Qigong: A Breath Of Fresh Air?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Qigong: Breathing Is Good (Magic Remains Unverified)
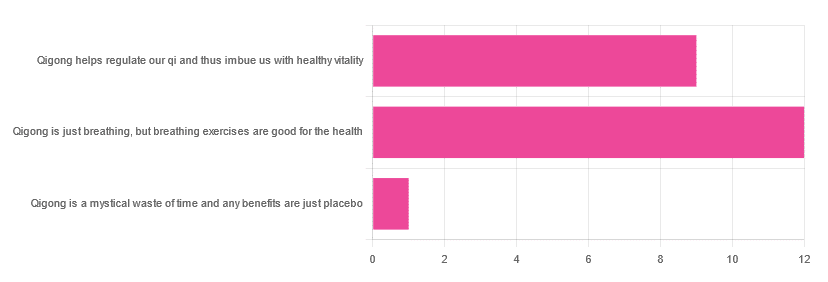
In Tuesday’s newsletter, we asked you for your opinions of qigong, and got the above-depicted, below-described, set of responses:
- About 55% said “Qigong is just breathing, but breathing exercises are good for the health”
- About 41% said “Qigong helps regulate our qi and thus imbue us with healthy vitality”
- One (1) person said “Qigong is a mystical waste of time and any benefits are just placebo”
The sample size was a little low for this one, but the results were quite clearly favorable, one way or another.
So what does the science say?
Qigong is just breathing: True or False?
True or False, depending on how we want to define it—because qigong ranges in its presentation from indeed “just breathing exercises”, to “breathing exercises with visualization” to “special breathing exercises with visualization that have to be exactly this way, with these hand and sometimes body movements also, which also must be just right”, to far more complex definitions that involve qi by various mystical definitions, and/or an appeal to a scientific analog of qi; often some kind of bioelectrical field or such.
There is, it must be said, no good quality evidence for the existence of qi.
Writer’s note, lest 41% of you want my head now: I’ve been practicing qigong and related arts for about 30 years and find such to be of great merit. This personal experience and understanding does not, however, change the state of affairs when it comes to the availability (or rather, the lack) of high quality clinical evidence to point to.
Which is not to say there is no clinical evidence, for example:
Acute Physiological and Psychological Effects of Qigong Exercise in Older Practitioners
…found that qigong indeed increased meridian electrical conductance!
Except… Electrical conductance is measured with galvanic skin responses, which increase with sweat. But don’t worry, to control for that, they asked participants to dry themselves with a towel. Unfortunately, this overlooks the fact that a) more sweat can come where that came from, because the body will continue until it is satisfied of adequate homeostasis, and b) drying oneself with a towel will remove the moisture better than it’ll remove the salts from the skin—bearing in mind that it’s mostly the salts, rather than the moisture itself, that improve the conductivity (pure distilled water does conduct electricity, but not very well).
In other words, this was shoddy methodology. How did it pass peer review? Well, here’s an insight into that journal’s peer review process…
❝The peer-review system of EBCAM is farcical: potential authors who send their submissions to EBCAM are invited to suggest their preferred reviewers who subsequently are almost invariably appointed to do the job. It goes without saying that such a system is prone to all sorts of serious failures; in fact, this is not peer-review at all, in my opinion, it is an unethical sham.❞
~ Dr. Edzard Ernst, a founding editor of EBCAM (he since left, and decries what has happened to it since)
One of the other key problems is: how does one test qigong against placebo?
Scientists have looked into this question, and their answers have thus far been unsatisfying, and generally to the tune of the true-but-unhelpful statement that “future research needs to be better”:
Problems of scientific methodology related to placebo control in Qigong studies: A systematic review
Most studies into qigong are interventional studies, that is to say, they measure people’s metrics (for example, blood pressure, heart rate, maybe immune function biomarkers, sleep quality metrics of various kinds, subjective reports of stress levels, physical biomarkers of stress levels, things like that), then do a course of qigong (perhaps 6 weeks, for example), then measure them again, and see if the course of qigong improved things.
This almost always results in an improvement when looking at the before-and-after, but it says nothing for whether the benefits were purely placebo.
We did find one study that claimed to be placebo-controlled:
…but upon reading the paper itself carefully, it turned out that while the experimental group did qigong, the control group did a reading exercise. Which is… Saying how well qigong performs vs reading (qigong did outperform reading, for the record), but nothing for how well it performs vs placebo, because reading isn’t a remotely credible placebo.
See also: Placebo Effect: Making Things Work Since… Well, A Very Long Time Ago ← this one explains a lot about how placebo effect does work
Qigong is a mystical waste of time: True or False?
False! This one we can answer easily. Interventional studies invariably find it does help, and the fact remains that even if placebo is its primary mechanism of action, it is of benefit and therefore not a waste of time.
Which is not to say that placebo is its only, or even necessarily primary, mechanism of action.
Even from a purely empirical evidence-based medicine point of view, qigong is at the very least breathing exercises plus (usually) some low-impact body movement. Those are already two things that can be looked at, mechanistic processes pointed to, and declarations confidently made of “this is an activity that’s beneficial for health”.
See for example:
- Effects of Qigong practice in office workers with chronic non-specific low back pain: A randomized control trial
- Qigong for the Prevention, Treatment, and Rehabilitation of COVID-19 Infection in Older Adults
- Impact of Medical Qigong on quality of life, fatigue, mood and inflammation in cancer patients: a randomized controlled trial
…and those are all from respectable journals with meaningful peer review processes.
None of them are placebo-controlled, because there is no real option of “and group B will only be tricked into believing they are doing deep breathing exercises with low-impact movements”; that’s impossible.
But! They each show how doing qigong reliably outperforms not doing qigong for various measurable metrics of health.
And, we chose examples with physical symptoms and where possible empirically measurable outcomes (such as COVID-19 infection levels, or inflammatory responses); there are reams of studies showings qigong improves purely subjective wellbeing—but the latter could probably be claimed for any enjoyable activity, whereas changes in inflammatory biomarkers, not such much.
In short: for most people, it indeed reliably helps with many things. And importantly, it has no particular risks associated with it, and it’s almost universally framed as a complementary therapy rather than an alternative therapy.
This is critical, because it means that whereas someone may hold off on taking evidence-based medicines while trying out (for example) homeopathy, few people are likely to hold off on other treatments while trying out qigong—since it’s being viewed as a helper rather than a Hail-Mary.
Want to read more about qigong?
Here’s the NIH’s National Center for Complementary and Integrative Health has to say. It cites a lot of poor quality science, but it does mention when the science it’s citing is of poor quality, and over all gives quite a rounded view:
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Why Brittle Bones Aren’t Just a Woman’s Problem

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Ronald Klein was biking around his neighborhood in North Wales, Pennsylvania, in 2006 and tried to jump a curb. “But I was going too slow — I didn’t have enough momentum,” he recalled.
As the bike toppled, he thrust out his left arm to break the fall. It didn’t seem like a serious accident, yet “I couldn’t get up,” he said.
At the emergency room, X-rays showed that he had fractured both his hip, which required surgical repair, and his shoulder. Klein, a dentist, went back to work in three weeks, using a cane. After about six months and plenty of physical therapy, he felt fine.
But he wondered about the damage the fall had caused. “A 52-year-old is not supposed to break a hip and a shoulder,” he said. At a follow-up visit with his orthopedist, “I said, ‘Maybe I should have a bone density scan.’”
As Klein suspected, the test showed he had developed osteoporosis, a progressive condition, increasing sharply with age, that thins and weakens bones and can lead to serious fractures. Klein immediately began a drug regimen and, now 70, remains on one.
Osteoporosis occurs so much more commonly in women, for whom medical guidelines recommend universal screening after age 65, that a man who was not a health care professional might not have thought about getting a scan. The orthopedist didn’t raise the prospect.
But about 1 in 5 men over age 50 will suffer an osteoporotic fracture in their remaining years, and among older adults, about a quarter of hip fractures occur in men.
When they do, “men have worse outcomes,” said Cathleen Colón-Emeric, a geriatrician at the Durham VA Health Care System and Duke University and the lead author of a recent study of osteoporosis treatment in male veterans.
“Men don’t do as well in recovery as women,” she said, with higher rates of death (25% to 30% within a year), disability and institutionalization. “A 50-year-old man is more likely to die from the complications of a major osteoporotic fracture than from prostate cancer,” she said.
(What’s “major”? Fractures of the wrist, hip, femur, humerus, pelvis or vertebra.)
In her study of 3,000 veterans ages 65 to 85, conducted at Veterans Affairs health centers in North Carolina and Virginia, only 2% of those assigned to the control group had undergone bone-density screening.
“Shockingly low,” said Douglas Bauer, a clinical epidemiologist and osteoporosis researcher at the University of California-San Francisco, who published an accompanying commentary in JAMA Internal Medicine. “Abysmal. And that’s at the VA, where it’s paid for by the government.”
But establishing a bone health service — overseen by a nurse who entered orders, sent frequent appointment reminders and explained results — led to dramatic changes in the intervention group, who had at least one risk factor for the condition.
Forty-nine percent of them said yes to a scan. Half of those tested had osteoporosis or a forerunner condition, osteopenia. Where appropriate, most of them began medications to preserve or rebuild their bones.
“We were pleasantly surprised that so many agreed to be screened and were willing to initiate treatment,” Colón-Emeric said.
After 18 months, bone density had increased modestly for those in the intervention group, who were more likely to stick to their drug regimens than osteoporosis patients of either sex in real-world conditions.
The study didn’t continue long enough to determine whether bone density increased further or fractures declined, but the researchers plan a secondary analysis to track that.
The results revive a longtime question: Given how life-altering, even deadly, such fractures can be, and the availability of effective drugs to slow or reverse bone loss, should older men be screened for osteoporosis, as women are? If so, which men and when?
Such issues mattered less when life spans were shorter, Bauer explained. Men have bigger and thicker bones and tend to develop osteoporosis five to 10 years later than women do. “Until recently, those men died of heart disease and smoking” before osteoporosis could harm them, he said.
“Now, men routinely live into their 70s and 80s, so they have fractures,” he added. By then, they have also accumulated other chronic conditions that impair their ability to recover.
With osteoporosis testing and treatment, “a man could see a clear-cut improvement in mortality and, more importantly, his quality of life,” Bauer said.
Both patients and many doctors still tend to regard osteoporosis as a women’s disease, however. “There’s a bit of a Superman idea,” said Eric Orwoll, an endocrinologist and osteoporosis researcher at Oregon Health & Science University.
“Men would like to believe they’re indestructible, so a fracture doesn’t have the implication that it should,” he added.
One patient, for example, for years resisted entreaties from his wife, a nurse, to “see someone” about his visibly rounded upper back.
Bob Grossman, 74, a retired public school teacher in Portland, blamed poor posture instead and told himself to straighten up. “I thought, ‘It can’t be osteoporosis — I’m a guy,’” he said. But it was.
Another obstacle to screening: “Clinical practice guidelines are all over the place,” Colón-Emeric said.
Professional associations like the Endocrine Society and the American Society for Bone and Mineral Research recommend that men 50 and older who have a risk factor, and all men over 70, should seek screening.
But the American College of Physicians and the U.S. Preventive Services Task Force have deemed the evidence for screening of men “insufficient.” Clinical trials have found that osteoporosis drugs increase bone density in men, as in women, but most male studies have been too small or lacked enough follow-up to show whether fractures also declined.
The task force’s position means that Medicare and many private insurers generally won’t cover screening for men who haven’t had a fracture, though they will cover care for men diagnosed with osteoporosis.
“Things have been stalled for decades,” Orwoll said.
So it may fall to older men themselves to ask their doctors about a DXA (pronounced DECKS-ah) scan, widely available at $100 to $300 out-of-pocket. Otherwise, because osteoporosis is typically asymptomatic, men (and women, who are also undertested and undertreated) don’t know their bones have deteriorated until one breaks.
“If you had a fracture after age 50, you should have a bone scan — that’s one of the key indicators,” Orwoll advised.
Other risk factors: falls, a family history of hip fractures, and a fairly long list of other health conditions including rheumatoid arthritis, hyperthyroidism and Parkinson’s disease. Smoking and excessive alcohol use increase the odds of osteoporosis as well.
“A number of medications also do a number on your bone density,” Colón-Emeric added, notably steroids and prostate cancer drugs.
When a scan reveals osteoporosis, depending on its severity, doctors may prescribe oral medications like Fosamax or Actonel, intravenous formulations like Reclast, daily self-injections of Forteo or Tymlos, or twice-annual injections of Prolia.
Lifestyle changes like exercising, taking calcium and vitamin D supplements, stopping smoking, and drinking only moderately will help but aren’t sufficient to stop or reverse bone loss, Colón-Emeric said.
Although guidelines don’t universally recommend it, at least not yet, she would like to see all men age 70 and up be screened, because the odds of disability after hip fractures are so high — two-thirds of older people will not regain their prior mobility, she noted — and the medications that treat it are effective and often inexpensive.
But informing patients and health care professionals that osteoporosis threatens men, too, has progressed “at a snail’s pace,” Orwoll said.
Klein remembers attending a seminar to instruct patients like him in using the drug Forteo. “I was the only male there,” he said.
The New Old Age is produced through a partnership with The New York Times.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
This article first appeared on KFF Health News and is republished here under a Creative Commons Attribution-NoDerivatives 4.0 International License.
Share This Post
-
Why Belly Fat Is The Last To Go (& 3 Signs You’re Nearly There)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cori Lefkowitz, of “Strong At Every Age” advises:
See the signs
It’s usually the last place to shrink, even though it’s the first place we want; it doesn’t help that most people quit too early or obsess over the scale, which can sabotage progress.
Three mistakes to avoid:
- Unduly focusing on calories: not only are listed caloric values often misleading, calorie-counting typically leads to restriction, fatigue, and rebound weight gain, none of which are good. Instead, track macros to keep your metabolism ticking over nicely, build/maintain muscle, and make what you’re doing sustainable.
- Prioritizing hard work over intentional work: random hard workouts and extreme restrictions will ultimately burn you out. Instead, every action should serve a clear purpose towards your goals, so do make a point of planning ahead from time to time (e.g. each month, make a plan, follow it, and then review your progress to plan again for the next month).
- Not following a workout progression: stringing random moves together won’t normally build lean muscle. Instead, she advises to repeat a structured plan for 3–6 weeks, progressively challenge yourself, measure results, and repeat until you’ve got to where you want to be.
Three signs you’re nearly there:
- Seeing more definition in other body parts: fat often comes off first from areas we don’t care about; this can even make the belly look bigger temporarily, but it’s actually progress!
- Clothes fitting more loosely: even without scale changes, fat loss and recomposition show up in how clothing fits over time.
- Improvements in performance, sleep, and health: stronger workouts, better energy, and healthier markers mean your body is functioning better and supporting fat loss.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Can You Shrink A Waist In Seven Days?
Take care!
Share This Post
-
Soy Allergy? No Problem! Turn Any Legume Into Tofu (Here’s How)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Legumes have similar chemical composition, which means they can generally be used in the same ways as each other:
Variety is the spice of life
In the video, he demonstrates this with green peas, red lentils, and green lentils, and mentions that it is the same for chickpeas too. The process is:
- Soak 100g dried legumes overnight in plenty of water.
- Drain and blend with 250ml fresh water until smooth.
- Pour into a nonstick frying pan, add ½ tsp salt, and stir.
- Cook until it thickens into a paste, then cook for another 2–3 minutes on low heat.
- Transfer to a 500ml mold, smooth the top, and set in the fridge for 1 hour.
- If properly set, it can be eaten as-is or fried into crispy cubes.
- Stir-fry tofu with: ginger, spring onions, garlic, and chili.
- Sauce: suggestions include soy sauce, rice wine vinegar, mirin, sesame oil.
- Garnish with: sesame and coriander seeds
Science behind it: heating alters protein bonds and starches, forming a thick paste that sets.
Note: legumes contain natural toxins that are destroyed by cooking. For some, like those mentioned above, frying for a few minutes is sufficient. However, kidney beans are high in phytohemagglutinin, which requires at least 20 minutes of cooking to be safe, making them unsuitable for this process.
For more on all of this, plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Six Ways To Eat For Healthier Skin
Take care!
Share This Post


Related Posts
-

What to Know About Stillbirths
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Series: Stillbirths:When Babies Die Before Taking Their First Breath
The U.S. has not prioritized stillbirth prevention, and American parents are losing babies even as other countries make larger strides to reduce deaths late in pregnancy.
Every year, more than 20,000 pregnancies in the U.S. end in a stillbirth, the death of an expected child at 20 weeks or more of pregnancy. Research shows as many as 1 in 4 stillbirths may be preventable. We interviewed dozens of parents of stillborn children who said their health care providers did not tell them about risk factors or explain what to watch for while pregnant. They said they felt blindsided by what followed. They did not have the information needed to make critical decisions about what happened with their baby’s body, about what additional testing could have been done to help determine what caused the stillbirth, or about how to navigate the process of requesting important stillbirth documents.
This guide is meant to help fill the void of information on stillbirths. It’s based on more than 150 conversations with parents, health care providers, researchers and other medical experts.
Whether you’re trying to better prepare for a pregnancy or grieving a loss, we hope this will help you and your family. This guide does not provide medical advice. We encourage you to seek out other reliable resources and consult with providers you trust.
We welcome your thoughts and questions at mailto:[email protected]. You can share your experience with stillbirth with us. If you are a health care provider interested in distributing this guide, let us know if we can help.
Table of contents:
- What Is Stillbirth?
- Are Stillbirths Preventable?
- What to Expect After a Stillbirth.
- Grieving After a Stillbirth.
- What You Might Say and Do After a Loved One Experiences a Stillbirth.
What Is Stillbirth?
Many people told us that the first time they heard the term stillbirth was after they delivered their stillborn baby. In many cases, the lack of information and awareness beforehand contributed to their heartache and guilt afterward.
Stillbirth is defined in the U.S. as the death of a baby in the womb at 20 weeks or more of pregnancy. Depending on when it happens, stillbirth is considered:
- Early: 20-27 weeks of pregnancy.
- Late: 28-36 weeks of pregnancy.
- Term: 37 or more weeks of pregnancy.
About half of all stillbirths in the U.S. occur at 28 weeks or later.
What is the difference between a stillbirth and a miscarriage?
Both terms describe pregnancy loss. The distinction is when the loss occurs. A miscarriage is typically defined as a loss before the 20th week of pregnancy, while stillbirth is after that point.
How common is stillbirth?
Each year, about 1 in 175 deliveries in the U.S. are stillbirths — that’s about 60 stillborn babies every day — making it one of the most common adverse pregnancy outcomes, but it is rarely discussed.
If you are surprised by that fact, you are not alone. Many people we spoke to did not know how common stillbirths are. Leandria Lee of Texas said she spent her 2021 pregnancy unaware that her daughter, Zuri Armoni, could die in the last phase of her pregnancy.
“If I was prepared to know that something could happen, I don’t think it would have been as bad. But to not know and then it happens, it affects you,” she said of her stillbirth at 35 weeks.
Some doctors have told us they don’t introduce the possibility of a stillbirth because they don’t want to create additional anxiety for patients.
Other doctors say withholding information leaves patients unprepared.
“We have this idea that we can’t scare the patient, which to me is very paternalistic,” said Dr. Heather Florescue, an OB-GYN near Rochester, New York, who works to inform doctors and patients about stillbirth prevention.
What causes stillbirths?
There is a lot we don’t know about stillbirths because there hasn’t been enough research. The cause of the stillbirth is unknown in about 1 in 3 cases.
What we do know is that a number of factors may cause or increase the risk of a stillbirth, including:
- The baby not growing as expected.
- Placental abnormalities or problems with the umbilical cord.
- Genetic or structural disorders that cause developmental issues.
- High blood pressure before pregnancy or preeclampsia, a potentially fatal complication that usually appears late in pregnancy and causes high blood pressure.
- Diabetes before or during pregnancy.
- An infection in the fetus, the placenta or the pregnant person.
- Smoking.
- Being 35 or older.
- Obesity.
- Being pregnant with more than one baby.
But not all doctors, hospitals or health departments perform tests to identify the potential cause of a stillbirth or determine if it could have been prevented. Even when a cause is identified, fetal death records are rarely updated. This means data is sometimes inaccurate. Researchers strongly encourage doctors to perform a stillbirth evaluation, which includes an examination of the placenta and umbilical cord, a fetal autopsy and genetic testing.
If your hospital or doctor does not proactively offer one or more of these exams, you can ask them to conduct the tests. Research shows that placental exams may help establish a cause of death or exclude a suspected one in about 65% of stillbirths, while autopsies were similarly useful in more than 40% of cases.
Are Stillbirths Preventable?
Not all stillbirths are preventable, but some are. For pregnancies that last 37 weeks or more, one study found that nearly half of stillbirths are potentially preventable.
Dr. Joanne Stone, who last year was president of the Society of Maternal-Fetal Medicine, leads the country’s first Rainbow Clinic at Mount Sinai Hospital in New York. The clinic is modeled on similar facilities in the United Kingdom that care for people who want to conceive again after a stillbirth. She said many doctors used to think there was nothing they could do to prevent stillbirth.
“People just looked at it like, ‘Oh, it was an accident, couldn’t have been prevented,’” said Stone, who also is the system chair of the obstetrics, gynecology and reproductive science department at the Icahn School of Medicine. “But we know now there are things that we can do to try to prevent that from happening.”
She said doctors can:
- More closely monitor patients with certain risk factors, like high blood pressure, diabetes or obesity.
- Ask about prior infant loss or other obstetrical trauma.
- Carefully assess whether a baby’s growth is normal.
- Work to diagnose genetic anomalies.
- Teach patients how to track their baby’s movements and encourage them to speak up if they notice activity has slowed or stopped.
- Deliver at or before 39 weeks if there are concerns.
What are the risks of stillbirth over the course of a pregnancy?
The risk of a stillbirth increases significantly toward the end of pregnancy, especially after 39 weeks. The risk is higher for people who get pregnant at 35 or older. The risk begins to climb even earlier, around 36 weeks, for people pregnant with twins.
What you and your doctor can do to reduce the risk of stillbirth.
While federal agencies in the U.S. have yet to come up with a checklist that may help reduce the risk of stillbirth, the Stillbirth Centre of Research Excellence in Australia has adopted a Safer Baby Bundle that lists five recommendations:
- Stop smoking.
- Regularly monitor growth to reduce the risk of fetal growth restriction, when the fetus is not growing as expected.
- Understand the importance of acting quickly if fetal movement decreases.
- Sleep on your side after 28 weeks.
- Talk to your doctor about when to deliver. Depending on your situation, it may be before your due date.
The American College of Obstetricians and Gynecologists has compiled a list of tests and techniques doctors can use to try to reduce the risk of a stillbirth. They include:
- A risk assessment to identify prenatal needs.
- A nonstresstest, which checks the fetus’s heart rate and how it changes as the fetus moves.
- A biophysical profile, which is done with an ultrasound to measure body movement, muscle tone and breathing, along with amniotic fluid volume.
The group stressed that there is no test that can guarantee a stillbirth won’t happen and that individual circumstances should determine what tests are run.
Are some people at higher risk for stillbirth?
Black women are more than twice as likely to have a stillbirth as white women. There are a number of possible explanations for that disparity, including institutional bias and structural racism, and a patient’s pre-pregnancy health, socioeconomic status and access to health care. In addition, research shows that Black women are more likely than white women to experience multiple stressful life events while pregnant and have their concerns ignored by their health care provider. Similar racial disparities drive the country’s high rate of maternal mortality.
How to find a provider you trust.
Finding a doctor to care for you during your pregnancy can be a daunting process. Medical experts and parents suggest interviewing prospective providers before you decide on the right one.
Here is a short list of questions you might want to ask a potential OB-GYN:
- What is the best way to contact you if I have questions or concerns?
- How do you manage inquiries after hours and on weekends? Do you see walk-ins?
- How do you manage prenatal risk assessments?
- What should I know about the risks of a miscarriage or stillbirth?
- How do you decide when a patient should be induced?
If a provider doesn’t answer your questions to your satisfaction, don’t be reluctant to move on. Dr. Ashanda Saint Jean, chair of the obstetrics and gynecology department at HealthAlliance Hospitals of the Hudson Valley in New York, said she encourages her patients to find the provider that meets their needs.
“Seek out someone that is like-minded,” said Saint Jean “It doesn’t have to be that they’re the same ethnicity or the same race, but like-minded in terms of the goals of what that patient desires for their own health and prosperity.”
What to know in the last trimester.
The last trimester can be an uncomfortable and challenging time as the fetus grows and you get increasingly tired. During this critical time, your provider should talk to you about the following topics:
- Whether you need a nonstress test to determine if the fetus is getting enough oxygen.
- The best way to track fetal movements.
- What to do if your baby stops moving.
- Whether you are at risk for preeclampsia or gestational diabetes.
Rachel Foran’s child, Eoin Francis, was stillborn at 41 weeks and two days. Foran, who lives in New York, said she believes that if her doctor had tracked her placenta, and if she had understood the importance of fetal movement, she and her husband might have decided to deliver sooner.
She remembers that her son was “very active” until the day before he was stillborn.
“I would have gone in earlier if someone had told me, ‘You’re doing this because the baby could die,’” she said of tracking fetal movement. “That would have been really helpful to know.”
Researchers are looking at the best way to measure the health, blood flow and size of the placenta, but studies are still in their early stages.
“If someone had been doing that with my son’s,” Foran said, “my son would be alive.”
A placental exam and an autopsy showed that a small placenta contributed to Foran’s stillbirth.
How often should you feel movement?
Every baby and each pregnancy are different, so it is important to get to know what levels of activity are normal for you. You might feel movement around 20 weeks. You’re more likely to feel movement when you’re sitting or lying down. Paying attention to movement during the third trimester is particularly important because research shows that changes, including decreased movement or bursts of excessive activity, are associated with an increased risk of stillbirth. Most of the time, it’s nothing. But sometimes it can be a sign that your baby is in distress. If you’re worried, don’t rely on a home fetal doppler to reassure you. Reach out to your doctor.
Saint Jean offers a tip to track movement: “I still tell patients each day to lay on their left side after dinner and record how many times their baby moves, because then that will give you an idea of what’s normal for your baby,” she said.
Other groups recommend using the Count the Kicks app as a way of tracking fetal movements and establishing what is normal for that pregnancy. Although there is no scientific consensus that counting kicks can prevent stillbirths, the American College of Obstetricians and Gynecologists and other groups recommend that patients be aware of fetal movement patterns.
Dr. Karen Gibbins is a maternal-fetal medicine specialist at Oregon Health & Science University who in 2018 had stillborn son named Sebastian. She said the idea that babies don’t move as much at the end of pregnancy is a dangerous myth.
“You might hear that babies slow down at the end,” she said. “They don’t slow down. They just have a little less space. So their movements are a little different, but they should be as strong and as frequent.”
What to Expect After a Stillbirth
What might happen at the hospital?
Parents are often asked to make several important decisions while they are still reeling from the shock and devastation of their loss. It’s completely understandable if you need to take some time to consider them.
Some other things you can ask for (if medical personnel don’t offer them) are:
- Blood work, a placental exam, an autopsy and genetic testing.
- A social worker or counselor, bereavement resources and religious or chaplain support.
- The option to be isolated from the labor rooms.
- Someone to take photos of you and your baby, typically either a nurse or an outside group.
- A small cooling cot that allows parents to spend more time with their babies after a stillbirth. If one is not available, you can ask for ice packs to put in the swaddle or the bassinet.
- A mold of your baby’s hands and feet.
- Information about burial or cremation services.
- Guidance on what to do if your milk comes in.
Getting an autopsy after a stillbirth.
Whether to have an autopsy is a personal decision. It may not reveal a cause of death, but it might provide important information about your stillbirth and contribute to broader stillbirth research. Autopsies can be useful if you are considering another pregnancy in the future. Families also told us that an autopsy can help parents feel they did everything they could to try to understand why their baby died.
But several families told us their health care providers didn’t provide them with the right information to help with that decision. Some aren’t trained in the advantages of conducting an autopsy after a stillbirth, or in when and how to sensitively communicate with parents about it. Some, for example, don’t explain that patients can still have an open-casket funeral or other service after an autopsy because the incisions can easily be covered by clothing. Others may not encourage an autopsy because they think they already know what caused the stillbirth or don’t believe anything could have been done to prevent it. In addition, not all hospitals have the capacity to do an autopsy, but there may be private autopsy providers that can perform one at an additional cost.
You can read more about autopsies in our reporting.
Paying for an autopsy after a stillbirth.
If you decide you want an autopsy, you may wonder whether you need to pay out-of-pocket for it. Several families told us their providers gave them incomplete or incorrect information. Many larger or academic hospitals offer autopsies at no cost to patients. Some insurance companies also cover the cost of an autopsy after a stillbirth.
When hospitals don’t provide an autopsy, they may give you names of private providers. That was the case for Rachel Foran. The hospital gave her and her husband a list of numbers to call if they wanted to pay for an autopsy themselves. The process, she said, shocked her.
“I had just delivered and we had to figure out what to do with his body,” Foran said. “It felt totally insane that that was what we had to do and that we had to figure it out on our own.”
An independent autopsy, records show, cost them $5,000.
What is a certificate of stillbirth and how do I get one?
A fetal death certificate is the official legal document that records the death. This is the document used to gather data on and track the number of stillbirths in the country. Many states also issue a certificate of stillbirth or a certificate of birth resulting in stillbirth, which acknowledge the baby’s birth. Families told us they appreciated having that document, since typical birth certificates are not issued for stillbirths. You can usually request a certificate from the vital records office.
Grieving After a Stillbirth
What are the effects of stillbirths on parents and families?
Over and over, families told us the effects of losing a baby can reverberate for a lifetime.
Bereavement support groups may help provide a space to share experiences and resources. Hospitals and birth centers may suggest a local grief group.
We talked with Anna Calix, a maternal health expert who became active in perinatal loss prevention after her son Liam was stillborn on his due date in 2016. Calix leads grief support groups for people of color in English and Spanish.
She suggested rededicating the time you would have spent taking care of a new baby to the grief process.
“You can do that by addressing your own thoughts and feelings and really experiencing those feelings,” Calix said. “We like to push those feelings away or try to do something to distract and avoid, but no matter what we do, the feelings are there.”
It’s important, she said, to give yourself permission to grow your connection with your child and work through thoughts of guilt or blame.
What You Might Say and Do After a Loved One Experiences a Stillbirth
Finding the right words can be difficult. The following are a few suggestions from parents who went through a stillbirth.
Helpful:
- Acknowledge the loss and offer condolences.
- Ask if the baby was named and use the name.
- Allow space for the family to talk about their baby.
Unhelpful:
- Avoid talking about the baby.
- Minimize the loss or compare experiences.
- Start statements with “at least.”
Suggested phrases to avoid:
- “You’re young. You can have more kids.”
- “At least you have other children.”
- “These things just happen.”
- “Your baby is in a better place now.”
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
What’s the difference between freckles, sunspots and moles?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You’ve got a new brown spot on your face, but is it a freckle or a sunspot? Or perhaps you’ve found a spot on your back that looks like a mole but is flatter than your other ones – is it a mole or a dark freckle?
Here’s how to tell the difference between freckles, sunspots and moles – and when you need to get a spot checked to see if it’s skin cancer.

Cottonbro Studio/Pexels Freckles
Freckles, known as ephelides, are small, flat, light brown spots that appear on people with fair skin, or red or light-coloured hair.
These people are more likely to have the MC1R gene, which leads to freckles forming.
Freckles are caused by sun exposure and are more noticeable in summer. When sunlight hits the skin, cells called melanocytes produce melanin, the pigment that gives skin its colour.
In people prone to freckles, the melanin doesn’t spread evenly. Instead, it clumps together, creating freckles.
Melanin doesn’t spread evenly in people prone to freckles. Chermiti Mohamed/Unsplash Freckles generally appear in childhood and may fade with age, especially if sun exposure reduces. As we age we produce less melanin, or it can break down or disperse, resulting in lighter or fewer freckles.
Using sunscreen and wearing protective clothing can help prevent new freckles from developing, especially on the face and arms.
While freckles are completely harmless, they are a sign that someone is genetically at higher risk of developing skin cancer.
Sunspots
Sunspots are also called age spots or solar lentigos (or liver spots, but they have nothing to do with the liver). They are larger than freckles: sometimes the size of a small coin, and appear as flat brown spots.
Sunspots develop over time due to long-term sun exposure, which leads to excessive melanin production. They tend to appear on skin with greater sun exposure, such as the face, hands, shoulders and arms.
Sunspots develop after years of sun exposure. Zay Nyi Nyi/Shutterstock Unlike freckles, which tend to get lighter with less sun exposure, sunspots will not fade with time, and may further darken with continued sun exposure.
However, some people try to remove their sunspots for cosmetic reasons using either a laser, chemical peel or a prescription topical cream.
While sunspots are not dangerous, they do increase your risk of other skin cancers in that area.
It’s also important to monitor them, as slow-growing melanomas may initially look like sunspots. If you see the spot changes in size, shape or colour, see your doctor to rule out skin cancer.
Moles
Moles are often dark, raised or flat skin growths that can appear anywhere on your body.
Although moles can exist from birth, they typically grow during childhood, adolescence and early adulthood (including during pregnancy, when hormones are changing), until around the age of around 40. Moles can increase in size, and new ones can also appear.
Most adults have between ten and 40 moles on their body. A person with a high mole count has 50 or more, while someone with a very high mole count has 100 or more.
Some moles are raised while others are flat. Pixel-Shot/Shutterstock Moles form when melanocytes grow in clusters instead of spreading evenly throughout the skin.
Moles can either be raised or flat, depending upon their type, depth and age.
Raised moles, referred to as compound nevi, have both flat and raised portions and typically have pigment that is deeper in the skin.
Dermal nevi are skin-coloured or light brown moles that are also raised.
Most moles are harmless. Some may have hair growing from them and some may disappear, whereas other moles may darken or alter with age or hormonal changes.
However, some moles can develop into melanoma, a dangerous form of skin cancer.
When to see your doctor
While freckles and sunspots are completely harmless, moles do require more attention, especially if they change in size, shape, colour or texture.
If a mole shows any of the following warning signs, see your doctor, who will use the ABCDE rule to detect if a lesion is a skin cancer:
- asymmetry: if one half of the mole looks different from the other half
- border: if your mole is shaped irregularly, jagged or has poorly defined edges
- colour: varied shades or sudden changes in colour of the mole
- diameter: if it is larger than 6 millimeters (about the size of a pencil eraser)
- evolving: if your mole has any changes in its size, shape, colour, or sensation such as itching or bleeding for more than a few weeks.
Our research shows only 21.7% of people can correctly identify melanoma on their own, so professional checks are essential.
How to prevent skin damage
Since freckles, sunspots and some moles are influenced by exposure to the sun, you can protect your skin by:
- avoiding the sun when ultraviolet rays are strongest
- wearing sunscreen with SPF 50 every day, even when it’s cloudy. Apply it 20 minutes before going outside and reapply every two hours
- wearing protective clothing, including a wide-brimmed hat to cover your face, neck and ears, and long-sleeved shirts and pants to protect your arms and legs.
Correction: this article originally referred to sun sports as actinic keratoses rather than solar lentigos.
Mike Climstein, Associate Professor, Faculty of Health, Southern Cross University; Jeremy Hudson, Adjunct Associate Professor, Faculty of Health, Southern Cross University; Michael Stapelberg, Adjunct Associate Professor, Faculty of Health, Southern Cross University, and Nedeljka Rosic, Senior Lecturer, Faculty of Health, Southern Cross University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Do Hard Things – by Steve Magness
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s easy to say that we must push ourselves if we want to achieve worthwhile things—and it’s also easy to push ourselves into an early grave by overreaching. So, how to do the former, without doing the latter?
That’s what this book’s about. The author, speaking from a background in the science of sports psychology, applies his accumulated knowledge and understanding to the more general problems of life.
Most of us are, after all, not sportspeople or if we are, not serious ones. Those few who are, will get benefit from this book too! But it’s mostly aimed at the rest of us who are trying to work out whether/when we should scale up, scale back, change track, or double down:
- How much can we really achieve in our career?
- How about in retirement?
- Do we ever really get too old for athletic feats, or should we keep pressing on?
Magness brings philosophy and psychological science together, to help us sort our way through.
Nor is this just a pep talk—there’s readily applicable, practical, real-world advice here, things to enable us to do our (real!) best without getting overwhelmed.
The style is pop-science, very easy-reading, and clear and comprehensible throughout—without succumbing to undue padding either.
Bottom line: this is a very pleasant read, that promises to make life more meaningful and manageable at the same time. Highly recommendable!
Click here to check out Do Hard Things, and get the most out of life!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: