Habits of a Happy Brain – by Dr. Loretta Graziano Breuning
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There are lots of books on “happy chemicals” and “how to retrain your brain”, so what makes this one different?
Firstly, it focuses on four “happy chemicals”, not just one:
- Serotonin
- Dopamine
- Oxytocin
- Endorphins
It also looks at the role of cortisol, and how it caps off each of those just a little bit, to keep us just a little malcontent.
Behavioral psychology tends to focus most on dopamine, while prescription pharmaceuticals for happiness (i.e., most antidepressants) tend to focus on serotonin. Here, Dr. Breuning helps us understand the complex interplay of all of the aforementioned chemicals.
She also clears up many misconceptions, since a lot of people misattribute the functions of each of these.
Common examples include “I’m doing this for the serotonin!” when the activity is dopaminergic not serotoninergic, or considering dopamine “the love molecule” when oxytocin, or even something else like phenylethylamine would be more appropriate.
The above may seem like academic quibbles and not something of practical use, but if we want to biohack our brains, we need to do better than the equivalent of a chef who doesn’t know the difference between salt and sugar.
Where things are of less practical use, she tends to skip over or at least streamline them. For example, she doesn’t really discuss the role of post-dopamine prolactin in men—but the discussion of post-happiness cortisol covers the same ground anyway, for practical purposes.
Dr. Breuning also looks at where our evolved neurochemical responses go wrong, and lays out guidelines for such challenges as overcoming addiction, or embracing delayed gratification.
Bottom line: this book is a great user-manual for the brain. If you’d like to be happier and more effective with fewer bad habits, this is the book for you.
Click here to check out Habits of a Happy Brain, and get biohacking yours!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Ketogenic Diet: Burning Fat Or Burning Out?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.

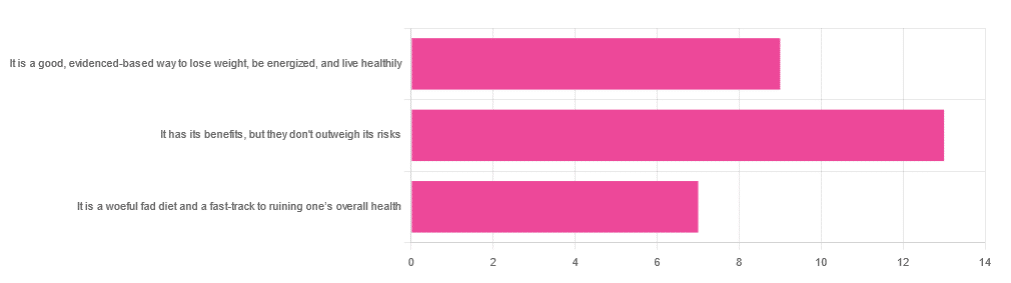
In Wednesday’s newsletter, we asked you for your opinion of the keto diet, and got the above-depicted, below-described set of responses:
- About 45% said “It has its benefits, but they don’t outweigh the risks”
- About 31% said “It is a good, evidence-based way to lose weight, be energized, and live healthily”
- About 24% said “It is a woeful fad diet and a fast-track to ruining one’s overall health”
So what does the science say?
First, what is the ketogenic diet?
There are two different stories here:
- Per science, it’s a medical diet designed to help treat refractory epilepsy in children.
- Per popular lore, it’s an energizing weight loss diet for Instagrammers and YouTubers.
Can it be both? The answer is: yes, but with some serious caveats, which we’ll cover over the course of today’s feature.
The ketogenic diet works by forcing the body to burn fat for energy: True or False?
True! This is why it helps for children with refractory epilepsy. By starving the body (including the brain) of glucose, the liver must convert fat into fatty acids and ketones, which latter the brain (and indeed the rest of the body) can now use for energy instead of glucose, thus avoiding one of the the main triggers of refractory epilepsy in children.
See: The Ketogenic Diet: One Decade Later | Pediatrics
Even the pediatric epilepsy studies, however, conclude it does have unwanted side effects, such as kidney stones, constipation, high cholesterol, and acidosis:
Source: Dietary Therapies for Epilepsy
The ketogenic diet is good for weight loss: True or False?
True! Insofar as it does cause weight loss, often rapidly. Of course, so do diarrhea and vomiting, but these are not usually held to be healthy methods of weight loss. As for keto, a team of researchers recently concluded:
❝As obesity rates in the populace keep rising, dietary fads such as the ketogenic diet are gaining traction.
Although they could help with weight loss, this study had a notable observation of severe hypercholesterolemia and increased risk of atherosclerotic cardiovascular disease among the ketogenic diet participants.❞
~ Dr. Shadan Khdher et al.
On which note…
The ketogenic diet is bad for the heart: True or False?
True! As Dr. Joanna Popiolek-Kalisz concluded recently:
❝In terms of cardiovascular mortality, the low-carb pattern is more beneficial than very low-carbohydrate (including the ketogenic diet). There is still scarce evidence comparing ketogenic to the Mediterranean diet.
Other safety concerns in cardiovascular patients such as adverse events related to ketosis, fat-free mass loss, or potential pharmacological interactions should be also taken into consideration in future research.❞
~ Dr. Joanna Popiolek-Kalisz
Read in full: Ketogenic diet and cardiovascular risk: state of the art review
The ketogenic diet is good for short-term weight loss, but not long-term maintenance: True or False?
True! Again, insofar as it works in the short term. It’s not the healthiest way to lose weight and we don’t recommend it, but it did does indeed precipitate short-term weight loss. Those benefits are not typically observed for longer than a short time, though, as the above-linked paper mentions:
❝The ketogenic diet does not fulfill the criteria of a healthy diet. It presents the potential for rapid short-term reduction of body mass, triglycerides level, Hb1Ac, and blood pressure.
Its efficacy for weight loss and the above-mentioned metabolic changes is not significant in long-term observations.❞
~ Ibid.
The ketogenic diet is a good, evidence-based way to lose weight, be energized, and live healthily: True or False?
False, simply, as you may have gathered from the above, but we’ve barely scratched the surface in terms of the risks.
That said, as mentioned, it will induce short-term weight loss, and as for being energized, typically there is a slump-spike-slump in energy:
- At first, the body is running out of glucose, and so naturally feels weak and tired.
- Next, the body enters ketosis, and so feels energized and enlivened ← this is the part where the popular enthusiastic reviews come from
- Then, the body starts experiencing all the longer-term problems associated with lacking carbohydrates and having an overabundance of fat, so becomes gradually more sick and tired.
Because of this, the signs of symptoms of being in ketosis (aside from: measurably increased ketones in blood, breath, and urine) are listed as:
- Bad breath
- Weight loss
- Appetite loss
- Increased focus and energy
- Increased fatigue and irritability
- Digestive issues
- Insomnia
The slump-spike-slump we mentioned is the reason for the seemingly contradictory symptoms of increased energy and increased fatigue—you get one and then the other.
Here’s a small but illustrative study, made clearer by its participants being a demographic whose energy levels are most strongly affected by dietary factors:
The ketogenic diet is a woeful fad diet and a fast-track to ruining one’s overall health: True or False?
True, subjectively in the first part, as it’s a little harsher than we usually go for in tone, though it has been called a fad diet in scientific literature. The latter part (ruining one’s overall health) is observably true.
One major problem is incidental-but-serious, which is that a low-carb diet is typically a de facto low-fiber diet, which is naturally bad for the gut and heart.
Other things are more specific to the keto diet, such as the problems with the kidneys:
However, kidney stones aren’t the worst of the problems:
Is Losing Weight Worth Losing Your Kidney: Keto Diet Resulting in Renal Failure
We’re running out of space and the risks associated with the keto diet are many, but for example even in the short term, it already increases osteoporosis risk:
❝Markers of bone modeling/remodeling were impaired after short-term low-carbohydrate high-fat diet, and only one marker of resorption recovered after acute carbohydrate restoration❞
~ Dr. Ida Heikura et al.
A Short-Term Ketogenic Diet Impairs Markers of Bone Health in Response to Exercise
Want a healthier diet?
We recommend the Mediterranean diet.
See also: Four Ways To Upgrade The Mediterranean
(the above is about keeping to the Mediterranean diet, while tweaking one’s choices within it for a specific extra health focus such as an anti-inflammatory upgrade, a heart-healthy upgrade, a gut-healthy upgrade, and a brain-healthy upgrade)
Enjoy!
Share This Post
-

PS, We Love You
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
PS, we love you. With good reason!
There are nearly 20,000 studies on PS listed on PubMed alone, and its established benefits include:
- significantly improving memory
- potential reversal (!) of neurodegeneration
- reduction of stress activation
- improvement in exercise capacity
- it even helps avoid rejection of medical implants
We’ll explore some of these studies and give an overview of how PS does what it does. Just like the (otherwise unrelated) l-theanine we talked about a couple of weeks ago, it does do a lot of things.
PS = Cow Brain?!
Let’s first address a concern. You may have heard something along the lines of “hey, isn’t PS made from cow brain, and isn’t that Very Bad™ for humans, mad cow disease and all?”. The short answer is:
Firstly: ingesting cow brain tissue is indeed generally considered Very Bad™ for humans, on account of the potential for transmission of Bovine Spongiform Encephalopathy (BSE) resulting in its human equivalent, Creutzfeldt–Jakob Disease (CJD), whose unpleasantries are beyond the scope of this newsletter.
Secondly (and more pleasantly): whilst PS can be derived from bovine brain tissue, most PS supplements these days derive from soy—or sometimes sunflower lecithin. Check labels if unsure.
Using PS to Improve Other Treatments
In the human body, the question of tolerance brings us a paradox (not the tolerance paradox, important as that may also be): we must build and maintain a strong immune system capable of quickly adapting to new things, and then when we need medicines (or even supplements), we need our body to not build tolerance of them, for them to continue having an effect.
So, we’re going to look at a very hot-off-the-press study (Feb 2023), that found PS to “mediate oral tolerance”, which means that it helps things (medications, supplements etc.) that we take orally and want to keep working, keep working.
In the scientists’ own words (we love scientists’ own words because they haven’t been distorted by the popular press)…
❝This immunotherapy has been shown to prevent/reduce immune response against life-saving protein-based therapies, food allergens, autoantigens, and the antigenic viral capsid peptide commonly used in gene therapy, suggesting a broad spectrum of potential clinical applications. Given the good safety profile of PS together with the ease of administration, oral tolerance achieved with PS-based nanoparticles has a very promising therapeutic impact.❞
Nguyen et al, Feb 2023
In other words, to parse those two very long sentences into two shorter bullet points:
- It allows a lot of important treatments to continue working—treatments that the body would otherwise counteract
- It is very safe—and won’t harm the normal function of your immune system at large
This is also very consistent with one of the benefits we mentioned up top—PS helps avoid rejection of implants, something that can be a huge difference to health-related quality of life (HRQoL), never mind sometimes life itself!
What is PS Anyways, and How Does It Work?
Phosphatidylserine is a phospholipid, a kind of lipid, found in cell membranes. More importantly:
It’s a signalling agent, mainly for apoptosis, which in lay terms means: it tells cells when it’s time to die.
Cellular death sounds like a bad thing, but prompt and efficient cellular apoptosis (death) and resultant prompt and efficient autophagy (recycling) reduce the risk of your body making mistakes when creating new cells from old cells.
Think about photocopying:
- Situation A: You have a document, and you want to copy it. If you copy it before it gets messed up, your copy will look almost, if not exactly, like the original. It’ll be super easy to read.
- Situation B: You have a document, and you want to copy it, but you delay doing so for so long that the original is all scuffed and creased and has a coffee stain on it. These unwanted changes will get copied onto the new document, and any copy made of that copy will keep the problems too. It gets worse and worse each time.
So, using this over-simplifier analogy, the speed of ‘copying’ is a major factor in cellular aging. The sooner cells are copied, before something gets damaged, the better the copy will be.
So you really, really want to have enough PS (our bodies make it too, by the way) to signal promptly to a cell when its time is up.
You do not want cells soldiering on until they’re the biological equivalent of that crumpled up, coffee-stained sheet of paper.
Little wonder, then, that PS’ most commonly-sought benefit when it comes to supplementation is to help avoid age-related neurodegeneration (most notably, memory loss)!
Keeping the cells young means keeping the brain young!
PS’s role as a signalling agent doesn’t end there—it also has a lot to say to a wide variety of the body’s immunological cells, helping them know what needs to happen to what. Some things should be immediately eaten and recycled; other things need more extreme measures applied to them first, and yet other things need to be ignored, and so forth.
You can read more about that in Elsevier’s publication if you’re curious 🙂
Wow, what a ride today’s newsletter has been! We started at paracetamoxyfrusebendroneomycin, and got down to the nitty gritty with a bunch of hopefully digestible science!
We love feedback, so please let us know if we’re striking the balance right, and/or if you’d like to see more or less of something—there’s a feedback widget at the bottom of this email!
Share This Post
-

Rise And (Really) Shine!
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Q&A with 10almonds Subscribers!
Q: Would love to hear more ideas about effective first thing in the morning time management to get a great start on your day.
A: There are a lot of schools of thought about what’s best in this regard! Maybe we’ll do a main feature sometime. But some things that are almost universally agreed upon are:
- Prepare your to-do list the night before
- Have some sort of buffer between waking up and getting to productivity.
- For me (hi, your writer here) it’s my first coffee of the day. It’s not even about the caffeine, it’s about the ritual of it, it’s a marker that separates my night from the day and tells my brain what gear to get into.
- Others may like to exercise first thing in the morning
- For still yet others, it could be a shower, cold or otherwise
- Some people like a tall glass of lemon water to rehydrate after sleeping!
- If you take drinkable morning supplements such as this pretty awesome nootropic stack, it’s a great time for that and an excellent way to get the brain-juices flowing!
- When you do get to productivity: eat the frog first! What this means is: if eating a frog is the hardest thing you’ll have to do all day, do that first. Basically, tackle the most intimidating task first. That way, you won’t spend your day stressed/anxious and/or subconsciously wasting time in order to procrastinate and avoid it.
- Counterpart to the above: a great idea is to also plan something to look forward to when your working day is done. It doesn’t matter much what it is, provided it’s rewarding to you, that makes you keen to finish your tasks to get to it.
Have a question you’d like to see answered here? Hit reply to this email, or use the feedback widget at the bottom! We always love to hear from you
Share This Post

Related Posts
-

Blind Spots – by Dr. Marty Makary
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
From the time the US recommended not giving peanuts to infants for the first three years of life “in order to avoid peanut allergies” (whereupon non-exposure to peanuts early in life led to, instead, an increase in peanut allergies and anaphylactic incidents), to the time the US recommended not taking HRT on the strength of the claim that “HRT causes breast cancer” (whereupon the reduced popularity of HRT led to, instead, an increase in breast cancer incidence and mortality), to many other such incidents of very bad public advice being given on the strength of a single badly-misrepresented study (for each respective thing), Dr. Makary puts the spotlight on what went wrong.
This is important, because this is not just a book of outrage, exclaiming “how could this happen?!”, but rather instead, is a book of inquisition, asking “how did this happen?”, in such a way that we the reader can spot similar patterns going forwards.
Oftentimes, this is a simple matter of having a basic understanding of statistics, and checking sources to see if the dataset really supports what the headlines are claiming—and indeed, whether sometimes it suggests rather the opposite.
The style is a little on the sensationalist side, but it’s well-supported with sound arguments, good science, and clear mathematics.
Bottom line: if you’d like to improve your scientific literacy, this book is an excellent illustrative guide.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Red Bell Peppers vs Tomatoes – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing red bell peppers to tomatoes, we picked the peppers.
Why?
In terms of macronutrients, these two fruits-that-get-used-as-vegetables are similar in most respects; they’re mostly water, negligible protein and fat, similar amounts of carbs, even a similar carb breakdown (mostly fructose and glucose). One thing that does set them apart is that peppers* have about 2x the fiber, which difference results in peppers having the lower Glycemic Index—though tomatoes are quite low in GI too.
*for brevity we’re just going to write “peppers”, but we are still talking about sweet red bell peppers throughout. This is important, as different color peppers have different nutrient profiles.
In the category of vitamins, peppers have much more of vitamins A, B1, B2, B3, B5, B6, B9, C, and E. In contrast, tomatoes have more vitamin K. An easy win for peppers.
When it comes to minerals, the margins are narrower, but peppers have more iron, zinc, and selenium, while tomatoes have more calcium and copper. They’re approximately equal on other minerals they both contain, making this category a slight (3:2) win for peppers.
As for phytochemical benefits, both are good sources of lycopene (both better when cooked) and other carotenes (for example lutein), and both have an array of assorted flavonoids.
All in all, a win for peppers, but both are great!
Want to learn more?
You might like to read:
- Brain Food? The Eyes Have It!
- Bell Peppers: A Spectrum Of Specialties
- Lycopene’s Benefits For The Gut, Heart, Brain, & More
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Spirulina vs Nori – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing spirulina to nori, we picked the nori.
Why?
In the battle of the seaweeds, if spirulina is a superfood (and it is), then nori is a super-dooperfood. So today is one of those “a very nutritious food making another very nutritious food look bad by standing next to it” days. With that in mind…
In terms of macros, they’re close to identical. They’re both mostly water with protein, carbs, and fiber. Technically nori is higher in carbs, but we’re talking about 2.5g/100g difference.
In the category of vitamins, spirulina has more vitamin B1, while nori has a lot more of vitamins A, B2, B3, B5, B6, B9, C, E, K, and choline.
When it comes to minerals, it’s a little closer but still a clear win for nori; spirulina has more copper, iron, and magnesium, while nori has more calcium, manganese, phosphorus, potassium, and zinc.
Want to try some nori? Here’s an example product on Amazon 😎
Want to learn more?
You might like to read:
21% Stronger Bones in a Year at 62? Yes, It’s Possible (No Calcium Supplements Needed!) ← nori was an important part of the diet enjoyed here
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: