available, but it’s hard to know what is and isn’t useful. Our new study evaluated freely available digital resources for child neurodevelopment and mental health to understand their quality and evidence base.
We found many resources were functional and engaging. However, resources often lacked evidence for the information provided and the claimed positive impact on children and families.
This is a common problem in the digital resource field, where the high expectations and claims of impact from digital tools to change health care have not yet been realised.

Fabio Principe/Shutterstock What type of resources?
Our study identified 3,435 separate resources, of which 112 (43 apps and 69 websites) met our criteria for review. These resources all claimed to provide information or supports for child neurodevelopment, mental health or wellbeing.
Resources had to be freely available, in English and have actionable information for children and families.
The most common focus was on autism, representing 17% of all resources. Resources suggested they provided strategies to promote speech, language and social development, and to support challenging behaviours.
Other common areas included language and communication (14%), and ADHD (10%).
Resources had various purposes, including journalling and providing advice, scheduling support, and delivering activities and strategies for parents. Resources delivered information interactively, with some apps organising content into structured modules.
Resources also provided options for alternative and assistive communication for people with language or communication challenges.
Most apps were functional and accessible
Our first question was about how engaging and accessible the information was. Resources that are hard to use aren’t used frequently, regardless of the information quality.
We evaluated aesthetics, including whether digital tools were easy to use and navigate, stylistically consistent, with clean and appealing graphics for users.
Most resources were rated as highly engaging, with strong accessibility and functionality.
Most apps and websites we evaluated were engaging. jamesteohart/Shutterstock But many lacked quality information
We ranked resources on various features from 1 (inadequate) to 5 (excellent), with a ranking of 3 considered acceptable. These ratings looked at how credible the resource was and whether there was evidence supporting it.
Despite their functionality, 37% of reviewed apps did not meet the minimum acceptable standards for information quality. This means many apps could not be recommended. Most websites fared better than apps.
There also wasn’t a lot of scientific evidence to suggest using either apps or digital resources actually helped families. Studies show long-term engagement with digital tools is rare, and downloads don’t correspond to frequent usage or benefits.
Digital tools are often viewed as a panacea to health-care gaps, but the evidence is yet to show they fill such gaps. Digital health is a fast-moving field and resources are often made available before they have been properly evaluated.
What should you look for in digital resources?
We found the highest quality resources were developed in collaboration with institutions, such as health, university or government groups.
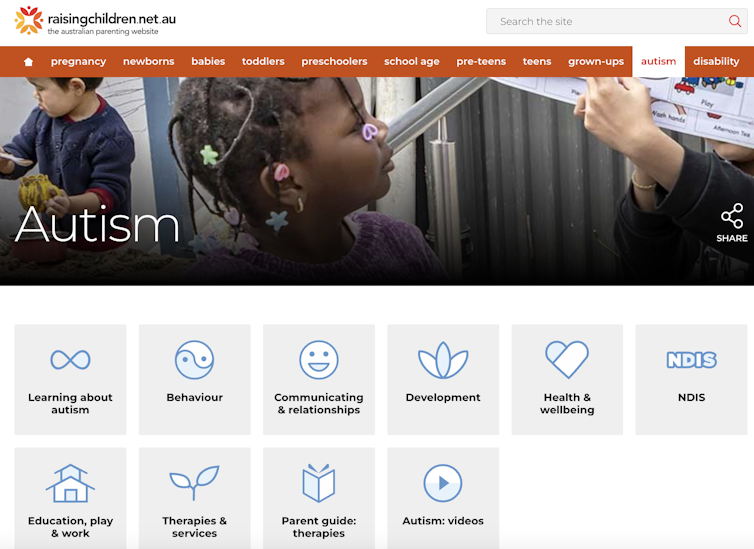
One highly rated resource was the Raising Children’s Network and the associated app, Raising Healthy Minds. These are co-developed with a university and hospital, and by people with appropriate qualifications.
This resource provides information to support children’s overall health, development and wellbeing, with dedicated sections addressing neurodevelopmental needs and concerns.
The Raising Children Network provides resources for child health, including neurodevelopmental needs. Raising Children Network screenshot Our research shows parents can assess whether digital resources are high quality by checking they are:
- factually correct. Look for where the app or resource is getting its information. Does the author have the qualifications and training to provide the information? Are they a registered health expert who is accountable to a regulatory body (such as AHPRA, the Australian Health Practitioners Regulation Agency) for providing information that does not cause harm?
- consistent across multiple credible sources, such as health institutions.
- linked to supporting information. Look for reliable links to reputable institutions. Links to peer-reviewed scientific journals are often helpful as those articles will also usually describe the limitations of the research presented.
- up-to-date. Apps should be frequently updated. For websites, dates of update are usually found on the homepage or at the bottom of individual pages.
Check when information was last updated. fizkes/Shutterstock Beware of red flags
Some things to watch out for are:
- testimonials and anecdotes without evidence and scientific links to back the anecdotes up. If it sounds too good to be true, it probably is.
- no information provided about conflicts of interest. Organisations gain when you click on their links or take their advice (financial, reputation and brand development). Think about what they gain when you use their information to help keep a balanced perspective.
Remember, the app’s star rating doesn’t mean it will contain factual information from a reliable source or be helpful for you and your child.
The role of digital tools
Digital tools won’t usually replace a health professional, but they can support care in many different ways. They may be used to help to educate and prepare for meetings, and to collaborate with health providers.
They may also be used to collect information about daily needs. Studies show reporting on sleep in children can be notoriously difficult, for example. But tracking sleep behaviour with actigraphy, where movement and activity patterns are measured using a wearable device, can provide information to support clinical care. With the promise of artificial intelligence, there will also be new opportunities to support daily living.
Our findings reflect a broader problem for digital health, however. Much investment is often made in developing products to drive use, with spurious claims of health benefits.
What’s needed is a system that prioritises the funding, implementation and evaluation of tools to demonstrate benefits for families. Only then may we realise the potential of digital tools to benefit those who use them.
Kelsie Boulton, Senior Research Fellow in Child Neurodevelopment, Brain and Mind Centre, University of Sydney and Adam Guastella, Professor and Clinical Psychologist, Michael Crouch Chair in Child and Youth Mental Health, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
The 3 Phases Of Fat Loss (& How To Do It Right!)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cori Lefkowith, of “Redefining Strength” and “Strength At Any Age” fame, has advice:
As easy as 1, 2, 3?
Any kind of fat loss plan will not work unless it takes into account that the body can and will adapt to a caloric deficit, meaning that constantly running a deficit will only ever yield short term results, followed by regaining weight (and feeling hungry the whole time). So, instead, if fat loss is your goal, you might want to consider doing it in these stages:
1. Lifestyle adjustments (main phase)
Focus on sustainable, gradual improvements in diet and workouts.
- Key strategies:
- Start with small, manageable changes, for example focusing on making your protein intake around 30–35% of your total calories.
- Track your current habits to identify realistic adjustments.
- Balance strength training and cardio, as maintaining your muscle is (and will remain) important.
- Signs of Progress:
- Slow changes in the numbers on the scale (up to 1 lb/week).
- Inches being lost (but probably not many), improved energy levels, and stable performance in workouts.
Caution: avoid feelings of extreme hunger or restriction. This is not supposed to be arduous.
2. Mini cut (short-term intensive)
Used for quick fat loss or breaking plateaus; lasts 7–14 days.
- Key strategies:
- Larger calorie deficit (e.g: 500 calories).
- High protein intake (40–50% of your total calories).
- Focus on strength training and reduce cardio, to avoid muscle loss.
- Signs of Progress:
- Rapid scale changes (up to 5 lbs/week).
- Reduced bloating, potential energy dips, and cravings.
- Temporary performance stagnation in workouts. Don’t worry about this; it’s expected and fine.
Caution: do not exceed 21 days, to avoid the metabolic adaptation that we talked about.
3. Diet break (rest & reset)
A maintenance period to recharge mentally and physically, typically lasting 7–21 days.
- Key strategies:
- Gradually increase calories (200–500) to maintenance level.
- Focus on performance goals and reintroducing foods you enjoy.
- Combine strength training with steady-state cardio.
- Signs of Progress:
- Increased energy, improved workout performance, and feeling fuller.
- Scale may fluctuate initially but stabilize or decrease by the end.
- Inches will be lost as muscle is built and fat is burned.
The purpose of this third stage is to prevent metabolic adaptation, regain motivation, and (importantly!) test maintenance.
For more on these and how best to implement them, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
- Key strategies:
-
The Most Underrated Hip Mobility Exercise (Not Stretching)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cori Lefkowith, of “Redefining Strength” and “Strong At Every Age” fame, is back to help us keep our hips in good order:
These tips don’t lie
It’s less about stretching, and more about range of motion and “use it or lose it”:
- Full range of motion in lifting exercises enhances joint mobility and stability, whereas strengthening muscles through a limited range of motion (e.g., half squats) can cause tightness.
- Lifting through a larger range of motion may result in faster strength gains too, so that’s a bonus.
- Customize your range of motion based on your body type and capability, but do try for what you reasonably can—don’t give up!
- Lower weights and focus on deeper movements like split squats or single-leg squats, but work up slowly if you have any difficulties to start with.
- Using exercises like the Bulgarian split squat and deficit split squat can improve hip mobility and strength (you’ll really need to see the video for this one)
- Fully controlling the range of motion is key to progress, even if it means going lighter; prioritize mobility over brute strength. Strength is good, but mobility is even more critical.
- Adding instability, such as raising the front foot in lunges, challenges muscles and increases mobility. Obviously, please be safe while doing so, and slowly increase the range of motion while maintaining control, avoiding reliance on momentum.
- Final tip that most don’t consider: try starting exercises from the bottom position to ensure proper form and muscle engagement!
For more on each of these plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: