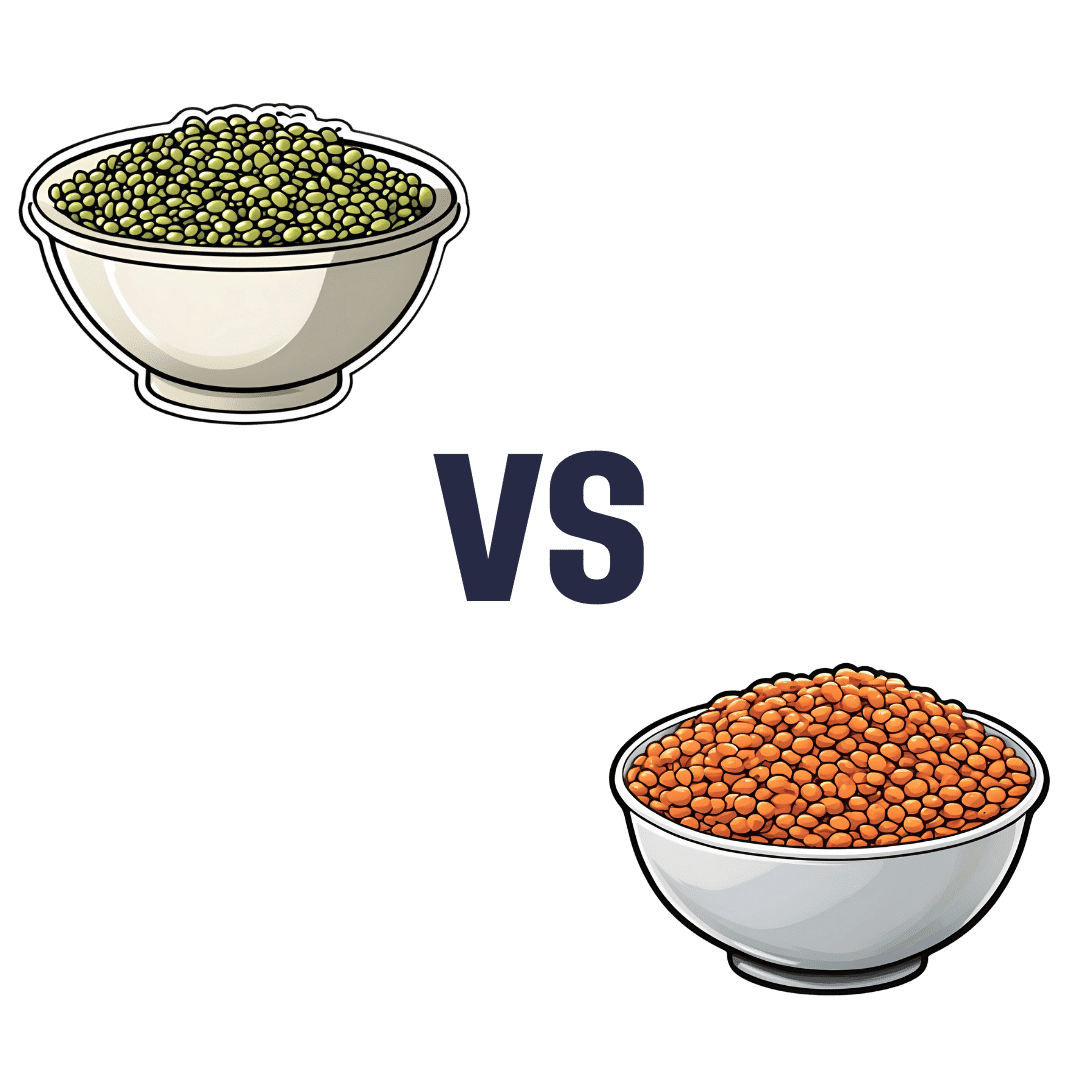
Mung Beans vs Red Lentils – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing mung beans to red lentils, we picked the lentils.
Why?
Both are great! But the lentils win on overall nutritional density.
In terms of macros, they have approximately the same carbs and fiber, and are both low glycemic index foods. The deciding factor is that the lentils have slightly more protein—but it’s not a huge difference; both are very good sources of protein.
In the category of vitamins, mung beans have more of vitamins A, E, and K, while red lentils have more of vitamins B1, B2, B3, B5, B6, B9, C, and choline. An easy win for lentils.
When it comes to minerals, again both are great, but mung beans have more calcium and magnesium (hence the green color) while red lentils have more copper, iron, manganese, phosphorus, potassium, selenium, and zinc. Another clear win for lentils.
Polyphenols are also a worthy category to note here; both have plenty, but red lentils have more, especially flavonols, anthocyanidins, proanthocyanidins, and anthocyanins (whence the red color).
In short: enjoy both, because diversity is almost always best. But if you’re picking one, red lentils are the most nutritious of the two.
Want to learn more?
You might like to read:
Sprout Your Seeds, Grains, Beans, Etc
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Seven Things To Do For Good Lung Health!

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
YouTube Channel Wellness Check is challenging us all to do the following things. They’re framing it as a 30-day challenge, but honestly, there’s nothing here that isn’t worth doing for life
Here’s the list:
- Stop smoking (of course, smoking is bad for everything, but the lungs are one of its main areas of destruction)
- Good posture (a scrunched up chest is not the lungs’ best operating conditions!)
- Regular exercise (exercising your body in different ways exercises your lungs in different ways!)
- Monitor air quality (some environments are much better/worse than others, but don’t underestimate household air quality threats either)
- Avoid respiratory infections (shockingly, COVID is not great for your lungs, nor are the various other respiratory infections available)
- Check your O2 saturation levels (pulse oximeters like this one are very cheap to buy and easy to use)
- Prevent mucus and phlegm from accumulating (these things are there for reasons; the top reason is trapping pathogens, allergens, and general pollutants/dust etc; once those things are trapped, we don’t want that mucus there any more!)
Check out the video itself for more detail on each of these items:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to know more?
You might like our article about COPD:
Why Chronic Obstructive Pulmonary Disease (COPD) Is More Likely Than You Think
Take care!
Share This Post
-

Exercises That Help You Walk Farther Without Pain
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Alyssa Kuhn shows us how:
At the seat of the problem
Glutes are critical to walking, because they not only help push your body push forwards, but also stabilize your pelvis to prevent limping or a waddling gait.
For this reason, weak glutes can (and often do) lead to joint pain, poor balance, quicker fatigue, due to increased stress on your hips, knees, and back—which in turn can lead to osteoarthritis, usually of the knee(s), in the first instance.
So, how to avoid that:
- Step-ups: step onto a step with one leg and step back down with the same leg to strengthen the glutes that drive you forwards. You can increase the height of a step or add weight to make the movement more challenging.
- Banded lateral steps: place a resistance band around your shins and step one leg out to the side while the other stabilizes your pelvis. Keep the tension on, and avoid letting your body sway side to side. You can also anchor a band to a stable object and move one leg against resistance, if maintaining balance is difficult at first. But if you do that, do try to progress to the main version when you can, because you need that balance too!
- Single-leg balance taps: a great one for training that balance, as well as training glute stability; simply stand on one leg and tap the other foot heel-toe on the floor. Keep your body upright, while your glutes stabilize your pelvis during movement.
For more on all of this plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
5 Proven Tips To Walk Longer Without Pain Or Discomfort
Take care!
Share This Post
-

Take These To Lower Cholesterol! (Statin Alternatives)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Ada Ozoh, a diabetes specialist, took an interest in this upon noting the many-headed beast that is metabolic syndrome means that neither diabetes nor cardiovascular disease exist in a vacuum, and there are some things that can help a lot against both. Here she shares some of her top recommendations:
Statin-free options
Dr. Ozoh recommends:
- Bergamot: lowers LDL (“bad” cholesterol) by about 30% and slightly increases HDL (“good” cholesterol), at 500–1000mg/day, seeing results in 1–6 months
- Berberine: prevents fat absorption and helps burn stored fat, as well as reducing blood sugar levels and blood pressure, at 1,500mg/day
- Silymarin: protects the liver, and lowers cholesterol in type 2 diabetes, at 280–420mg/day
- Phytosterols: lower cholesterol by about 10%; found naturally in many plants, but it takes supplementation to read the needed (for this purpose) dosage of 2g/day
- Red yeast rice: this is white rice fermented with yeast, and it lowers LDL cholesterol by about 25%, seeing results in around 3 months
For more information on all of the above (including more details on the biochemistry, as well as potential issues to be aware of), enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- Statins: His & Hers? Very Different For Men & Women
- Berberine For Metabolic Health
- Milk Thistle For The Brain, Bones, & More ← this is about silymarin, which is extracted from Silybum marianum, the milk thistle plant
Take care!
Share This Post

Related Posts
-
Can You Pass These 5 Mobility Tests?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
90% of people fail, so you’ll be in good company if you don’t, but you might also consider it a call to action to achieve these!
Mobility coach Alisa Szyman shows us how:
Move it or lose it
Here are the “5” tests, though two of them (hamstrings and hips) being in two parts each means you might prefer to count them as 7:
- Shoulder mobility (the up-scratch test): reach one hand over your shoulder and the other behind your back, and try to touch your hands while keeping your lower back neutral. It’s a pass if your hands touch but fail if there is a gap, which indicates limited shoulder mobility or possible left–right asymmetry.
- Hamstring flexibility (passive flexibility): stand with your legs straight and fold forwards to touch the floor with your hands or palms, passing if you reach the floor and failing if you cannot.
- Hamstring mobility (active flexibility): lie on your back with both legs straight and lift one leg using only your muscles until it reaches about 90°, passing if the leg reaches vertical and failing if it cannot while remaining straight.
- Spinal rotation: sit tall in a chair with your hands clasped at chest height and rotate your torso to each side while keeping your hips facing forwards, passing if you reach roughly 90° of rotation each way and failing if your rotation is clearly restricted.
- Ankle mobility (knee-to-wall test): stand with your foot about 12cm from a wall and bend your knee forwards to touch the wall while keeping your heel flat, passing if your knee reaches the wall without your heel lifting.
- Hip extension: lie near the edge of a bed or bench while pulling one knee to your chest and letting the other leg relax downwards, passing if the lowered leg stays relaxed and down and failing if it lifts, straightens, or causes your lower back to engage.
- Hip rotation: sit on the floor with both knees bent and feet flat, then drop both knees together side to side while keeping your chest upright, passing if both sides move smoothly without leaning back or hip pinching.
For more on all of this plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Mobility For Now & For Later: Train For The Marathon That Is Your Life!
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

‘Free birthing’ and planned home births might sound similar but the risks are very different
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The death of premature twins in Byron Bay in an apparent “wild birth”, or free birth, last week has prompted fresh concerns about giving birth without a midwife or medical assistance.
This follows another case from Victoria this year, where a baby was born in a critical condition following a reported free birth.
It’s unclear how common free birthing is, as data is not collected, but there is some evidence free births increased during the COVID pandemic.
Planned home births also became more popular during the pandemic, as women preferred to stay away from hospitals and wanted their support people with them.
But while free births and home births might sound similar, they are a very different practice, with free births much riskier. So what’s the difference, and why might people opt for a free birth?
What are home births?
Planned home births involve care from midwives, who are registered experts in childbirth, in a woman’s home.
These registered midwives work privately, or are part of around 20 publicly funded home birth programs nationally that are attached to hospitals.
They provide care during the pregnancy, labour and birth, and in the first six weeks following the birth.
The research shows that for women with low risk pregnancies, planned home births attended by competent midwives (with links to a responsive mainstream maternity system) are safe.
Home births result in less intervention than hospital births and women perceive their experience more positively.
What are free births?
A free birth is when a woman chooses to have a baby, usually at home, without a registered health professional such as a midwife or doctor in attendance.
Different terms such as unassisted birth or wild pregnancy or birth are also used to refer to free birth.
The parents may hire an unregulated birth worker or doula to be a support at the birth but they do not have the training or medical equipment needed to manage emergencies.
Women may have limited or no health care antenatally, meaning risk factors such as twins and breech presentations (the baby coming bottom first) are not detected beforehand and given the right kind of specialist care.
Why do some people choose to free birth?
We have been studying the reasons women and their partners choose to free birth for more than a decade. We found a previous traumatic birth and/or feeling coerced into choices that are not what the woman wants were the main drivers for avoiding mainstream maternity care.
Australia’s childbirth intervention rates – for induction or augmentation of labour, episiotomy (cutting the tissue between the vaginal opening and the anus) and caesarean section – are comparatively high.
One in ten women report disrespectful or abusive care in childbirth and some decide to make different choices for future births.
Lack of options for a natural birth and birth choices such as home birth or birth centre birth also played a major role in women’s decision to free birth.
Publicly funded home birth programs have very strict criteria around who can be accepted into the program, excluding many women.
In other countries such as the United Kingdom, Netherlands and New Zealand, publicly funded home births are easier to access.

It can be difficult to access home birth services in Australia.
Ink Drop/ShutterstockOnly around 200 midwives provide private midwifery services for home births nationally. Private midwives are yet to obtain insurance for home births, which means they are risking their livelihoods if something goes wrong and they are sued.
The cost of a home birth with a private midwife is not covered by Medicare and only some health funds rebate some of the cost. This means women can be out of pocket A$6-8,000.
Access to home birth is an even greater issue in rural and remote Australia.
How to make mainstream care more inclusive
Many women feel constrained by their birth choices in Australia. After years of research and listening to thousands of women, it’s clear more can be done to reduce the desire to free birth.
As my co-authors and I outline in our book, Birthing Outside the System: The Canary in the Coal Mine, this can be achieved by:
- making respectful care a reality so women aren’t traumatised and alienated by maternity care and want to engage with it
- supporting midwifery care. Women are seeking more physiological and social ways of birthing, minimising birth interventions, and midwives are the experts in this space
- supporting women’s access to their chosen place of birth and model of care and not limiting choice with high out-of-pocket expenses
- providing more flexible, acceptable options for women experiencing risk factors during pregnancy and/or birth, such as having a previous caesarean birth, having twins or having a baby in breech position. Women experiencing these complications experience pressure to have a caesarean section
- getting the framework right with policies, guidelines, education, research, regulation and professional leadership.
Ensuring women’s rights and choices are informed and respected means they’re less likely to feel they’re left with no other option.

Hannah Dahlen, Professor of Midwifery, Associate Dean Research and HDR, Midwifery Discipline Leader, Western Sydney University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
What Can Be Done About Long COVID?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small 😎
❝Can anything be done about long covid at all?❞
The short answer is: yes!
The longer answer is…
For the sake of us being methodical, kindly pardon that we will start by saying that ideally, the best thing to do about it is to avoid getting COVID in the first place. We realize that if you’re asking this question though, that that ship has sailed already.
However, for readers who have thus far dodged it, then well, if you still haven’t had it by 5 years in, then you’re probably immune, or asymptomatic, or doing everything right. But as it’s hard to know which of those three scenarios you’re living, it’s good to check your lifestyle against: Why Some People Get Sick More (And How To Not Be One Of Them)
And of course: Beyond Supplements: The Real Immune-Boosters!
Now, about long COVID and the chronic fatigue that usually comes with it, then check out: How To Be 7.5x More Likely To Develop Chronic Fatigue Syndrome ← this isn’t just “if you get COVID you are >7.5x more likely to get chronic fatigue syndrome”, by the way. It is also that, but it additionally has practical advice too.
We previously advised, in answer to the question (that we posed ourselves as part of that article) “What if I do get (or already have) long COVID and/or ME/CFS?”, the following:
Well, that is definitely going to suck, but there are still some things that can be done.
Here’s a big one: How To Eat To Beat Chronic Fatigue ← this will not, of course, cure you, but it’s a way of getting maximum nutrition for minimum effort, given that for someone with chronic fatigue, effort is a very finite resource that must be used sparingly
Finally, here are some further resources:
However! That was then and this is now, and science goes marching on, so…
Long COVID lives up your nose and can be removed from there
We are, for the second day in a row*, going to tell you about a serious illness that can be addressed by doing something to the part of you that lives just behind your nose**.
*after yesterday’s The Facial Massage That Keeps Dementia At Bay (it has to do with lymphatic clearance)
**You may be thinking: “but I am a brain in a body and therefore I live just behind my nose by default”, and well, yes, but today we’re not going that far behind your nose; actually just to the deepest part of it.
In few words: Japanese researchers (Dr. Kensuke Nishi et al.) earlier this year (2025, for posterity) did a study (published in March) and found (we’re summarizing and simplifying a lot here):
- Long COVID genetic fragments can, after the main infection battle has been fought and won (by the body), remain deep behind the nose, lodged in the epipharynx (please don’t do this, but just to explain where it is: if you were to poke something up both nostrils simultaneously, the epipharynx is where they would meet).
- These viral remnants are not the virus itself, and so cannot outright cause another infection, but they do consistently annoy the immune system, causing chronic inflammation in the upper respiratory tract, which in turn causes coughing, fatigue, dizziness, brain fog, etc.
- This chronic inflammation can, of course, leave you vulnerable to getting another infection from another source, but that is a separate matter. The point is that these fragments can’t reanimate into an actual virus.
- The researchers wondered if this could be treated with an old Japanese treatment, called epipharyngeal abrasive therapy (EAT), which involves swabbing the area once per week with a cotton swab soaked in 1% zinc chloride solution.
- They found that it could indeed; after 12 weeks the patients showed reduced markers in all relevant things, and significantly reduced symptoms.
- That doesn’t mean it can’t get rid of it entirely—it just means that after 12 weeks, the researchers had results to publish. The investigation itself is ongoing, and it’s likely (but not yet known for sure) that it’ll eliminate it entirely (or at least reduce things to undetectable levels, which is functionally the same in this case).
You can read the paper in full, here: Spatial transcriptomics of the epipharynx in long COVID identifies SARS-CoV-2 signalling pathways and the therapeutic potential of epipharyngeal abrasive therapy
You may be wondering: can I do this at home?
And the answer is: we’re not recommending that, because:
- swabbing that deeply should not be done without expertise; there are sensitive tissues up there
- zinc chloride is also not to be messed around with. As a 1% aqueous solution it’s harmless and even quite “friendly” to your innards, but dry zinc chloride (which includes: the precipitate from an aqueous solution) is corrosive, and you surely do not want that up your nose.
So, we’d recommend instead bringing the study to the attention of your normal healthcare provider, and asking if they can do that.
Meanwhile, for a gentler wash up there, one thing we would recommend (generally, but especially in light of the above) is using a neti pot to rinse (pouring warm saltwater into one nostril and out of the other, then switching sides with a second batch of warm salt water).
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: