

Homeopathy: Evidence So Tiny That It’s Not there?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Homeopathy: Evidence So Tiny That It’s Not There?
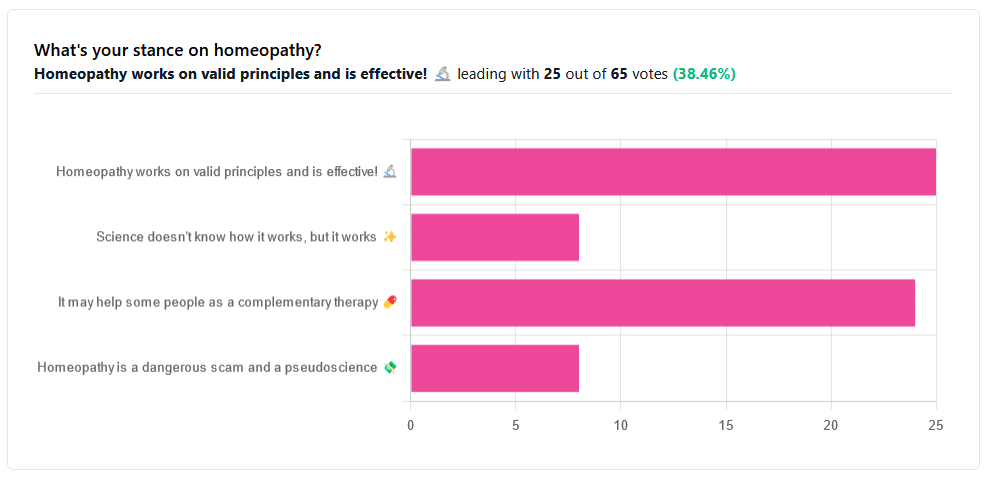
Yesterday, we asked you your opinions on homeopathy. The sample size of responses was a little lower than we usually get, but of those who did reply, there was a clear trend:
- A lot of enthusiasm for “Homeopathy works on valid principles and is effective”
- Near equal support for “It may help some people as a complementary therapy”
- Very few people voted for “Science doesn’t know how it works, but it works”; this is probably because people who considered voting for this, voted for the more flexible “It may help some people as a complementary therapy” instead.
- Very few people considered it a dangerous scam and a pseudoscience.
So, what does the science say?
Well, let us start our investigation by checking out the position of the UK’s National Health Service, an organization with a strong focus on providing the least expensive treatments that are effective.
Since homeopathy is very inexpensive to arrange, they will surely want to put it atop their list of treatments, right?
❝Homeopathy is a “treatment” based on the use of highly diluted substances, which practitioners claim can cause the body to heal itself.
There’s been extensive investigation of the effectiveness of homeopathy. There’s no good-quality evidence that homeopathy is effective as a treatment for any health condition.❞
The NHS actually has a lot more to say about that, and you can read their full statement here.
But that’s just one institution. Here’s what Australia’s National Health and Medical Research Council had to say:
❝There was no reliable evidence from research in humans that homeopathy was effective for treating the range of health conditions considered: no good-quality, well-designed studies with enough participants for a meaningful result reported either that homeopathy caused greater health improvements than placebo, or caused health improvements equal to those of another treatment❞
You can read their full statement here.
The American FDA, meanwhile, have a stronger statement:
❝Homeopathic drug products are made from a wide range of substances, including ingredients derived from plants, healthy or diseased animal or human sources, minerals and chemicals, including known poisons. These products have the potential to cause significant and even permanent harm if they are poorly manufactured, since that could lead to contaminated products or products that have potentially toxic ingredients at higher levels than are labeled and/or safe, or if they are marketed as substitute treatments for serious or life-threatening diseases and conditions, or to vulnerable populations.❞
You can read their full statement here.
Homeopathy is a dangerous scam and a pseudoscience: True or False?
False and True, respectively, mostly.
That may be a confusing answer, so let’s elaborate:
- Is it dangerous? Mostly not; it’s mostly just water. However, two possibilities for harm exist:
- Careless preparation could result in a harmful ingredient still being present in the water—and because of the “like cures like” principle, many of the ingredients used in homeopathy are harmful, ranging from heavy metals to plant-based neurotoxins. However, the process of “ultra-dilution” usually removes these so thoroughly that they are absent or otherwise scientifically undetectable.
- Placebo treatment has its place, but could result in “real” treatment going undelivered. This can cause harm if the “real” treatment was critically needed, especially if it was needed on a short timescale.
- Is it a scam? Probably mostly not; to be a scam requires malintent. Most practitioners probably believe in what they are practising.
- Is it a pseudoscience? With the exception that placebo effect has been highly studied and is a very valid complementary therapy… Yes, aside from that it is a pseudoscience. There is no scientific evidence to support homeopathy’s “like cures like” principle, and there is no scientific evidence to support homeopathy’s “water memory” idea. On the contrary, they go against the commonly understood physics of our world.
It may help some people as a complementary therapy: True or False?
True! Not only is placebo effect very well-studied, but best of all, it can still work as a placebo even if you know that you’re taking a placebo… Provided you also believe that!
Science doesn’t know how it works, but it works: True or False?
False, simply. At best, it performs as a placebo.
Placebo is most effective when it’s a remedy against subjective symptoms, like pain.
However, psychosomatic effect (the effect that our brain has on the rest of our body, to which it is very well-connected) can mean that placebo can also help against objective symptoms, like inflammation.
After all, our body, directed primarily by the brain, can “decide” what immunological defenses to deploy or hold back, for example. This is why placebo can help with conditions as diverse as arthritis (an inflammatory condition) or diabetes (an autoimmune condition, and/or a metabolic condition, depending on type).
Here’s how homeopathy measures up, for those conditions:
(the short answer is “no better than placebo”)
Homeopathy works on valid principles and is effective: True or False?
False, except insofar as placebo is a valid principle and can be effective.
The stated principles of homeopathy—”like cures like” and “water memory”—have no scientific basis.
We’d love to show the science for this, but we cannot prove a negative.
However, the ideas were conceived in 1796, and are tantamount to alchemy. A good scientific attitude means being open-minded to new ideas and testing them. In homeopathy’s case, this has been done, extensively, and more than 200 years of testing later, homeopathy has consistently performed equal to placebo.
In summary…
- If you’re enjoying homeopathic treatment and that’s working for you, great, keep at it.
- If you’re open-minded to enjoying a placebo treatment that may benefit you, be careful, but don’t let us stop you.
- If your condition is serious, please do not delay seeking evidence-based medical treatment.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How Much Can Hypnotherapy Really Do?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Sit Back, Relax, And…

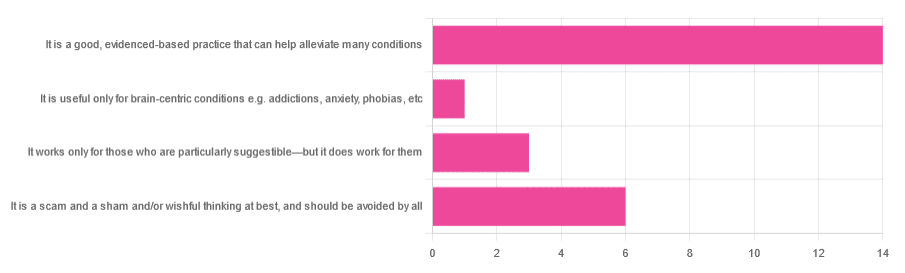
In Tuesday’s newsletter, we asked you for your opinions of hypnotherapy, and got the above-depicted, below-described, set of responses:
- About 58% said “It is a good, evidenced-based practice that can help alleviate many conditions”
- Exactly 25% said “It is a scam and sham and/or wishful thinking at best, and should be avoided by all”
- About 13% said “It works only for those who are particularly suggestible—but it does work for them”
- One (1) person said “It is useful only for brain-centric conditions e.g. addictions, anxiety, phobias, etc”
So what does the science say?
Hypnotherapy is all in the patient’s head: True or False?
True! But guess which part of your body controls much of the rest of it.
So while hypnotherapy may be “all in the head”, its effects are not.
Since placebo effect, nocebo effect, and psychosomatic effect in general are well-documented, it’s quite safe to say at the very least that hypnotherapy thus “may be useful”.
Which prompts the question…
Hypnotherapy is just placebo: True or False?
False, probably. At the very least, if it’s placebo, it’s an unusually effective placebo.
And yes, even though testing against placebo is considered a good method of doing randomized controlled trials, some placebos are definitely better than others. If a placebo starts giving results much better than other placebos, is it still a placebo? Possibly a philosophical question whose answer may be rooted in semantics, but happily we do have a more useful answer…
Here’s an interesting paper which: a) begins its abstract with the strong, unequivocal statement “Hypnosis has proven clinical utility”, and b) goes on to examine the changes in neural activity during hypnosis:
Brain Activity and Functional Connectivity Associated with Hypnosis
It works only for the very suggestible: True or False?
False, broadly. As with any medical and/or therapeutic procedure, a patient’s expectations can affect the treatment outcome.
And, especially worthy of note, a patient’s level of engagement will vastly affect it treatment that has patient involvement. So for example, if a doctor prescribes a patient pills, which the patient does not think will work, so the patient takes them intermittently, because they’re slow to get the prescription refilled, etc, then surprise, the pills won’t get as good results (since they’re often not being taken).
How this plays out in hypnotherapy: because hypnotherapy is a guided process, part of its efficacy relies on the patient following instructions. If the hypnotherapist guides the patient’s mind, and internally the patient is just going “nope nope nope, what a lot of rubbish” then of course it will not work, just like if you ask for directions in the street and then ignore them, you won’t get to where you want to be.
For those who didn’t click on the above link by the way, you might want to go back and have a look at it, because it included groups of individuals with “high/low hypnotizability” per several ways of scoring such.
It works only for brain-centric things, e.g. addictions, anxieties, phobias, etc: True or False?
False—but it is better at those. Here for example is the UK’s Royal College of Psychiatrists’ information page, and if you go to “What conditions can hypnotherapy help to treat”, you’ll see two broad categories; the first is almost entirely brain-stuff; the second is more varied, and includes pain relief of various kinds, burn care, cancer treatment side effects, and even menopause symptoms. Finally, warts and other various skin conditions get their own (positive) mention, per “this is possible through the positive effects hypnosis has on the immune system”:
RCPsych | Hypnosis And Hypnotherapy
Wondering how much psychosomatic effect can do?
You might like this previous article; it’s not about hypnotherapy, but it is about the difference the mind can make on physical markers of aging:
Aging, Counterclockwise: When Age Is A Flexible Number
Take care!
Share This Post
-

Quercetin Quinoa Probiotic Salad
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This quercetin-rich salad is a bit like a tabbouleh in feel, with half of the ingredients switched out to maximize phenolic and gut-healthy benefits.
You will need
- ½ cup quinoa
- ½ cup kale, finely chopped
- ½ cup flat leaf parsley, finely chopped
- ½ cup green olives, thinly sliced
- ½ cup sun-dried tomatoes, roughly chopped
- 1 pomegranate, peel and pith removed
- 1 preserved lemon, finely chopped
- 1 oz feta cheese or plant-based equivalent, crumbled
- 1 tsp black pepper, coarse ground
- 1 tbsp capers
- 1 tbsp chia seeds
- 1 tbsp extra virgin olive oil
Note: you shouldn’t need salt or similar here, because of the diverse gut-healthy fermented products bringing their own salt with them
Method
(we suggest you read everything at least once before doing anything)
1) Rinse the quinoa, add the tbsp of chia seeds, cook as normal for quinoa (i.e. add hot water, bring to boil, simmer for 15 minutes or so until pearly and tender), carefully (don’t lose the chia seeds; use a sieve) drain and rinse with cold water to cool. Shake off excess water and/or pat dry on kitchen paper if necessary.
2) Mix everything gently but thoroughly.
3) Serve:

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Tasty Tabbouleh with Tahini ← in case you want an actual tabbouleh
- Making Friends With Your Gut (You Can Thank Us Later)
- Fight Inflammation & Protect Your Brain, With Quercetin
Take care!
Share This Post
-
Some women start menopause after surgery or medical treatment. Here’s how it’s different
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
For most women, menopause occurs naturally around the age of 49. In the lead up to menopause, the quality and quantity of eggs declines over time. Then the ovaries stop releasing eggs completely.
At this time, the ovaries also stop producing the sex hormones oestrogen and progesterone. This causes menstrual periods to end. When you clock 12 months of no periods, you’re in menopause.
But some women will start menopause quickly after having their ovaries removed in surgery. Others will transition to menopause over a longer timeframe if medical treatments, such as chemotherapy or radiotherapy, damage their ovaries.
So what can you expect from menopause due to surgery or medical treatments?
MomentoJpeg/Getty Images What treatments can cause menopause?
Surgical menopause occurs when women have their ovaries removed to treat conditions such as ovarian cancer.
Some women with a genetic predisposition to ovarian and breast cancer, such as those like Angelina Jolie who carry the BRCA1 gene, may also have their ovaries removed to stop the production of oestrogen. This reduces the risk of ovarian and breast cancers, which are considered oestrogen-dependent cancers.
Other pelvic surgery can damage the ovaries and trigger menopause, such as removal of ovarian cysts or treatment for endometriosis.
Medical treatments that severely damage or are toxic to the ovaries can also trigger menopause. These include chemotherapy or radiotherapy for cancer, and treatment for rheumatological conditions such as lupus.
Whether you become menopausal after medical treatment will depend on your age, underlying ovarian reserve, as well as the type and dose of chemotherapy or radiotherapy. Younger women generally have greater ovarian stores so can withstand more damage.
When does it happen? How is it diagnosed?
Menopause due to medical treatment may occur earlier than the typical age of natural menopause. When menopause occurs between 40 and 45 years, it’s called early menopause. Around 12% of women will have early menopause.
Before 40, early menopause is called “premature ovarian insufficiency”. This is because for women whose periods spontaneously stop, there’s still a chance of their ovarian function returning. But this is less likely if periods stop due to the effect of medical treatments. And it’s impossible after surgical menopause. Around 4% of women have premature ovarian insufficiency.
The diagnosis of surgical menopause is clear. But making a diagnosis of menopause after medical treatments can be more difficult. The diagnosis is based on four months or more of no or irregular menstrual periods, plus a high follicle-stimulating hormone level, which is determined using a blood test.
What are the symptoms? How do they differ?
Symptoms of oestrogen deficiency, such as hot flushes, usually start quickly after surgical menopause. Other symptoms such as vaginal dryness may develop more slowly. Symptoms of surgical menopause are often more severe than natural menopause.
But every person’s experience is different. And symptoms can vary within and between people. It can also be hard to tell what symptoms are due to menopause and what are due to the underlying health problem or treatment, such as the effects of chemotherapy on cognition.
Low oestrogen from premature ovarian insufficiency can cause vaginal dryness, reduced libido, muscle decline and bone loss, and may also impair brain function. It can also increase risk risk of heart disease and stroke, with a higher risk after surgical menopause than spontaneous premature menopause.
Premature ovarian insufficiency can can also result in poorer mental health and quality of life, and can impact your ability to work.
Women with surgical menopause cannot become pregnant, while women with premature ovarian insufficiency are unlikely to fall pregnant naturally.
How is it treated?
Our previous research has shown women with early menopause and premature ovarian insufficiency often receive poor health care. There is a large variation of quality between health providers.
To assist health-care professionals provide best-practice care, in 2024 we updated the evidence-based guidelines with 145 recommendations to treat early menopause and premature ovarian insufficiency.
Hormone-replacement therapy (HRT), which replaces the missing oestrogen (plus progesterone if you still have your uterus), is the mainstay of treatment for women with premature ovarian insufficiency and early menopause.
Women who have undergone surgical menopause or are experiencing premature ovarian insufficiency can consider HRT for symptom relief and bone protection.
However, HRT cannot be used if you have certain health conditions such as hormone-sensitive breast cancers.
It’s important you talk to you health-care provider about the pros and cons of HRT in your situation.
Other treatment options include:
- vaginal oestrogen, which can be helpful for vaginal dryness
- cognitive behavioural therapy (CBT), which be helpful for managing hot flushes, sleep and mood.
Although Chinese herbal medicine may alleviate menopausal symptoms in some women, overall there isn’t enough scientific evidence that complementary therapies can effectively manage premature ovarian insufficiency.
Health practitioners should talk to patients about the likely symptoms and risks of surgical menopause and premature ovarian insufficiency before starting any treatments that can cause these conditions.
Options to minimise these risks and preserve fertility should also be discussed and may require a referral to a specialist.
Carolyn Ee, Associate Professor, Cancer Survivorship and Primary Care, Caring Futures Institute, Flinders University; Western Sydney University and Amanda Vincent, Adjunct Clinical Associate Professor and Endocrinologist, Monash University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post




Related Posts
-
5 Ways To Lose Fat Without Losing Muscle
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It can seem like a paradox, trying to lose weight and gain it (in muscle) at the same time. But it can be done:
How to do it
Chances are, if you’re looking for change that you’re not currently getting, it won’t be by doing what you’ve been doing already. Thus:
- Accept the change you hate most: the change you resist most is usually what you need most (precisely because it’s what’s missing, because you’ve been avoiding it). Avoiding discomfort keeps you stuck. Real progress often comes from doing what feels hardest.
- Track everything: it gives you the data to make informed decisions. Whether it’s logging macros, using hand portions, or taking food photos, tracking brings clarity and helps tailor your plan. Otherwise, you are guessing. And that can be fine for maintaining a stable status quo that you’re happy with, but not for effecting change.
- Diet for fat loss, train for muscle: nutrition drives fat loss; training builds muscle. Worry less about cardio and focus on strength training with progressive overload. Rest when needed, and train with intent to preserve/define muscle.
- Create daily consistency: simple habits done consistently yield lasting results. Keep your routine steady across training (while still integrating rest days to allow recovery), which coupled with the “track everything” dictum, will reduce guesswork, and reveal what actually works over time.
- What you put first gets priority: tackle key habits early in the day. Prioritize strength training over cardio, and do your most important exercises first in your workout to get your best effort when it matters most.
For more on each of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Can You Gain Muscle & Lose Fat At The Same Time? ← for our own main feature on this topic, with much more specificity than provided in the video.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Here’s why morning exercise feels so hard
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Your alarm goes off. Somehow you manage to get dressed, drag yourself to the gym, and start squatting.
But why does it feel so hard? Your legs are heavy and the weight you lifted only a couple of days ago – in the afternoon – feels almost impossible.
No, you’re not imagining it. There’s a large body of evidence to suggest most of us are stronger, more powerful, and have better endurance later in the day.
There are several reasons exercising can feel much harder first thing in the morning. Here’s why, and how you can adjust to morning exercise if you need to.
Ketut Subiyanto/Pexels Your circadian rhythm affects your workout
Your body has a natural 24-hour clock that regulates hormones, body temperature and when you feel most awake or ready for sleep.
This clock is called your circadian rhythm. It is controlled by the brain but can also be influenced by external factors such as sunlight. This might explain why exercising in the morning in winter can be especially hard for some of us.
Research shows your circadian rhythm is clearly linked to exercise performance, which tends to follow a daily pattern.
Most people reach their peak between 4 and 7pm. This means we tend to be stronger, faster and more powerful in the afternoon and early evening.
We don’t know exactly why. But there are a few potential explanations.
Matt Garrow/The Conversation. Adapted from Delos, CC BY Body temperature
Your core body temperature is at its lowest around 5am, and steadily increases across the day. When your body temperature rises, your muscles contract more efficiently. We think this is part of the reason people are typically stronger and more powerful later in the day.
Hormonal fluctuations
Insulin – the hormone that regulates blood sugar (glucose) levels – tends to be highest in the morning. This leads to a decrease in blood sugar, meaning less glucose your body can use as fuel, likely affecting how hard you can push.
Nervous system function
While we don’t know exactly why, there is some evidence to suggest your nervous system is better at sending signals to your muscles throughout the day. This allows you to use more of your muscle fibres during exercise, essentially making you stronger.
But what if I’m a morning person?
Your sleep chronotype can also affect exercise performance.
This describes your natural inclination for sleep and wakefulness at certain parts of the day – basically whether you’re a “morning person” (an “early bird”), or feel more productive and alert in the evening (a “night owl”).
Research shows night owls with a late chronotype do notably worse when exercising in the morning, compared to people with an early chronotype.
While we don’t know why this is the case, it might be that night owls experience smaller fluctuations in hormones and temperature throughout the day – although this is just speculation.
Interestingly, being sleep deprived seems to affect physical performance in the afternoon more than in the morning. So if you’re staying up late and not getting much sleep, you may actually find it easier to exercise the next morning than the next afternoon.
So, does timing matter?
Whatever time of day, if you can feel yourself working you will make progress – for example, increasing muscle strength and improving aerobic fitness and heart health.
So if you’re exercising to get bigger, stronger and fitter, the timing doesn’t actually matter.
Besides, when we exercise often comes down to motivation and convenience. If you like to exercise earlier in the day and that suits you best, there’s no reason to change.
But you can adapt if you need
If you have a sporting event coming up in the morning – and you usually train in the afternoon – you might want to prepare by doing some early exercise so you’re at your peak.
There is evidence to suggest that repeatedly training in the morning can close the gap between your afternoon and morning performance.
Basically, your body can get used to exercising at a particular time, although it will likely take a few weeks to adapt.
Finally, if you find exercising close to bedtime makes you feel too alert and is disrupting your sleep, you may want to try doing something more gentle at night and/or exercising earlier in the day.
Hunter Bennett, Lecturer in Exercise Science, University of South Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Artichoke vs Tomato – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing artichoke to tomato, we picked the artichoke.
Why?
Tomatoes are great, but artichokes are simply better in most ways:
In terms of macros, artichokes have more than 4x the fiber, more than 2x the carbs, and nearly 4x the protein, winning in this category.
In the category of vitamins, artichoke has more of vitamins B1, B2, B3, B5, B6, B7, B9, and K, while tomatoes have more of vitamins A, C, and E, giving artichokes an 8:3 win in this round.
Looking at minerals, artichoke has more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc, while tomatoes are not higher in any minerals; a complete win for artichoke here.
In other considerations, artichokes have more polyphenols, while tomatoes are a famously good source of lycopene, so we’ll call this round a tie.
Adding up the sections makes for a clear overall win for artichoke, but by all means enjoy either or both, as diversity is good!
Want to learn more?
You might like:
Lycopene’s Benefits For The Gut, Heart, Brain, & More
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:




