When A Period Is Very Late (Post-Menopause)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Knowledge Is Power Safety, Post-Menopause Too
Note: this article will be most relevant for a subset of our subscribership, but it’s a very large subset, so we’re going to go ahead and address the reader as “you”.
If, for example, you are a man and this doesn’t apply to you, we hope it will interest you anyway (we imagine there are women in your life).
PS: the appendicitis check near the end, works for anyone with an appendix
We’ve talked before about things that come with (and continue after) menopause:
- What You Should Have Been Told About The Menopause Beforehand
- What Menopause Does To The Heart
- Alzheimer’s Sex Differences May Not Be What They Appear
But what’s going on if certain menstrual symptoms reappear post-menopause (e.g. after more than a year with no menstruation)?
Bleeding
You should not, of course, be experiencing vaginal bleeding post-menopause. You may have seen “PSA” style posts floating around social media warning that this is a sign of cancer. And, it can be!
But it’s probably not.
Endometrial cancer (the kind that causes such bleeding) affects 2–3% of women, and of those reporting post-menopausal bleeding, the cause is endometrial cancer only 9% of those times.
So in other words, it’s not to be ignored, but for 9 people out of 10 it won’t be cancer:
Read more: Harvard Health | Postmenopausal bleeding: Don’t worry—but do call your doctor
Other more likely causes are uterine fibroids or polyps. These are unpleasant but benign, and can be corrected with surgery if necessary.
The most common cause, however is endometrial and/or vaginal atrophy resulting in tears and bleeding.
Tip: Menopausal HRT will often correct this.
Read more: The significance of “atrophic endometrium” in women with postmenopausal bleeding
(“atrophic endometrium” and “endometrial atrophy” are the same thing)
In summary: no need to panic, but do get it checked out at your earliest convenience. This is not one where we should go “oh that’s weird” and ignore.
Cramps
If you are on menopausal HRT, there is a good chance that these are just period cramps. They may feel different than they did before, because you didn’t ovulate and thus you’re not shedding a uterine lining now, but your body is going to do its best to follow the instructions given by the hormones anyway (hormones are just chemical messengers, after all).
If it is just this, then they will probably settle down to a monthly cycle and become quite predictable.
Tip: if it’s the above, then normal advice for period cramps will go here. We recommend ginger! It’s been found to be as effective as Novafen (a combination drug of acetaminophen (Tylenol), caffeine, and ibuprofen), in the task of relieving menstrual pain:
See: Effect of Ginger and Novafen on menstrual pain: A cross-over trial
It could also be endometriosis. Normally this affects those of childbearing age, but once again, exogenous hormones (as in menopausal HRT) can fool the body into doing it.
If you are not on menopausal HRT (or sometimes even if you are), uterine fibroids (as discussed previously) are once again a fair candidate, and endometriosis is also still possible, though less likely.
Special last note
Important self-check: if you are experiencing a sharp pain in that general area and are worrying if it is appendicitis (also a possibility), then pressing on the appropriately named McBurney’s point is a first-line test for appendicitis. If, after pressing, it hurts a lot more upon removal of pressure (rather than upon application of pressure), this is considered a likely sign of appendicitis. Get thee to a hospital, quickly.
And if it doesn’t? Still get it checked out at your earliest convenience, of course (better safe than sorry), but you might make an appointment instead of calling an ambulance.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

If You’re Not Flexible, These Are The Only 3 Stretches You Need, To Fix That

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
If you can’t put your leg behind your head while standing, try doing the splits against a wall first, and progress from there! ← text version of an item from a “if you can’t do this yet, try this first” picture set this writer saw on Instagram once upon a time
So, what if you’re more at the point of not quite being able to touch your toes yet?
From zero to…
Liv, of LivInLeggings fame, has these three starter-stretches that are actually starter-stretches:
Stretch 1: Reverse Tabletop with Foot Tuck Variation
- Sit on the floor, feet slightly wider than your hips, lean back onto your hands (fingertips pointing outward).
- Lift your hips towards a reverse tabletop, engage your glutes, and flatten the front of your hips.
- Add a foot tuck variation by stepping one foot back and pressing your weight forward.
Benefits:
- Stretches multiple muscles, including the soles of the feet.
- Improves foot arches, balance, and stability.
- Loosens fascia, enhancing flexibility in subsequent stretches.
Stretch 2: Squat to Forward Fold
- Start in a low squat (feet wider than your hips, toes mostly forward).
- Alternate between a low squat and a forward fold, keeping your hands on the floor or your toes.
Benefits:
- Stretches hamstrings, glutes, and lower back.
- Maintains good form and avoids overstraining.
Stretch 3: Side Lunge with Side Body Reach
- Begin in a tall kneeling position, step one foot out to the side (toes pointing outward).
- Lunge your hips towards your front ankle, keeping your tailbone tucked.
- Add a side body reach by resting your forearm on your thigh and reaching the other arm overhead.
- For a deeper stretch, cradle the back of your head with your hand, pressing lightly for a tricep stretch.
Benefits:
- Stretches inner thighs, lats, and triceps.
- Improves posture, shoulder mobility, and low squat ability.
For more on each of these plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Test For Whether You Will Be Able To Achieve The Splits
Take care!
Share This Post
-

Can We Drink To Good Health?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Can we drink to good health?
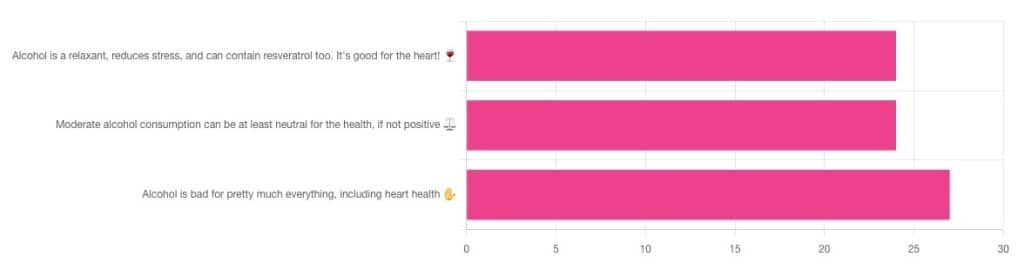
We asked you for your thoughts on alcohol and heart health, and we got quite an even spread of results!

If perchance that’s too tiny to read, the figures were:
- 32% voted for “Alcohol is a relaxant, reduces stress, and can contain resveratrol too. It’s good for the heart!”
- 32% voted for: “Moderate alcohol consumption can be at least neutral for the health, if not positive ⚖️”
- 36% voted for: “Alcohol is bad for pretty much everything, including heart health ✋”
One subscriber who voted for “Alcohol is a relaxant, reduces stress, and can contain resveratrol too. It’s good for the heart!” added the following thoughts:
❝While it isn’t necessary to consume alcohol, moderate amounts can be beneficial and contribute to well-being through social activity, celebrations, etc.❞
That’s an interesting point, and definitely many people do see alcohol that way! Of course, that does not mean that one will find no social activities, celebrations, etc, in parts of the world where alcohol consumption is uncommon. Indeed, in India, wedding parties where no alcohol is consumed can go on for days!
But, “we live in a society” and all that, and while we’re a health newsletter not a social issues newsletter, it’d be remiss of us to not acknowledge the importance of socialization for good mental health—and thus the rest of our health too.
So, if indeed all our friends and family drink alcohol, it can certainly make abstaining more of a challenge.
On that note, let’s take a moment to consider “The French Paradox” (an observation of a low prevalence of ischemic heart disease despite high intakes of saturated fat, a phenomenon accredited to the consumption of red wine).
As it happens, a comprehensive review in “Circulation”, a cardiovascular health journal, has suggested the French Paradox may not be so paradoxical after all.
Research suggests it has more to do with other lifestyle factors (and historic under-reporting of cardiovascular disease by French doctors), which would explain why Japan has lower rates of heart disease, despite drinking little wine, and more beer and spirits.
So, our subscriber’s note may not be completely without reason! It’s just about the party, not the alcohol.
One subscriber who voted for “Moderate alcohol consumption can be at least neutral for the health, if not positive ⚖️” wrote:
❝Keeping in mind, moderate means one glass of wine for women a day and two for men. Hard alcohol doesn’t have the same heart benefits as wine❞
That is indeed the guideline according to some health bodies!
In other places with different guiding advisory bodies, that’s been dropped down to one a day for everyone (the science may be universal, but how government institutions interpret that is not).
About that wine… Specifically, red wine, for its resveratrol content:
While there are polyphenols such as resveratrol in red wine that could boost heart health, there’s so little per glass that you may need 100–1000 glasses to get the dosage that provides benefits in mouse studies. If you’re not a mouse, you might even need more.
To this end, many people prefer resveratrol supplementation. ← link is to an example product, but there are plenty more so feel free to shop around
A subscriber who voted for “Alcohol is bad for pretty much everything, including heart health ✋” says:
❝New guidelines suggest 1 to 2 drinks a week are okay but the less the better.❞
If you haven’t heard these new guidelines, we’ll mention again: every government has its own official bodies and guidelines so perhaps your local guidelines differ, but for example here’s what that World Health Organization has to say (as of January this year):
WHO: No level of alcohol consumption is safe for our health
So, whom to believe? The governments who hopefully consider the welfare of their citizenry more important than the tax dollars from alcohol sales, or the World Health Organization?
It’s a tough one, but we’ll always err on the side of the science.
Share This Post
-

No Time to Panic – by Matt Gutman
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Matt Gutman is not a doctor or a psychologist. He’s a journalist, accustomed to asking questions and then asking more probing questions, unrelenting until he gets the answers he’s looking for.
This book is the result of what happened when he needed to overcome his own anxiety and panic attacks, and went on an incisive investigative journey.
The style is as clear and accessible as you’d expect of a journalist, and presents a very human exploration, nonetheless organized in a way that will be useful to the reader.
It’s said that “experience is a great teacher, but she sends hefty bills”. In this case as in many, it’s good to learn from someone else’s experience!
By the end of the book, you’ll have a good grounding in most approaches to dealing with anxiety and panic attacks, and an idea of efficacy/applicability, and what to expect.
Bottom line: without claiming any magic bullet, this book presents six key strategies that Gutman found to work, along with his experiences of what didn’t. Valuable reading if you want to curb your own anxiety, or want to be able to help/support someone else with theirs.
Click here to check out No Time To Panic, and find the peace you deserve!
Share This Post

Related Posts
-

Cost of living: if you can’t afford as much fresh produce, are canned veggies or frozen fruit just as good?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The cost of living crisis is affecting how we spend our money. For many people, this means tightening the budget on the weekly supermarket shop.
One victim may be fresh fruit and vegetables. Data from the Australian Bureau of Statistics (ABS) suggests Australians were consuming fewer fruit and vegetables in 2022–23 than the year before.
The cost of living is likely compounding a problem that exists already – on the whole, Australians don’t eat enough fruit and vegetables. Australian dietary guidelines recommend people aged nine and older should consume two serves of fruit and five serves of vegetables each day for optimal health. But in 2022 the ABS reported only 4% of Australians met the recommendations for both fruit and vegetable consumption.
Fruit and vegetables are crucial for a healthy, balanced diet, providing a range of vitamins and minerals as well as fibre.
If you can’t afford as much fresh produce at the moment, there are other ways to ensure you still get the benefits of these food groups. You might even be able to increase your intake of fruit and vegetables.

New Africa/Shutterstock Frozen
Fresh produce is often touted as being the most nutritious (think of the old adage “fresh is best”). But this is not necessarily true.
Nutrients can decline in transit from the paddock to your kitchen, and while the produce is stored in your fridge. Frozen vegetables may actually be higher in some nutrients such as vitamin C and E as they are snap frozen very close to the time of harvest. Variations in transport and storage can affect this slightly.
Minerals such as calcium, iron and magnesium stay at similar levels in frozen produce compared to fresh.
Another advantage to frozen vegetables and fruit is the potential to reduce food waste, as you can use only what you need at the time.
Freezing preserves the nutritional quality of vegetables and increases their shelf life. Tohid Hashemkhani/Pexels As well as buying frozen fruit and vegetables from the supermarket, you can freeze produce yourself at home if you have an oversupply from the garden, or when produce may be cheaper.
A quick blanching prior to freezing can improve the safety and quality of the produce. This is when food is briefly submerged in boiling water or steamed for a short time.
Frozen vegetables won’t be suitable for salads but can be eaten roasted or steamed and used for soups, stews, casseroles, curries, pies and quiches. Frozen fruits can be added to breakfast dishes (with cereal or youghurt) or used in cooking for fruit pies and cakes, for example.
Canned
Canned vegetables and fruit similarly often offer a cheaper alternative to fresh produce. They’re also very convenient to have on hand. The canning process is the preservation technique, so there’s no need to add any additional preservatives, including salt.
Due to the cooking process, levels of heat-sensitive nutrients such as vitamin C will decline a little compared to fresh produce. When you’re using canned vegetables in a hot dish, you can add them later in the cooking process to reduce the amount of nutrient loss.
To minimise waste, you can freeze the portion you don’t need.
Fermented
Fermented vegetables are another good option. Angela Khebou/Unsplash Fermentation has recently come into fashion, but it’s actually one of the oldest food processing and preservation techniques.
Fermentation largely retains the vitamins and minerals in fresh vegetables. But fermentation may also enhance the food’s nutritional profile by creating new nutrients and allowing existing ones to be absorbed more easily.
Further, fermented foods contain probiotics, which are beneficial for our gut microbiome.
5 other tips to get your fresh fix
Although alternatives to fresh such as canned or frozen fruit and vegetables are good substitutes, if you’re looking to get more fresh produce into your diet on a tight budget, here are some things you can do.
1. Buy in season
Based on supply and demand principles, buying local seasonal vegetables and fruit will always be cheaper than those that are imported out of season from other countries.
2. Don’t shun the ugly fruit and vegetables
Most supermarkets now sell “ugly” fruit and vegetables, that are not physically perfect in some way. This does not affect the levels of nutrients in them at all, or their taste.
Buying fruit and vegetables during the right season will be cheaper. August de Richelieu/Pexels 3. Reduce waste
On average, an Australian household throws out A$2,000–$2,500 worth of food every year. Fruit, vegetables and bagged salad are the three of the top five foods thrown out in our homes. So properly managing fresh produce could help you save money (and benefit the environment).
To minimise waste, plan your meals and shopping ahead of time. And if you don’t think you’re going to get to eat the fruit and vegetables you have before they go off, freeze them.
4. Swap and share
There are many websites and apps which offer the opportunity to swap or even pick up free fresh produce if people have more than they need. Some local councils are also encouraging swaps on their websites, so dig around and see what you can find in your local area.
5. Gardening
Regardless of how small your garden is you can always plant produce in pots. Herbs, rocket, cherry tomatoes, chillies and strawberries all grow well. In the long run, these will offset some of your cost on fresh produce.
Plus, when you have put the effort in to grow your own produce, you are less likely to waste it.
Evangeline Mantzioris, Program Director of Nutrition and Food Sciences, Accredited Practising Dietitian, University of South Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Too much vitamin B6 can be toxic. 3 symptoms to watch out for
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Side effects from taking too much vitamin B6 – including nerve damage – may be more widespread than we think, Australia’s medicines regulator says.
In an ABC report earlier this week, a spokesperson for the Therapeutic Goods Administration (TGA) says it may have underestimated the extent of the side effects from vitamin B6 supplements.
However, there are proposals to limit sales of high-dose versions due to safety concerns.
A pathologist who runs a clinic that tests vitamin B6 in blood samples from across Australia also appeared on the program. He told the ABC that data from May suggests 4.5% of samples tested had returned results “very likely” indicating nerve damage.
Selena3726/Shutterstock What is vitamin B6?
Vitamin B6, also known as pyridoxine, plays an important role in keeping the body healthy. It is involved in the metabolism of proteins, carbohydrates and fats in food. It is also important for the production of neurotransmitters – chemical messengers in the brain that maintain its function and regulate your mood.
Vitamin B6 also supports the immune system by helping to make antibodies, which fight off infections. And it is needed to produce haemoglobin, the protein in red blood cells that carries oxygen around the body.
Some women take a vitamin B6 supplement when pregnant. It is thought this helps reduce the nausea associated with the early stages of pregnancy. Some women also take it to help with premenstrual syndrome.
However, most people don’t need, and won’t benefit from, a vitamin B6 supplement. That’s because you get enough vitamin B6 from your diet through meat, breakfast cereal, fruit and vegetables.
You don’t need much. A dose of 1.3–1.7 milligrams a day is enough for most adults.
Currently, vitamin B6 supplements with a daily dose of 5–200mg can be sold over the counter at health food stores, supermarkets and pharmacies.
Because of safety concerns, the TGA is proposing limiting their sale to pharmacies, and only after consultation with a pharmacist.
Daily doses higher than 200mg already need a doctor’s prescription. So under the proposal that would stay the same.
What happens if you take too much?
If you take too much vitamin B6, in most cases the excess will be excreted in your urine and most people won’t experience side effects. But there is a growing concern about long-time, high-dose use.
A side effect the medical community is worried about is peripheral neuropathy – where there is damage to the nerves outside the brain and spinal cord. This results in pain, numbness or weakness, usually in your hands and feet. We don’t yet know exactly how this happens.
In most reported cases, these symptoms disappear once you stop taking the supplement. But for some people it may take three months to two years before they feel completely better.
There is growing, but sometimes contradictory, evidence that high doses (more than 50mg a day) for extended periods can result in serious side effects.
A study from the 1990s followed 70 patients for five years who took a dose of 100 to 150mg a day. There were no reported cases of neuropathy.
But more recent studies show high rates of side effects.
A 2023 case report provides details of a man who was taking multiple supplements. This resulted in a daily combined 95mg dose of vitamin B6, and he experienced neuropathy.
Another report describes seven cases of neuropathy linked to drinking energy drinks containing vitamin B6.
Reports to the TGA’s database of adverse events notifications (a record of reported side effects) shows 174 cases of neuropathy linked with vitamin B6 use since 2023.
What should I do if I take vitamin B6?
The current advice is that someone who takes a dose of 50mg a day or more, for more than six months, should be monitored by a health-care professional. So if you regularly take vitamin B6 supplements you should discuss continued use with your doctor or pharmacist.
There are three side effects to watch out for, the first two related to neuropathy:
- numbness or pain in the feet and hands
- difficulty with balance and coordination as a result of muscle weakness
- heartburn and nausea.
If you have worrying side effects after taking vitamin B6 supplements, contact your state’s poison information centre on 13 11 26 for advice.
Nial Wheate, Professor, School of Natural Sciences, Macquarie University and Slade Matthews, Senior Lecturer, Toxicology, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Body Image Dissatisfaction/Appreciation Across The Ages
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Every second news article about body image issues is talking about teens and social media use, but science tells a different story.
A large (n=1,327) study of people of mixed genders aged 16–88 examined matters relating to people’s body image, expecting…
❝We hypothesized that body dissatisfaction and importance of appearance would be higher in women than in men, that body dissatisfaction would remain stable across age in women, and that importance of appearance would be lower in older women compared to younger women. Body appreciation was predicted to be higher in men than in women.❞
As they discovered, only half of that turned out to be true:
❝In line with our hypotheses, body dissatisfaction was higher in women than in men and was unaffected by age in women, and importance of appearance was higher in women than in men.
However, only in men did age predict a lower level of the importance of appearance. Compared to men, women stated that they would invest more hours of their lives to achieve their ideal appearance.
Contrary to our assumption, body appreciation improved and was higher in women across all ages than in men.❞
You can read the study in full here:
That’s a lot of information, and we don’t have the space to go into all parts of it here, fascinating as that would be. So we’re going to put two pieces of information (from the above) next to each other:
- body dissatisfaction was higher in women than in men and was unaffected by age in women
- body appreciation improved and was higher in women across all ages than in men
…and resolve this apparent paradox.
Dissatisfied appreciation
How is it that women are both more dissatisfied with, and yet also more appreciative of, their bodies?
The answer is that we can have positive and negative feelings about the same thing, without them cancelling each other out. In short, simply, feeling more feelings about it.
Whether the gender-related disparity in this case comes more from hormones or society could be vigorously debated, but chances are, it’s both. And, for our gentleman-readers, note that the principle still applies to you, even if scaled down on average.
Call to action:
- be aware of the negative feelings of body dissatisfaction
- focus on the positive feelings of body appreciation
While in theory both could motivate us to action, in reality, the former will tend to inform us (about what we might wish to change), while the latter will actually motivate us in a useful way (to do something positive about it).
This is because the negative feelings about body image tend to be largely based in shame, and shame is a useless motivator (i.e., it simply doesn’t work) when it comes to taking positive actions:
Why Shame Only Works Negatively
You can’t hate yourself into a body you love
That may sound like a wishy-washy platitude, but given the evidence on how shame works (and doesn’t), it’s true.
Instead, once you’ve identified the things about your body with which you’re dissatisfied, you can then assess:
- what can reasonably be changed
- whether it is important enough to you to change it
- how to go about usefully changing it
While weight issues are perhaps the most commonly-discussed body image consideration, to the point that often all others get forgotten, let’s look at something that’s generally more specific to adults, and also a very common cause of distress for women and men alike: hair loss/thinning.
If your hair is just starting to thin and fall, then if this bothers you, there’s a lot that can be done about it quite easily, but (and this is important) you have to love yourself enough to actually do it. Merely feeling miserable about it, and perhaps like you don’t deserve better, or that it is somehow a personal failing on your part, will not help.
If your hair has been gone for years, then chances are you’ve made your peace with this by now, and might not even take it back if a fairy godmother came along and offered to restore it magically. On the other hand, let’s say that you’re just coming out the other end of a 10-year-long depression, and perhaps you let a lot of things go that you now wish you hadn’t, and maybe your hair is one of them. In this case, now you need to decide whether getting implants (likely the only solution at this late stage) is worth it.
Note that in both cases, whatever the starting point and whether the path ahead is easy or hard, the person who has dissatisfaction and/but still values themself and their body will get what they need.
In contrast, the person who has dissatisfaction and does not value themself and their body, will languish.
The person without dissatisfaction, of course, probably already has what they need.
In short: identification of dissatisfaction + love and appreciation of oneself and one’s body → motivation to usefully take action (out of love, not hate)
Now, dear reader, apply the same thinking to whatever body image issues you may have, and take it from there!
Embodiment
A quick note in closing: if you are a person with no body dissatisfactions, there are two main possible reasons:
- You are genuinely happy with your body in all respects. Congratulations!
- You have disassociated from your body to such an extent that it’s become a mere vehicle to you and you don’t care about it.
This latter may seem like a Zen-level win, but in fact it’s a warning sign for depression, so please do examine that even if you don’t “feel” depressed (depression is often characterized by a lack of feelings), perhaps by taking the (very quick) free PHQ9 Test ← under 2 minutes; immediate results; industry-standard diagnostic tool
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: