What Most People Don’t Know About HIV
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What To Know About HIV This World AIDS Day
Yesterday, we asked 10almonds readers to engage in a hypothetical thought experiment with us, and putting aside for a moment any reason you might feel the scenario wouldn’t apply for you, asked:
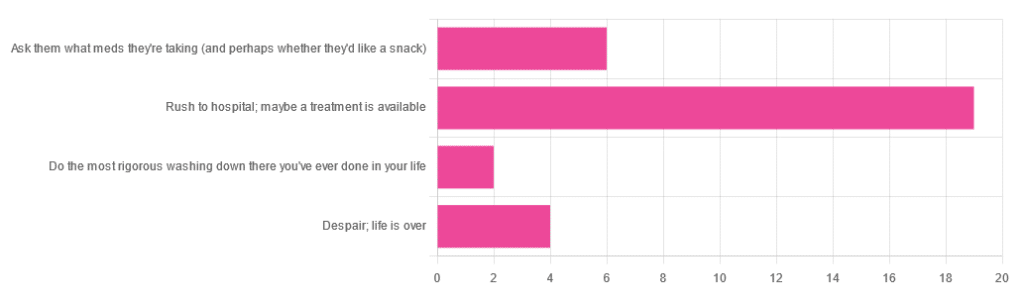
❝You have unprotected sex with someone who, afterwards, conversationally mentions their HIV+ status. Do you…❞
…and got the above-depicted, below-described, set of responses. Of those who responded…
- Just over 60% said “rush to hospital; maybe a treatment is available”
- Just under 20% said “ask them what meds they’re taking (and perhaps whether they’d like a snack)”
- Just over 10% said “despair; life is over”
- Two people said “do the most rigorous washing down there you’ve ever done in your life”
So, what does science say about it?
First, a quick note on terms
- HIV is the Human Immunodeficiency Virus. It does what it says on the tin; it gives humans immunodeficiency. Like many viruses that have become epidemic in humans, it started off in animals (called SIV, because there was no “H” involved yet), which were then eaten by humans, passing the virus to us when it one day mutated to allow that.
- It’s technically two viruses, but that’s beyond the scope of today’s article; for our purposes they are the same. HIV-1 is more virulent and infectious than HIV-2, and is the kind more commonly found in most of the world.
- AIDS is Acquired Immunodeficiency Syndrome, and again, is what it sounds like. When a person is infected with HIV, then without treatment, they will often develop AIDS.
- Technically AIDS itself doesn’t kill people; it just renders people near-defenseless to opportunistic infections (and immune-related diseases such as cancer), since one no longer has a properly working immune system. Common causes of death in AIDS patients include cancer, influenza, pneumonia, and tuberculosis.
People who contract HIV will usually develop AIDS if untreated. Untreated life expectancy is about 11 years.
HIV/AIDS are only a problem for gay people: True or False?
False, unequivocally. Anyone can get HIV and develop AIDS.
The reason it’s more associated with gay men, aside from homophobia, is that since penetrative sex is more likely to pass it on, then if we go with the statistically most likely arrangements here:
- If a man penetrates a woman and passes on HIV, that woman will probably not go on to penetrate someone else
- If a man penetrates a man and passes on HIV, that man could go on to penetrate someone else—and so on
- This means that without any difference in safety practices or promiscuity, it’s going to spread more between men on average, by simple mathematics.
- This is why “men who have sex with men” is the generally-designated higher-risk category.
There is medication to cure HIV/AIDS: True or False?
False so far (though there have been individual case studies of gene treatments that may have cured people—time will tell).
But! There are medications that can prevent HIV from being a life-threatening problem:
- PrEP (Pre-Exposure Prophylaxis) is a medication that one can take in advance of potential exposure to HIV, to guard against it.
- This is a common choice for people aren’t sure about their partners’ statuses, or people working in risky environments.
- PEP (Post-Exposure Prophylaxis) is a medication that one can take after potential exposure to HIV, to “nip it in the bud”.
- Those of you who were rushing to hospital in our poll, this is what you’re rushing there for.
- ARVs (Anti-RetroVirals) are a class of medications (there are different options; we don’t have room to distinguish them) that reduce an HIV+ person’s viral load to undetectable levels.
- Those of you who were asking what meds your partner was taking, these will be those meds. Also, most of them are to be taken in the morning with food, so that’s what the snack was for.
If someone is HIV+, the risk of transmission in unprotected sex is high: True or False?
True or False, with false being the far more likely. It depends on their medications, and this is why you were asking. If someone is on ARVs and their viral load is undetectable (as is usual once someone has been on ARVs for 6 months), they cannot transmit HIV to you.
U=U is not a fancy new emoticon, it means “undetectable = untransmittable”, which is a mathematically true statement in the case of HIV viral loads.
See: NIH | HIV Undetectable=Untransmittable (U=U)
If you’re thinking “still sounds risky to me”, then consider this:
You are safer having unprotected sex with someone who is HIV+ and on ARVs with an undetectable viral load, than you are with someone you are merely assuming is HIV- (perhaps you assume it because “surely this polite blushing young virgin of a straight man won’t give me cooties” etc)
Note that even your monogamous partner of many decades could accidentally contract HIV due to blood contamination in a hospital or an accident at work etc, so it’s good practice to also get tested after things that involve getting stabbed with needles, cut in a risky environment, etc.
If you’re concerned about potential stigma associated with HIV testing, you can get kits online:
CDC | How do I find an HIV self-test?
(these are usually fingerprick blood tests, and you can either see the results yourself at home immediately, or send it in for analysis, depending on the kit)
If I get HIV, I will get AIDS and die: True or False?
False, assuming you get treatment promptly and keep taking it. So those of you who were at “despair; life is over” can breathe a sigh of relief now.
However, if you get HIV, it does currently mean you will have to take those meds every day for the rest of your (no reason it shouldn’t be long and happy) life.
So, HIV is definitely still something to avoid, because it’s not great to have to take a life-saving medication every day. For a little insight as to what that might be like:
HIV.gov | Taking HIV Medication Every Day: Tips & Challenges
(as you’ll see there, there are also longer-lasting injections available instead of daily pulls, but those are much less widely available)
Summary
Some quick take-away notes-in-a-nutshell:
- Getting HIV may have been a death sentence in the 1980s, but nowadays it’s been relegated to the level of “serious inconvenience”.
- Happily, it is very preventable, with PrEP, PEP, and viral loads so low that they can’t transmit HIV, thanks to ARVs.
- Washing will not help, by the way. Safe sex will, though!
- As will celibacy and/or sexual exclusivity in seroconcordant relationships, e.g. you have the same (known! That means actually tested recently! Not just assumed!) HIV status as each other.
- If you do get it, it is very manageable with ARVs, but prevention is better than treatment
- There is no certain cure—yet. Some people (small number of case studies) may have been cured already with gene therapy, but we can’t know for sure yet.
Want to know more? Check out:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Sticky Jackfruit Burgers

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
All the taste and experience of pulled pork, without the increased risk of cancer and metabolic disease. On the contrary, jackfruit introduces lots of fiber, vitamins, carotenoids, and flavanones. We’ll have to do a main feature about jackfruit sometime; it’s an unusual fruit especially for its protein content, but for now, let’s get cooking!
You will need
- 1 can (14oz/400g) green jackfruit, drained (the flesh will not, in fact, be green—this is referring to the fruit being unripe and thus still firm in texture, which is what we want. The outside of the fruit, which will not be in the can, will have been green)
- 1/4 red cabbage, thinly sliced
- 1/2 carrot, grated
- 6 mangetout, thinly sliced
- 2 tbsp mayonnaise (your preference what kind, and yes, vegan is fine too)
- 1 tbsp extra virgin olive oil
- 1 tbsp gochujang paste (if you can’t find gochujang paste locally, you can either order it online (here it is on Amazon) or substitute with harissa paste, which is not the same—it uses different spices—but will do the same job here re texture, umami taste, and level of spiciness)
- 1 tbsp soy sauce
- 1 tbsp balsamic vinegar
- 1 tsp apple cider vinegar
- 1 tsp garlic paste
- 1 tsp tomato paste
- 1 tsp ginger paste
- 1 tsp chili flakes
- 3½ fl oz water
- 2 burger buns (unless you make them yourself, burger buns will probably not be healthy; you can, however, also look for small round wholemeal breads—the name of which varies far too much by region for us to try to get a catch-all name here—and use them in place of burger buns)
Method
(we suggest you read everything at least once before doing anything)
1) Combine the garlic paste, ginger paste, tomato paste, gochujang paste, soy sauce, balsamic vinegar, and chili flakes in a saucepan
2) Boil the 3½ fl oz water we mentioned; add it to the saucepan, mixing well, turn on the heat and let it simmer for 5 minutes or until it is thick and sticky (it will thicken more as it cools, too, so don’t worry if it doesn’t seem thick enough yet). Set it aside.
3) Dry the jackfruit (using strong kitchen paper should be fine), add the olive oil to a skillet and bring it to a high heat; add the jackfruit and fry on both sides for a few minutes, until it looks cooked (remember, while this may look like animal meat, it’s not, so there’s no danger of undercooking here).
4) When the jackfruit looks a nice golden-brown, add two thirds of the sauce from the saucepan, and break apart the jackfruit a bit (this can be done with a wooden/bamboo spatula, so as to not damage your pan), When it all looks how you’d expect pulled jackfruit (or pulled pork) to look, take it off the heat.
5) Combine the carrot, cabbage, and mangetout in a small bowl, adding the apple cider vinegar and mixing well; this will be the coleslaw element
6) Mix the remaining sauce with the mayonnaise
7) (optional) toast the burger buns
8) Assemble the burgers; we recommend the following order: bottom bun, pulled jackfruit, coleslaw, gochujang mayo, top bun

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Level-Up Your Fiber Intake, The Fun Way!
- 10 Ways To Balance Blood Sugars
- Our Top 5 Spices: How Much Is Enough For Benefits?
Take care!
Share This Post
-

Celery vs Rhubarb – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing celery to rhubarb, we picked the rhubarb.
Why?
In terms of macros, rhubarb has more carbs and fiber, the ratio of which give it the lower glycemic index, though both are low glycemic index foods. This means we’re calling this category a very marginal win for rhubarb, but a first-round win nevertheless!
In the category of vitamins, celery has more of vitamins A, B5, B6, and B9, while rhubarb has more vitamin C. A win for celery, this time.
Looking at minerals next, celery has more copper and phosphorus, while rhubarb has more calcium, iron, magnesium, manganese, potassium, and selenium. This one’s a clear win for rhubarb.
In other considerations, rhubarb has more polyphenols in not only in terms of overall quantity, but also in terms of “more useful to humans” too, being rich in an assortment of flavanols while celery must make do with some furanocoumarins (not in dangerous quantities, though).
Adding up the sections make for a clear overall win for rhubarb, but by all means do enjoy either or both, as diversity is best!
Want to learn more?
You might like to read:
Take care!
Share This Post
-

Bacopa Monnieri: A Well-Evidenced Cognitive Enhancer
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Bacopa monnieri: a powerful nootropic
Bacopa monnieri is one of those “from traditional use” herbs that has made its way into science.
It’s been used for at least 1,400 years in Ayurvedic medicine, for cognitive enhancement, against anxiety, and some disease-specific treatments.
See: Pharmacological attributes of Bacopa monnieri extract: current updates and clinical manifestation
What are its claimed health benefits?
Bacopa monnieri is these days mostly sold and bought as a nootropic, and that’s what the science supports best.
Nootropic benefits claimed:
- Improves attention, learning, and memory
- Reduces depression, anxiety, and stress
- Reduces restlessness and impulsivity
Other benefits claimed:
- Antioxidant properties
- Anti-inflammatory properties
- Anticancer properties
What does the science say?
Those last three, the antioxidant / anti-inflammatory / anticancer properties, when something has one of those qualities it often has all three, because there are overlapping systems at hand when it comes to oxidative stress, inflammation, and cellular damage.
Bacopa monnieri is no exception to this “rule of thumb”, and/but studies to support these benefits have mostly been animal studies and/or in vitro studies (i.e., cell cultures in a petri dish in lab conditions).
For example:
- Inhibition of lipoxygenases and cyclooxygenase-2 enzymes by extracts isolated from Bacopa monnieri
- Assessing the anti-inflammatory effects of Bacopa-derived bioactive compounds using network pharmacology and in vitro studies
- The evolving roles of Bacopa monnieri as potential anticancer agent: a review
In the category of antioxidant and anti-inflammatory effects in the brain, sometimes results differ depending on the test population, for example:
- Neuroprotective effects of Bacopa monnieri in experimental model of dementia (it worked for rats)
- Use of Bacopa monnieri in the treatment of dementia due to Alzheimer’s disease: systematic review of randomized controlled trials (it didn’t work for humans)
Anything more promising than that?
Yes! The nootropic effects have been much better-studied in humans, and with much better results.
For example, in this 12-week study in healthy adults, taking 300mg/day significantly improved visual information processing, learning, and memory (tested against placebo):
The chronic effects of an extract of Bacopa monnieri on cognitive function in healthy human subjects
Another 12-week study showed older adults enjoyed the same cognitive enhancement benefits as their younger peers:
Children taking 225mg/day, meanwhile, saw a significant reduction in ADHD symptoms, such as restlessness and impulsivity:
And as for the mood benefits, 300mg/day significantly reduced anxiety and depression in elderly adults:
In summary
Bacopa monnieri, taken at 300mg/day (studies ranged from 225mg/day to 600mg/day, but 300mg is most common) has well-evidenced cognitive benefits, including:
- Improved attention, learning, and memory
- Reduced depression, anxiety, and stress
- Reduced restlessness and impulsivity
It may also have other benefits, including against oxidative stress, inflammation, and cancer, but the research is thinner and/or not as conclusive for those.
Where to get it
As ever, we don’t sell it (or anything else), but for your convenience, here is an example product on Amazon.
Enjoy!
Share This Post


Related Posts
-
Elderberries vs Cranberries – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing elderberries to cranberries, we picked the elderberries.
Why?
In terms of macros, elderberry has slightly more carbs and 2x the fiber, the ratio of which gives elderberries the lower glycemic index also. A win for elderberries, then.
Looking at the vitamins, elderberries have more of vitamins A, B1, B2, B3, B6, B9, and C, while cranberries have more vitamin B5. An easy win for elderberries in this category.
In the category of minerals, we see a similar story: elderberries have more calcium, copper, iron, phosphorus, potassium, selenium, and zinc, while cranberries have (barely) more magnesium. Another clear win for elderberries.
Both of these fruits have additional “special” properties, and it’s worth noting that:
- elderberries’ bonus properties include that they significantly hasten recovery from upper respiratory tract viral infections.
- cranberries’ bonus properties (including: famously very good at reducing UTI risk) come with some warnings, including that they may increase the risk of kidney stones if you are prone to such, and also that cranberries have anti-clotting effects, which are great for heart health but can be a risk of you’re on blood thinners or have a bleeding disorder.
You can read about both of these fruits’ special properties in more detail below:
Want to learn more?
You might like to read:
- Herbs for Evidence-Based Health & Healing ← elderberry is in the list. We haven’t, at time of writing, done a main feature just on elderberry. Maybe soon!
- Health Benefits Of Cranberries (But: You’d Better Watch Out)
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Exercise That Protects Your Brain
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The Neuroscientist In The Gym

This is Dr. Wendy Suzuki. She’s a neuroscientist, and an expert in the neurobiology of memory, as well as neuroplasticity, and the role of exercise in neuroprotection.
We’ve sneakily semi-featured her before when we shared her Big Think talk:
Brain Benefits In Three Months… Through Walking?
Today we’re going to expand on that a little!
A Quick Recap
To share the absolute key points of that already fairly streamlined rundown:
- Exercise boosts levels of neurotransmitters such as dopamine and serotonin (and, which wasn’t mentioned there, noradrenaline)
- These are responsible for motivation, happiness, and focus (amongst other things)
- Persistent exercise boosts certain regions of the brain in particular, most notably the pre-frontal cortex and the hippocampi*
- These are responsible for planning and memory (amongst other things)
Dr. Suzuki advocates for stepping up your exercise routine if you can, with more exercise generally being better than less (unless you have some special medical reason why that’s not the case for you).
*often referred to in the singular as the hippocampus, but you have one on each side of your brain (unless a serious accident/incident destroyed one, but you’ll know if that applies to you, unless you lost both, in which case you will not remember about it).
What kind(s) of workout?
While a varied workout is best for overall health, for these brain benefits specifically, what’s most important is that it raises your heart rate.
This is why in her Big Think talk we shared before, she talks about the benefits of taking a brisk walk daily. See also:
If that’s not your thing, though (and/or is for whatever reason an inaccessible form of exercise for you), there is almost certainly some kind of High Intensity Interval Training that is a possibility for you. That might sound intimidating, but if you have a bit of floor and can exercise for one minute at a time, then HIIT is an option for you:
How To Do HIIT (Without Wrecking Your Body)
Dr. Suzuki herself is an ardent fan of “intenSati” which blends cardio workouts with yoga for holistic mind-and-body fitness. In fact, she loves it so much that she became a certified exercise instructor:
How much is enough?
It’s natural to want to know the minimum we can do to get results, but Dr. Suzuki would like us to bear in mind that when it comes to our time spent exercising, it’s not so much an expense of time as an investment in time:
❝Exercise is something that when you spend time on it, it will buy you time when you start to work❞
Read more: A Neuroscientist Experimented on Her Students and Found a Powerful Way to Improve Brain Function
Ok, but we really want to know how much!
Dr. Suzuki recommends at least three to four 30-minute exercise sessions per week.
Note: this adds up to less than the recommended 150 minutes of moderate exercise per week, but high-intensity exercise counts for twice the minutes for these purposes, e.g. 1 minute of high-intensity exercise is worth 2 minutes of moderate exercise.
How soon will we see benefits?
Benefits start immediately, but stack up cumulatively with continued long-term exercise:
❝My lab showed that a single workout can improve your ability to shift and focus attention, and that focus improvement will last for at least two hours. ❞
…which is a great start, but what’s more exciting is…
❝The more you’re working out, the bigger and stronger your hippocampus and prefrontal cortex gets. Why is that important?
Because the prefrontal cortex and the hippocampus are the two areas that are most susceptible to neurodegenerative diseases and normal cognitive decline in aging. ❞
In other words, while improving your heart rate through regular exercise will help prevent neurodegeneration by the usual mechanism of reducing neuroinflammation… It’ll also build the parts of your brain most susceptible to decline, meaning that when/if decline sets in, it’ll take a lot longer to get to a critical level of degradation, because it had more to start with.
Read more:
Inspir Modern Senior Living | Dr. Wendy Suzuki Boosts Brain Health with Exercise
Want more from Dr. Suzuki?
You might enjoy her TED talk:
Click Here If The Embedded Video Doesn’t Load Automatically
Prefer text? TED.com has a transcript for you
Prefer lots of text? You might like her book, which we haven’t reviewed yet but will soon:
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
- Exercise boosts levels of neurotransmitters such as dopamine and serotonin (and, which wasn’t mentioned there, noradrenaline)
-
What’s the best way to support autistic kids with mild to moderate delay?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Autistic children with mild to moderate developmental delay will no longer be eligible for the National Disability Insurance Scheme (NDIS) from mid-2027.
Instead, they will be directed to a new support system called Thriving Kids. This is yet to be fully designed, but it’s intended to prioritise children receiving support through mainstream community-based services.
Understandably, some parents and professionals are concerned, and many are asking whether the new program can match the support currently provided through the NDIS.
While time will reveal the impact of the policy, the more urgent task now is to define and deliver what best practice looks like for autistic children.
Start with terminology
With the announcement came some confusion about autism and developmental delay.
Disability and NDIS Minister Mark Butler referred to children with “mild to moderate autism” which is not actually a diagnosis, or a way we talk about autism in contemporary practice.
A clearer way would have been to refer to children with developmental delay as the target group for Thriving Kids, noting it will include many, but not all, autistic children.
The wording is important because, from a clinical perspective, autism is a lifelong neurodevelopmental condition that influences the way a person understands and interacts with other people and the world around them. Children don’t “grow out of autism”, but needs can fluctuate over time.
Developmental delay is a term used when a child is behind their peers in one or more aspects of development, such as motor skills, communication, or cognition.
Many autistic children have a developmental delay, but not all.
A three-year-old autistic child may have a mild developmental delay in motor skills that impacts their ability to climb at the playground. A five-year-old autistic child may have a moderate delay in language, which impacts their ability to understand and follow instructions in the classroom. But another autistic child may be at, or above, the age expected level for their developmental milestones.
Around 25% of autistic children have profound disability, meaning they require 24/7 supervision and support to be safe.
By seeing autism and developmental delay as separate, but related, we are better able to understand and meet the different needs of children “across the spectrum”.
So what does best practice look like for autistic children with mild to moderate developmental delay?
Best practice for autistic children
Australia’s national guideline sets out recommendations for supporting the learning, participation and wellbeing of autistic children and their families.
The guideline puts forward a principles-based approach that places children and families at the centre, and includes recommendations for goal-setting, selecting and delivering supports, monitoring outcomes and safeguarding.
The goals for supporting autistic children are no different from those for all children. They need love, opportunities to learn through everyday activities, and strong connections with family, culture and community.
The difference comes when children are struggling, and the question shifts to what additional supports will help. Keeping this broader understanding front of mind makes every other decision about extra support clearer and more consistent.
A stepped care approach
The guideline states support should be personalised for each child and family. There is no blanket approach to supporting autistic children that will be equally beneficial for each child and family.
At a system level, it means a stepped-care model of support in which the right type of support is delivered at the right time and in the right amount to match the child’s age, developmental level, strengths, needs and family circumstances. This is best practice internationally and something we should strive for.
Let’s say a parent takes their child to a routine visit with a maternal child health nurse or GP, and there are signs of developmental delay. Perhaps the child is behind in terms of motor skills and communication.
In a stepped-care model, the nurse or doctor can listen, ask questions, and understand any concerns the parents may have. If some additional support is needed, the “next step” depends on exactly what was learned.
For one parent, the “next step” might be some information and strategies to encourage their child’s development, for another it might be connection to a community playgroup, and for another a referral for some further assessment.
If difficulties emerge in childcare or school settings, the most effective approach is usually to strengthen the capability of educators to include and support children.
There may also be scope for targeted specialist input, such as speech pathology, physiotherapy, or psychology, when needed.
The point is that the “steps” match the needs, and will be different for each child and family.
As professionals, we can support parents to make decisions by encouraging them to ask: “is this the best next step for my child and family?” This approach helps prevent the over-servicing that can happen when families are directed straight to the highest level of support.
What should happen next?
The new Thriving Kids program represents a genuine opportunity to transform how Australia supports children with mild to moderate developmental delays, including many autistic children.
Done well, it could become the stepped-care model of support that families desperately need. Get it wrong, and it becomes another well-intentioned policy that fails the children it’s meant to help.
Stepped-care models require deliberate design, sustained investment and careful attention to implementation details.
The key to getting this right lies in genuine co-design with the people who matter most: children and families themselves. They understand what works and what doesn’t, and where the gaps are.
David Trembath, Head of Autism Research and Senior Principal Research Fellow, The Kids Research Institute Australia; Andrew Whitehouse, Deputy Director, the Kids Research Institute Australia, The University of Western Australia, and Kandice Varcin, Senior Research Fellow in autism research, The Kids Research Institute Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: