How Beneficial Is MCT Oil, Really?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Often derived from coconuts (though it doesn’t have to be), medium-chain triglycerides (MCTs) are trendy… But does the science back the hype?
First, the principle
MCTs are commonly enjoyed because unlike short- or long-chain fatty acids, they can be quickly broken down and either immediately converted quickly and easily into energy, or turned into ketones in the case of a surplus (in the case of true excess, however, it’ll simply be stored as fat).
Most of that involves the liver, so for anyone who wants a refresher on liver health:
How To Unfatty A Fatty Liver ← notwithstanding the title, this is also important knowledge even if your liver is healthy now—if you’d like it to stay healthy, anyway!
You can also read about the ins and outs of glycogen metabolism and the body’s energy-based metabolic processes in general (including the body’s energy processes that go on in the liver), here:
From Apples to Bees, and High-Fructose Cs: Which Sugars Are Healthier, And Which Are Just The Same?
If the liver turns the MCTs into ketones, those ketones will then be used for energy if there is insufficient glucose available (as the body will always use glucose from the blood first, if available, before moving to alternative energy sources such as ketones and/or fat reserves.)
Thus, many people look to ketones as a solution for having enough energy to function while on a very low-carb diet such as the ketogenic diet:
Ketogenic Diet: Burning Fat Or Burning Out?
…which as you’ll recall, does work for short-term weight loss, but brings long-term health risks, so should not be undertaken for long periods of time.
So, does MCT Oil help?
With regard to weight loss, the research is weak and mixed:
- Weak, because often the methodology was shoddy, often there are many factors not controlled-for, and often the sample sizes were small (and also, RCTs by their very nature tend to be quite short-term (often 6, 8, or 12 weeks), whereas heavy reliance on ketones from MCTs may fall into the same long-term problems as the ketogenic diet in general).
- Mixed, because the results varied widely (probably because of the aforementioned problems).
Rather than pick at individual studies, let’s look at this review and meta-analysis of 13 studies, with a combined sample size of 749 people (so you can imagine how small the individual RCTs were):
❝Compared with LCTs, MCTs decreased body weight (-0.51 kg [95% CI-0.80 to -0.23 kg]; P<0.001; I(2)=35%); waist circumference (-1.46 cm [95% CI -2.04 to -0.87 cm]; P<0.001; I(2)=0%), hip circumference (-0.79 cm [95% CI -1.27 to -0.30 cm]; P=0.002; I(2)=0%), total body fat (standard mean difference -0.39 [95% CI -0.57 to -0.22]; P<0.001; I(2)=0%), total subcutaneous fat (standard mean difference -0.46 [95% CI -0.64 to -0.27]; P<0.001; I(2)=20%), and visceral fat (standard mean difference -0.55 [95% CI -0.75 to -0.34]; P<0.001; I(2)=0%).
No differences were seen in blood lipid levels.
Many trials lacked sufficient information for a complete quality assessment, and commercial bias was detected.❞
So, if we’re going to take those numbers at face value, that means a net weight loss, over the course of the trial period, was…
*drumroll*
0.51kg (that’s about 1 lb).
To put that into perspective, if you did nothing else but pee 1 cup of urine before getting weighed, you’d register as having lost 0.25kg (or about ½ lb) by virtue of the bathroom trip alone.
Here’s the paper:
What about cholesterol and heart health?
With regard to cholesterol, MCT oil is touted as improving blood lipids, which means lowering LDL and increasing HDL (within a safe range, anyway).
You’ll remember that the above review concluded “No differences were seen in blood lipid levels”.
It may again be a case of individual studies cancelling each other out. For example…
This study found that it improved lipids in 40 young women as part of a calorie-controlled interventional diet:
This study found that it worsened lipids in 17 young men, worse even than taking an equivalent amount of sunflower oil:
In short, it’s a gamble.
It may be good for insulin sensitivity, though
This one seems to be specific to people with type 2 diabetes. The paper heading says it all, but we include the link in case you want to know the details (the short version is, it improved insulin sensitivity in diabetic subjects only (not others), and didn’t affect anything else that was measured:
The sample size was small (20 people total, of whom 10 had diabetes), and the next study was with 40 people, this time moderately overweight and all with type 2 diabetes:
Want to try some?
We don’t sell it, but here for your convenience is an example product on Amazon 😎
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Healthy Butternut Macaroni Cheese

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A comfort food classic, healthy and plant-based, without skimping on the comfort.
You will need
- ½ butternut squash, peeled and cut into small pieces (if buying ready-chopped, this should be about 1 lb)
- 1 onion, chopped
- ¼ bulb garlic
- 2 tbsp extra virgin olive oil
- 12 oz (or thereabouts) wholegrain macaroni, or similar pasta shape (even penne works fine—which is good, as it’s often easier to buy wholegrain penne than wholegrain macaroni) (substitute with a gluten-free pasta such as buckwheat pasta, if avoiding gluten)
- 6 oz (or thereabouts) cashews, soaked in hot water for at least 15 minutes (but longer is better)
- ½ cup milk (your preference what kind; we recommend hazelnut for its mellow nutty flavor)
- 3 tbsp nutritional yeast
- Juice of ½ lemon
- 2 tsp black pepper, coarse ground
- ½ tsp MSG, or 1 tsp low-sodium salt
- Optional: smoked paprika, to serve
Note: if you are allergic to nuts, please accept our apologies that there’s no substitution available in this one. Simply put, removing the cashews would mean changing most of the rest of the recipe to compensate, so there’s no easy “or substitute with…” that we can mention. We’ll have to find/develop a good healthy plant-based no-nuts recipe for you at a later date.
Method
(we suggest you read everything at least once before doing anything)
1) Preheat the oven to 400℉ / 200℃.
2) Combine the butternut squash, onion, and garlic with the olive oil, in a large roasting tin, tossing thoroughly to ensure an even coat of oil. Roast them for about 25 minutes until soft.
3) Cook the macaroni while you wait (this should take about 10 minutes or so in salted water), drain, and rinse thoroughly in cold water, before setting aside. This cooling increases the pasta’s resistant starch content (that’s good, for your gut and for your blood sugars, and thus also for your heart and brain), and it will maintain this benefit even when we reheat it later.
4) Drain the cashews, and tip them into a high-speed blender with the milk, and process until smooth. Add the roasted vegetables and the remaining ingredients apart from the pasta, and continue to process until again smooth. You can add a little more milk if you need to, but go easy with it.
5) Heat the sauce (that you just made in the food processor) gently in a saucepan, and refresh the pasta by pouring a kettle of boiling water through it in a colander.
6) Optional: combine the pasta and sauce in an ovenproof dish or cast iron pan, and give it a few minutes under the hottest grill (or browning iron, if you have such) your oven can muster. Alternatively, use a culinary blowtorch, if you have one.
7) Serve; and if you didn’t do the optional step above, this means combining the pasta and sauce. You can also dust the top with some extra seasonings if you like. Smoked paprika works well for this.

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Butternut Squash vs Pumpkin – Which is Healthier?
- Cashew Nuts vs Coconut – Which is Healthier?
- The Many Health Benefits Of Garlic
- Black Pepper’s Impressive Anti-Cancer Arsenal (And More)
- Sea Salt vs MSG – Which is Healthier?
Take care!
Share This Post
-

100 Things Productive People Do – by Nigel Cumberland
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This is a book of a hundred small chapters (the book is 396 pages, so 2–3 pages per chapter) which makes for a feeling of quick reading, and definitely gives an option of “light bites”, dipping into the book here and there.
Cumberland offers a wide range of practical wisdom here, and while the book is (per the title) focused on productivity, it also includes all due weight to not burning out and/or breaking down. Because things productive people do does not, it turns out, include working themselves directly into an early grave.
But—despite the author’s considerable and obvious starting point of social privilege—nor is this a tome of “offer your genius leadership and otherwise just coast while everyone does your work for you”, either. This is a “brass tacks” book and highly relatable whether your to-do list most prominently features “personally manage the merger of these Fortune 500 companies” or “sort out that junk in the spare room”
Bottom line: we’d be surprised if this book with 100 pieces of advice failed to bring you enough value to more than pay for itself!
Pick up your copy of 100 Things Productive People Do from Amazon today!
Share This Post
-

Rewire Your OCD Brain – by Dr. Catherine Pittman & Dr. William Youngs
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
OCD is just as misrepresented in popular media as many other disorders, and in this case, it’s typically not “being a neat freak” or needing to alphabetize things, so much as having uncontrollable obsessive intrusive thoughts, and often in response to those, unwanted compulsions. This can come from unchecked spiralling anxiety, and/or PTSD, for example.
What Drs. Pittman & Young offer is an applicable set of solutions, to literally rewire the brain (insofar as synapses can be considered neural wires). Leveraging neuroplasticity to work with us rather than against us, the authors talk us through picking apart the crossed wires, and putting them back in more helpful ways.
This is not, by the way, a book of CBT, though it does touch on that too.
Mostly, the book explains—clearly and simply and sometimes with illustrations—what is going wrong for us neurologically, and how to neurologically change that.
Bottom line: whether you have OCD or suffer from anxiety or just need help dealing with obsessive thoughts, this book can help a lot in, as the title suggests, rewiring that.
Click here to check out Rewire Your OCD Brain, and banish obsessive thoughts!
Share This Post

Related Posts
-

The Knowledge That Harvard Medical School’s Clinical Instructor Dr. Monique Tello Thinks Everyone SHOULD Have About Heart Health
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Anyone (who has not had a double mastectomy, anyway) can get breast cancer.
Breast cancer, if diagnosed early (before it spreads), has a 98% survival rate.
That survival rate drops to 31% if diagnosed after it has spread through the body.
(The US CDC’s breast cancer “stat bite” page has more stats and interactive graphs, so click here to see those charts and get the more detailed low-down on mortality/survival rates with various different situations)
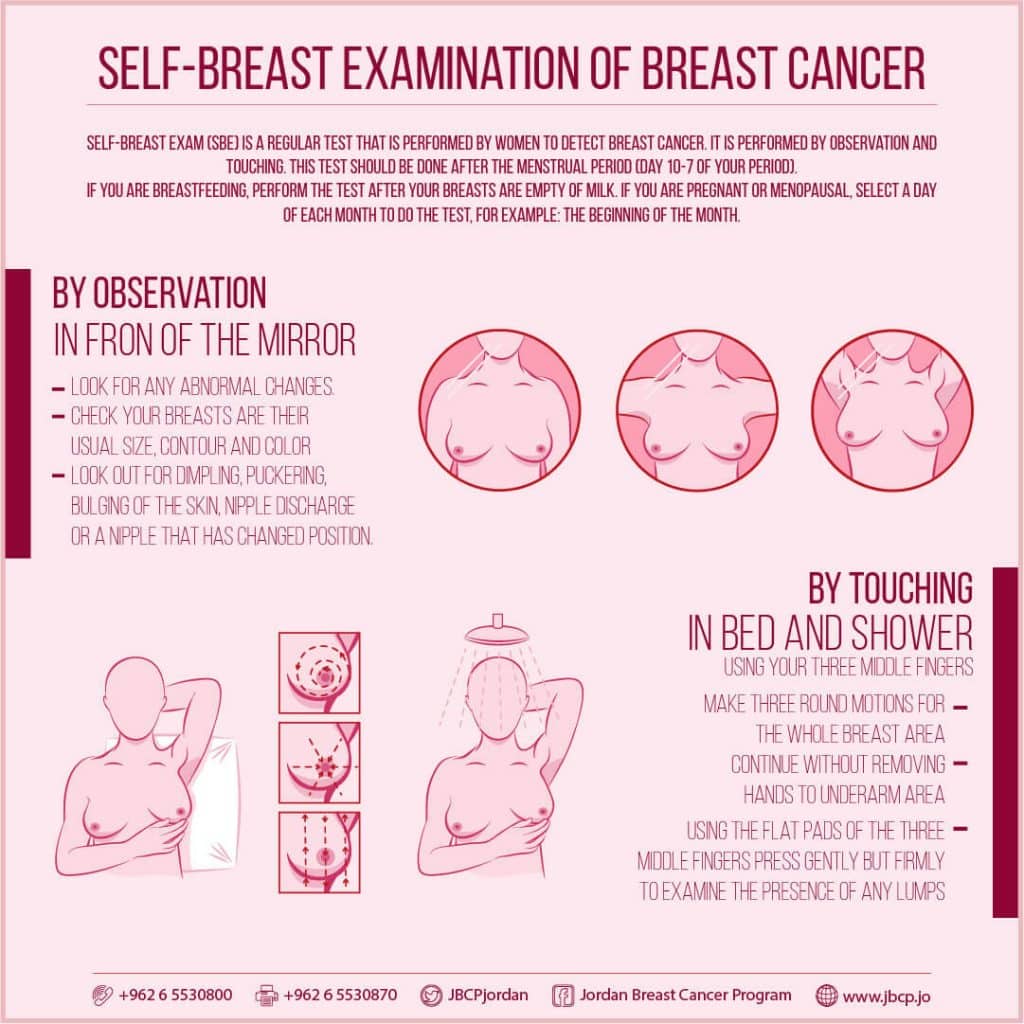
We think that the difference between 98% and 31% survival rates is more than enough reason to give ourselves a monthly self-check at the very least! You’ve probably seen how-to diagrams before, but here are instructions for your convenience:
This graphic created by the Jordan Breast Cancer Program (check them out, as they have lots of resources)

If you don’t have the opportunity to take matters into your own hands right now, rather than just promise yourself “I’ll do that later”, take this free 4-minute Breast Health Assessment from Aurora Healthcare. Again, we think the difference early diagnosis can make to your survival chances make these tests well worth it.
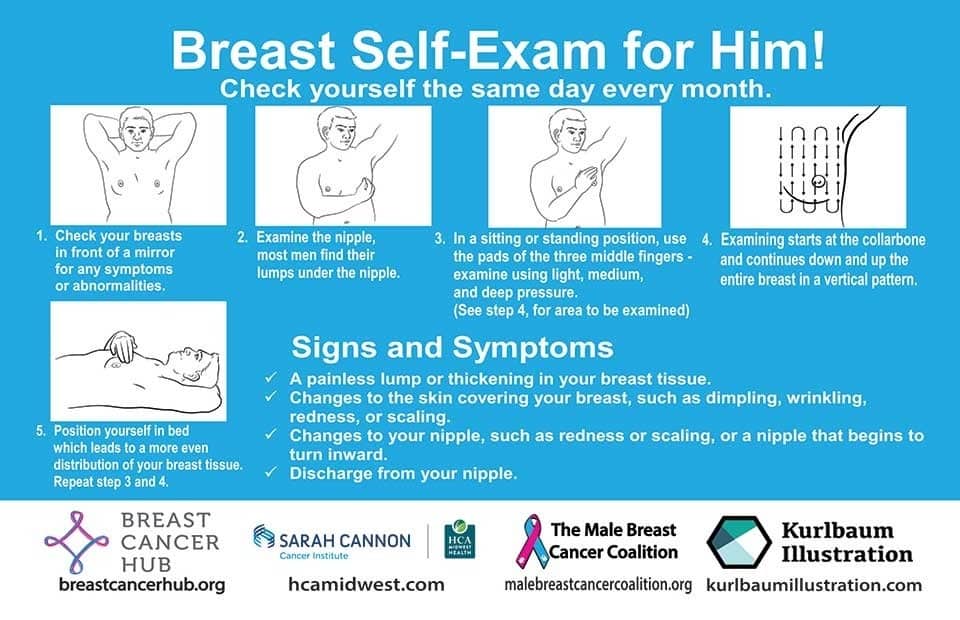
Lest we forget, men can also get breast cancer (the CDC has a page for men too), especially if over 50. But how do you check for breast cancer, when you don’t have breasts in the commonly-understood sense of the word?

So take a moment to do this (yes, really actually do it!), and set a reminder in your calendar to repeat it monthly—there really is no reason not to! Take care of yourself; you’re important.
Pssst! Did you scroll past the diagrams, looking for the online 4-minute test promised by the subtitle? If so, scroll back up; the link is in the middle!
Harvard Medical School’s Clinical Instructor’s Five-Point Plan for Heart Health
Dr. Monique Tello, M.D., M.P.H., is a practicing physician at Massachusetts General Hospital, director of research and academic affairs for the MGH DGM Healthy Lifestyle Program, clinical instructor at Harvard Medical School, and author of the evidence-based lifestyle change guide Healthy Habits for Your Heart.

Here are what she says are the five most important factors to help keep your ticker ticking:
5. Have (at most) a moderate alcohol intake! While there are polyphenols such as resveratrol in red wine that could boost heart health, there’s so little per glass that you may need 100–1000 glasses to get the dosage that provides benefits in mouse studies. If you’re not a mouse, it may not be as beneficial, and Dr. Tello recommends drinking no more than one glass per day of any alcohol. What constitutes a glass? It varies from one kind of drink to another, so here’s a handy guide.
4. Don’t smoke. Best of all to never start. But if you did, quit. Simple as that. There is no healthy amount of smoking. While paradoxically, quitting smoking may of course be stressful to you, the long term gains are considered more than worth it. As with all advice, do consult your own physician for guidance, as individual circumstances may vary, and that may change the best approach for you.
3. Maintain a healthy body weight. While BMI (Body Mass Index) is not a perfect system, it’s a system in popular use, and Dr. Tello recommends keeping a BMI between 18.5 and 24.9.
What’s your BMI? It takes into account your height and weight; here’s a Quick BMI Calculator for your convenience.
2. Keep a healthy level of physical activity—which ideally means at least 30 minutes per day vigorous activity, but obviously if you’re not used to this, take it slowly and build up over time. Even just small lifestyle changes (walking where possible, taking the stairs instead of the elevator where possible, etc) can add up to a big difference.
1. Enjoy a healthy diet. This is the single most important thing, and the best modern scientific consensus holds that the best diet contains plenty of vegetables, fruits and nuts, whole grains, and omega-3 fatty acids, while it avoids processed meats, sugar-sweetened beverages, trans fats (what are trans fats?), and too much sodium.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Reverse Inflammation Naturally – by Dr. Michelle Honda
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This book is in some ways not as marketable as some; it doesn’t have lots of colorful healthy food on the cover; it doesn’t even have a “woman laughing alone with salad” (you know the stock photo trope), let alone someone looking glamorous in a labcoat with a stethoscope draped over their shoulder despite listening to hearts not being a regular part of their job as an immunologist or such.
What it does have, instead, is a lot of very useful information, and much more than you’ll usually find in a book for laypeople.
For example, you probably know that for fighting inflammation, a green salad is better than a cheeseburger, say, and a black coffee is better than a glass of wine.
But do you know about the roles, for good or ill, of prostaglandins and linoleic fats vs dietary fats? How about delta-6-desaturase? Neu5Gc and arachidonic acid?
Dr. Honda demystifies all of these and more, as well as talking about the impacts of very many foods and related habits on various different inflammation-based disease. And of course, almost all disease involves some kind of inflammation (making fighting inflammation one of the best things you can do for your overall disease-avoidance strategy!), but she singles out some of the most relevant, as per the list on the front cover.
She also talks a lot of “pharmacy in your kitchen”, in other words, what herbs, spices, and plant extracts we can enjoy for (evidence-based!) benefits on top of our default healthy diet free (or at least mostly free, for surely none of us are perfect) from inflammatory agents.
Not content with merely giving a huge amount of information, she also gives recipes and a meal plan, but honestly, it’s the informational chapters that are the real value of the book.
Bottom line: if you’d like to reduce your body’s inflammation levels (and/or perhaps those of a loved one for whom you cook), then this book will be an invaluable resource.
Click here to check out Reverse Inflammation Naturally, and reverse inflammation naturally!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Patient Underwent One Surgery but Was Billed for Two. Even After Being Sued, She Refused To Pay.
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Jamie Holmes says a surgery center tried to make her pay for two operations after she underwent only one. She refused to buckle, even after a collection agency sued her last winter.
Holmes, who lives in northwestern Washington state, had surgery in 2019 to have her fallopian tubes tied, a permanent birth-control procedure that her insurance company agreed ahead of time to cover.
During the operation, while Holmes was under anesthesia, the surgeon noticed early signs of endometriosis, a common condition in which fibrous scar tissue grows around the uterus, Holmes said. She said the surgeon later told her he spent about 15 minutes cauterizing the troublesome tissue as a precaution. She recalls him saying he finished the whole operation within the 60 minutes that had been allotted for the tubal ligation procedure alone.
She said the doctor assured her the extra treatment for endometriosis would cost her little, if anything.
Then the bill came.
The Patient: Jamie Holmes, 38, of Lynden, Washington, who was insured by Premera Blue Cross at the time.
Medical Services: A tubal ligation operation, plus treatment of endometriosis found during the surgery.
Service Provider: Pacific Rim Outpatient Surgery Center of Bellingham, Washington, which has since been purchased, closed, and reopened under a new name.
Total Bill: $9,620. Insurance paid $1,262 to the in-network center. After adjusting for prices allowed under the insurer’s contract, the center billed Holmes $2,605. A collection agency later acquired the debt and sued her for $3,792.19, including interest and fees.
What Gives: The surgery center, which provided the facility and support staff for her operation, sent a bill suggesting that Holmes underwent two separate operations, one to have her tubes tied and one to treat endometriosis. It charged $4,810 for each.
Holmes said there were no such problems with the separate bills from the surgeon and anesthesiologist, which the insurer paid.
Holmes figured someone in the center’s billing department mistakenly thought she’d been on the operating table twice. She said she tried to explain it to the staff, to no avail.
She said it was as if she ordered a meal at a fast-food restaurant, was given extra fries, and then was charged for two whole meals. “I didn’t get the extra burger and drink and a toy,” she joked.
Her insurer, Premera Blue Cross, declined to pay for two operations, she said. The surgery center billed Holmes for much of the difference. She refused to pay.
Holmes said she understands the surgery center could have incurred additional costs for the approximately 15 minutes the surgeon spent cauterizing the spots of endometriosis. About $500 would have seemed like a fair charge to her. “I’m not opposed to paying for that,” she said. “I am opposed to paying for a whole bunch of things I didn’t receive.”
The physician-owned surgery center was later purchased and closed by PeaceHealth, a regional health system. But the debt was turned over to a collection agency, SB&C, which filed suit against Holmes in December 2023, seeking $3,792.19, including interest and fees.
The collection agency asked a judge to grant summary judgment, which could have allowed the company to garnish wages from Holmes’ job as a graphic artist and marketing specialist for real estate agents.
Holmes said she filed a written response, then showed up on Zoom and at the courthouse for two hearings, during which she explained her side, without bringing a lawyer. The judge ruled in February that the collection agency was not entitled to summary judgment, because the facts of the case were in dispute.
More From Bill Of The Month
- Her Hearing Implant Was Preapproved. Nonetheless, She Got $139,000 Bills for Months.
- It’s Called an Urgent Care Emergency Center — But Which Is It?
- He Fell Ill on a Cruise. Before He Boarded the Rescue Boat, They Handed Him the Bill.
Representatives of the collection agency and the defunct surgery center declined to comment for this article.
Sabrina Corlette, co-director of Georgetown University’s Center on Health Insurance Reforms, said it was absurd for the surgery center to bill for two operations and then refuse to back down when the situation was explained. “It’s like a Kafka novel,” she said.
Corlette said surgery center staffers should be accustomed to such scenarios. “It is quite common, I would think, for a surgeon to look inside somebody and say, ‘Oh, there’s this other thing going on. I’m going to deal with it while I’ve got the patient on the operating table.’”
It wouldn’t have made medical or financial sense for the surgeon to make Holmes undergo a separate operation for the secondary issue, she said.
Corlette said that if the surgery center was still in business, she would advise the patient to file a complaint with state regulators.
The Resolution: So far, the collection agency has not pressed ahead with its lawsuit by seeking a trial after the judge’s ruling. Holmes said that if the agency continues to sue her over the debt, she might hire a lawyer and sue them back, seeking damages and attorney fees.
She could have arranged to pay off the amount in installments. But she’s standing on principle, she said.
“I just got stonewalled so badly. They treated me like an idiot,” she said. “If they’re going to be petty to me, I’m willing to be petty right back.”
The Takeaway: Don’t be afraid to fight a bogus medical bill, even if the dispute goes to court.
Debt collectors often seek summary judgment, which allows them to garnish wages or take other measures to seize money without going to the trouble of proving in a trial that they are entitled to payments. If the consumers being sued don’t show up to tell their side in court hearings, judges often grant summary judgment to the debt collectors.
However, if the facts of a case are in dispute — for example, because the defendant shows up and argues she owes for just one surgery, not two — the judge may deny summary judgment and send the case to trial. That forces the debt collector to choose: spend more time and money pursuing the debt or drop it.
“You know what? It pays to be stubborn in situations like this,” said Berneta Haynes, a senior attorney for the National Consumer Law Center who reviewed Holmes’ bill for KFF Health News.
Many people don’t go to such hearings, sometimes because they didn’t get enough notice, don’t read English, or don’t have time, she said.
“I think a lot of folks just cave” after they’re sued, Haynes said.
Emily Siner reported the audio story.
After six years, we’ll have a final installment with NPR of our Bill of the Month project in the fall. But Bill of the Month will continue at KFF Health News and elsewhere. We still want to hear about your confusing or outrageous medical bills. Visit Bill of the Month to share your story.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: