Genetic Risk Factors For Long COVID
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Some people, after getting COVID, go on to have Long COVID. There are various contributing factors to this, including:
- Lifestyle factors that impact general disease-proneness
- Immune-specific factors such as being immunocompromised already
- Genetic factors
We looked at some modifiable factors to improve one’s disease-resistance, yesterday:
And we’ve taken a more big-picture look previously:
Beyond Supplements: The Real Immune-Boosters!
Along with some more systemic issues:
Why Some People Get Sick More (And How To Not Be One Of Them)
But, for when the “don’t get COVID” ship has sailed, one of the big remaining deciding factors with regard to whether one gets Long COVID or not, is genetic
The Long COVID Genes
For those with their 23andMe genetic data to hand…
❝Study findings revealed that three specific genetic loci, HLA-DQA1–HLA-DQB1, ABO, and BPTF–KPAN2–C17orf58, and three phenotypes were at significantly heightened risk, highlighting high-priority populations for interventions against this poorly understood disease.❞
For those who don’t, then first: you might consider getting that! Here’s why:
Genetic Testing: Health Benefits & Methods
But also, all is not lost meanwhile:
The same study also found that individuals with genetic predispositions to chronic fatigue, depression, and fibromyalgia, as well as other phenotypes such as autoimmune conditions and cardiometabolic conditions, are at significantly higher risk of long-COVID than individuals without these conditions.
Good news, bad news
Another finding was that women and non-smokers were more likely to get Long COVID, than men and smokers, respectively.
Does that mean that those things are protective against Long COVID, which would be very counterintuitive in the case of smoking?
Well, yes and no; it depends on whether you count “less likely to get Long COVID because of being more likely to just die” as protective against Long COVID.
(Incidentally, estrogen is moderately immune-enhancing, while testosterone is moderately immune-suppressing, so the sex thing was not too surprising. It’s also at least contributory to why women get more autoimmune disorders, while men get more respiratory infections such as colds and the like)
Want to know more?
You can read the paper itself, here:
*GWAS = Genome-Wide Association Study
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Mini Cuts: How To Lose Fat Quickly & Safely

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
No, one cannot healthily do this long-term. But for a few weeks to quickly drop fat while preserving lean muscle, yes:
Briefly does it
Step by step, the process goes like this:
- prep before starting: eat at maintenance for 1–2 weeks; set a clear goal (perhaps you have a vacation or event in mind that you want to look a certain way for).
- set calorie target: calculate maintenance calories; and subtract 300–500 for your mini cut. If unsure, use goal bodyweight in pounds ×10.
- set macro ratios: week 1 use 45% protein, 25% carbs, 30% fat; week 2 use 50% protein, 30% carbs, 20% fat; track as accurately as you reasonably can.
- plan and prep meals: batch-prep simple, repetitive meals (this makes tracking easier), with a focus on lean proteins, vegetables, fruits, and other high-volume foods to improve satiety.
- training adjustments: keep your strength training consistent; consider a small carb snack pre-workout if you usually train fasted, and avoid excessive cardio.
- remember to end the mini cut: per the first step, the duration should be 7–14 days (absolute maximum 30).
- reverse out: increase calories gradually by around 100 kcal per day until it’s back to the maintenance levels; you can reduce protein to 30–40% as carbs and fats normalize. then stay at maintenance for at least another 1–2 weeks before considering another deficit phase if you still want to lose more fat.
- reflect and reset: assess your results (body composition, energy, performance); treat mini cuts as a tool, not a lifestyle; returning to balanced eating is important for sustainability and general health.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
How To Lose Weight (Healthily!) ← for a more sustainable approach; honestly we recommend this much more
Take care!
Share This Post
-
Singledom & Healthy Longevity
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Statistically, those who live longest, do so in happy, fulfilling, committed relationships.
Note: happy, fulfilling, committed relationships. Less than that won’t do. Your insurance company might care about your marital status for its own sake, but your actual health doesn’t—it’s about the emotional safety and security that a good, healthy, happy, fulfilling relationship offers.
We wrote about this here:
Only One Kind Of Relationship Promotes Longevity This Much!
But that’s not the full story
For a start, while being in a happy fulfilling committed relationship statistically adds healthy life years, being in a relationship that falls short of those adjectives certainly does not. See also:
Relationships: When To Stick It Out & When To Call It Quits
But also, life satisfaction steadily improves with age, for single people (the results are more complicated for partnered people—probably because of the range of difference in quality of relationships). At least, this held true in this large (n=6,188) study of people aged 40–85 years:
❝With advancing age, partnership status became less predictive of loneliness and the satisfaction with being single increased. Among later-born cohorts, the association between partnership status and loneliness was less strong than among earlier-born cohorts. Later-born single people were more satisfied with being single than their earlier-born counterparts.❞
Note that this does mean that while life satisfaction indeed improves with age for single people, that’s a generalized trend, and the greatest life satisfaction within this set of singles comes hand-in-hand with being single by choice rather than by perceived obligation, i.e., those who are “single and not looking” will generally be the most content, and this contentedness will improve with age, but for those who are “single and looking”, in that case it’s the younger people who have it better, likely due to a greater sense of having plenty of time.
For that matter, gender plays a role; this large survey of singles found that (despite the popular old pop-up ads advising that “older women in your area are looking to date”), in reality older single women were the least likely to actively look for a partner:
See: A Profile Of Single Americans
…which also shows that about half of single Americans are “not looking”, and of those who are, about half are open to a serious relationship, though this is more common under the age of 40, while being over the age of 40 sees more people looking only for something casual.
Take-away from this section: being single only decreases life satisfaction if one doesn’t enjoy being single, and even then, and increases it if one does enjoy being single.
But that’s about life satisfaction, not longevity
We found no studies specifically into longevity of singledom, only the implications that may be drawn from the longevity of partnered people.
However, there is a lot of research that shows it’s not being single that kills, it’s being socially isolated. It’s a function of neurodegeneration from a lack of conversation, and it’s a function of what happens when someone slips in the shower and is found a week later. Things like that.
For example: Is Living Alone “Aging Alone”? Solitary Living, Network Types, and Well-Being
What if you are alone and don’t want to be?
We’ve not, at time of writing, written dating advice in our Psychology Sunday section, but this writer’s advice is: don’t even try.
That’s not nihilism or even cynicism, by the way; it’s actually a kind of optimism. The trick is just to let them come to you.
(sample size of one here, but this writer has never looked for a relationship in her life, they’ve always just found me, and now that I’m widowed and intend to remain single, I still get offers—and no, I’m not a supermodel, nor rich, nor anything like that)
Simply: instead of trying to find a partner, just work on expanding your social relationships in general (which is much easier, because the process is something you can control, whereas the outcome of trying to find a suitable partner is not), and if someone who’s right for you comes along, great! If not, then well, at least you have a flock of friends now, and who knows what new unexpected romance may lie around the corner.
As for how to do that,
How To Beat Loneliness & Isolation
Take care!
Share This Post
-
Neurologists Debunk 11 Brain Myths
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Neuroscientists Dr. Santoshi Billakota and Dr. Brad Kamitaki debunk 11 myths about the brain. How many did you know?
From the top
Without further ado, the myths are…
- “We only use 10% of our brains”: False! We use most parts of our brain at different times, depending on the activity. PET/MRI scans show widespread usage.
- “The bigger the brain, the smarter the creature”: False! While there’s often a correlation, intelligence depends on brain complexity and development of specific regions, not overall size. For this reason get, for example, some corvids that are more intelligent than some dogs.
- “IQ tests are an accurate measure of intelligence”: False! IQ tests measure limited aspects of intelligence and are influenced by external factors like test conditions and education.
- “Video games rot your brain”: False! Video games can improve problem-solving, strategy, and team-building skills when played in moderation.
- “Memory gets worse as you age”: Partly false. While episodic memory may decline, semantic and procedural memory often improve with age.
- “Left-brained people are logical, and right-brained people are creative”: False! Both hemispheres work together, and personality or skills are influenced by environment and experiences, not brain hemispheres.
- “You can’t prevent a stroke”: False! Strokes can often be prevented by managing risk factors like blood pressure, cholesterol, and lifestyle choices.
- “Eating fish makes you smarter”: False! Eating fish, especially those rich in omega-3s, can support brain health but won’t increase intelligence.
- “You can always trust your senses”: False! Senses can be deceptive and influenced by emotions, memories, or neurological conditions.
- “Different sexes have different brains”: False! Structurally, brains are the same regardless of chromosomal sex; differences arise from environmental (including hormonal) and experiential factors—and even there, there’s more than enough overlap that we are far from categorizable as sexually dimorphic.
- “If you have a seizure, you have epilepsy”: False! A seizure can occur from various causes, but epilepsy is defined by recurrent unprovoked seizures and requires specific diagnosis and treatment.
For more on all of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
The Dopamine Myth ← a bonus 12th myth!
Take care!
Share This Post

-

This salt alternative could help reduce blood pressure. So why are so few people using it?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
One in three Australian adults has high blood pressure (hypertension). Excess salt (sodium) increases the risk of high blood pressure so everyone with hypertension is advised to reduce salt in their diet.
But despite decades of strong recommendations we have failed to get Australians to cut their intake. It’s hard for people to change the way they cook, season their food differently, pick low-salt foods off the supermarket shelves and accept a less salty taste.
Now there is a simple and effective solution: potassium-enriched salt. It can be used just like regular salt and most people don’t notice any important difference in taste.
Switching to potassium-enriched salt is feasible in a way that cutting salt intake is not. Our new research concludes clinical guidelines for hypertension should give patients clear recommendations to switch.
What is potassium-enriched salt?
Potassium-enriched salts replace some of the sodium chloride that makes up regular salt with potassium chloride. They’re also called low-sodium salt, potassium salt, heart salt, mineral salt, or sodium-reduced salt.
Potassium chloride looks the same as sodium chloride and tastes very similar.
Potassium-enriched salt works to lower blood pressure not only because it reduces sodium intake but also because it increases potassium intake. Insufficient potassium, which mostly comes from fruit and vegetables, is another big cause of high blood pressure.
What is the evidence?
We have strong evidence from a randomised trial of 20,995 people that switching to potassium-enriched salt lowers blood pressure and reduces the risks of stroke, heart attacks and early death. The participants had a history of stroke or were 60 years of age or older and had high blood pressure.
An overview of 21 other studies suggests much of the world’s population could benefit from potassium-enriched salt.
The World Health Organisation’s 2023 global report on hypertension highlighted potassium-enriched salt as an “affordable strategy” to reduce blood pressure and prevent cardiovascular events such as strokes.
What should clinical guidelines say?
We teamed up with researchers from the United States, Australia, Japan, South Africa and India to review 32 clinical guidelines for managing high blood pressure across the world. Our findings are published today in the American Heart Association’s journal, Hypertension.
We found current guidelines don’t give clear and consistent advice on using potassium-enriched salt.
While many guidelines recommend increasing dietary potassium intake, and all refer to reducing sodium intake, only two guidelines – the Chinese and European – recommend using potassium-enriched salt.
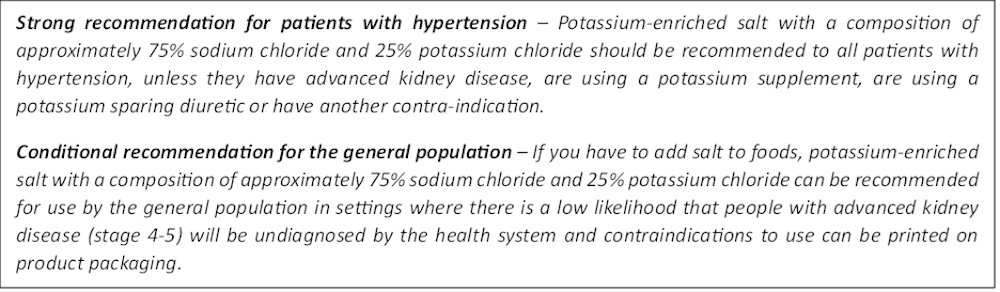
To help guidelines reflect the latest evidence, we suggested specific wording which could be adopted in Australia and around the world:

Recommended wording for guidance about the use of potassium-enriched salt in clinical management guidelines. Why do so few people use it?
Most people are unaware of how much salt they eat or the health issues it can cause. Few people know a simple switch to potassium-enriched salt can help lower blood pressure and reduce the risk of a stroke and heart disease.
Limited availability is another challenge. Several Australian retailers stock potassium-enriched salt but there is usually only one brand available, and it is often on the bottom shelf or in a special food aisle.
Potassium-enriched salts also cost more than regular salt, though it’s still low cost compared to most other foods, and not as expensive as many fancy salts now available.
It looks and tastes like normal salt.
Jimmy Dean/UnsplashA 2021 review found potassium-enriched salts were marketed in only 47 countries and those were mostly high-income countries. Prices ranged from the same as regular salt to almost 15 times greater.
Even though generally more expensive, potassium-enriched salt has the potential to be highly cost effective for disease prevention.
Preventing harm
A frequently raised concern about using potassium-enriched salt is the risk of high blood potassium levels (hyperkalemia) in the approximately 2% of the population with serious kidney disease.
People with serious kidney disease are already advised to avoid regular salt and to avoid foods high in potassium.
No harm from potassium-enriched salt has been recorded in any trial done to date, but all studies were done in a clinical setting with specific guidance for people with kidney disease.
Our current priority is to get people being managed for hypertension to use potassium-enriched salt because health-care providers can advise against its use in people at risk of hyperkalemia.
In some countries, potassium-enriched salt is recommended to the entire community because the potential benefits are so large. A modelling study showed almost half a million strokes and heart attacks would be averted every year in China if the population switched to potassium-enriched salt.
What will happen next?
In 2022, the health minister launched the National Hypertension Taskforce, which aims to improve blood pressure control rates from 32% to 70% by 2030 in Australia.
Potassium-enriched salt can play a key role in achieving this. We are working with the taskforce to update Australian hypertension management guidelines, and to promote the new guidelines to health professionals.
In parallel, we need potassium-enriched salt to be more accessible. We are engaging stakeholders to increase the availability of these products nationwide.
The world has already changed its salt supply once: from regular salt to iodised salt. Iodisation efforts began in the 1920s and took the best part of 100 years to achieve traction. Salt iodisation is a key public health achievement of the last century preventing goitre (a condition where your thyroid gland grows larger) and enhancing educational outcomes for millions of the poorest children in the world, as iodine is essential for normal growth and brain development.
The next switch to iodised and potassium-enriched salt offers at least the same potential for global health gains. But we need to make it happen in a fraction of the time.

Xiaoyue Xu (Luna), Scientia Lecturer, UNSW Sydney; Alta Schutte, SHARP Professor of Cardiovascular Medicine, UNSW Sydney, and Bruce Neal, Executive Director, George Institute Australia, George Institute for Global Health
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
The Exercise That Protects Older Adults From Cancer
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The relationship between exercise and cancer has sometimes been laden with confusion, and in particular, it was long popularly believed that exercise accelerates cancer once it occurs, but now it seems that’s not the case.
You might have read about that, and specifically about how a research team (Dr. Alice Avancini et al.) analysed data from 22 randomized controlled trials (total n=968 participants) that investigated the effects of exercise on various pro-inflammatory biomarkers (mostly interleukin variants, but also c-reactive proteins) that are known to increase breast cancer reoccurrence risk.
What they found was:
❝Exercise induced small to large significant reductions in IL-6 (SMD = -0.85; 95% CI = -1.68 to -0.02; p = .05) and TNF-α (SMD = -0.40; 95% CI = -0.81 to 0.01; p = .05) and a trend for a decrease in CRP.
When stratifying by exercise mode, trends toward reduction in IL-6 and TNF-α were observed for combined exercise, whilst changes were not generally affected by exercise program duration❞
The “combined exercise” mentioned?
Aerobic exercise and resistance training.
This is important, because as regular 10almonds readers may remember…
What Your Metabolism Says About How Aggressive Cancer Is Likely To Be For You ← this makes a huge difference to survival chances
So, this study’s findings are very consistent with that, because:
- Aerobic training increases cardiovascular fitness, improving metabolism
- Resistance training increases muscle mass, improving metabolism*
*because muscle “costs” calories to maintain, prompting an increase in metabolism, whereas fat prompts our metabolism to slow, to conserve energy to face the obvious food shortage that must be coming
See also: Stop Cancer 20 Years Ago
Exercise & aging muscle
Yes, we said “older adults” specifically in the title, and now we’re getting to that part!
Most recently, another team of scientists (Dr. Jun Nishiyama et al.) that healthy skeletal* muscle acts as an anti-tumor organ, releasing tiny particles called extracellular vesicles (EVs) that help suppress the development of tumors.
*This means the muscles that move your skeleton, as opposed to different kinds of muscle such as, for example, the smooth muscle that operates the peristaltic motion of your intestines, or that forms the main part of the walls of your uterus (if you have one), or that wiggle your ears, and so forth.
As muscles age and lose mass (per sarcopenia), they produce fewer of these vesicles. The vesicles that are released also contain lower levels of a molecule (known as miR-7a-5p to its friends) that normally helps restrain tumor growth. As a result, aging muscle can lose a lot of its natural cancer-fighting ability.
The good news is that exercise appears to reverse part of this process. The researchers found that physical activity reactivates a biological pathway involved in EV production, restoring the release of protective signals from muscle.
In other words: exercise more (be it with aerobic activity or resistance training, though ideally both), and greatly reduce your risk of cancer.
You can find this paper in full, here: Sarcopenia promotes tumorigenesis by disrupting NOTCH-SDC2-regulated biogenesis of muscle-derived extracellular vesicles
Want to learn more?
You might like this excellent book we reviewed:
Moving Through Cancer – by Dr. Kathryn Schmitz
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Social connections, service access, language: how disability can make things even harder for refugees
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Settling in a new country as a refugee comes with a variety of opportunities and challenges, from forming social connections, to navigating government services, and many others. The challenges can be greater for refugees with disability, our new research shows.
We don’t have concrete data on how many refugees with disability have settled in Australia. But we know numbers have increased in recent years after a 2010 parliamentary inquiry recommended a policy change to reduce barriers to refugees with disability settling in Australia.
Still, there’s a significant research gap on the intersection of disability and migration in Australia. There’s also little international research on refugees with disability.
Through surveys and interviews, we explored the experiences of settlement and integration for refugees with disability in Australia.
Our 75 survey respondents were permanent residents who had lived in Australia for an average of 4.3 years. They were mostly from Iraq, Syria and Afghanistan.
For the survey, we used questions from our previous research with refugees conducted by Western Sydney University and Settlement Services International (SSI). This allowed us to put the experiences of refugees with disability into context, comparing them with refugees more broadly.
Our findings suggest intersecting issues – across domains including social connections, housing, and English language learning – influence the settlement and integration trajectories of refugees with disability in Australia.
FG Trade Latin/Getty Images Some good news
Among refugees with disability, 72% of respondents said they felt part of the Australian community always or most of the time. Some 65% rated their overall settlement experience in Australia as good or very good.
These two percentages are lower than what refugees in general reported in our previous research in 2021, wherein 87% felt part of the community and 83% had an overall positive settlement experience.
Our new research also indicates refugees with disability gain important support from their own communities.
They were more likely to feel supported or given comfort by their national and ethnic community (54%) than refugees in general (38%) in our previous research.
In their religious communities, 46% of refugees with disability felt supported. This is compared to 27% of refugees generally in our earlier research.
As Haneen, a proxy respondent for and sister of Jamal, a 56-year-old man with disability from Iraq, explained:
I go to the church on Sundays, every Sunday and Wednesday. Majority of time I try not to miss it and Jamal also joins me. My sisters and her friends, they say if you don’t bring Jamal, don’t come, we want to see Jamal be with you, they like to have him there.
A nuanced picture
Developing connections outside their own communities posed significant challenges for refugees with disability. Most found it hard or very hard to make friends in Australia (77%), to talk to their Australian neighbours (76%) and to understand Australian ways or culture (68%).
These figures were much higher than what refugees more broadly reported in our previous research: 29%, 31% and 25% respectively.
Refugees with disability said English language difficulties, compounded by experiences of disability, hampered opportunities to develop mixed social networks.
Generally, they also faced significant difficulties accessing government services. Reported reasons for this included language barriers (75%), problems using government mobile apps such as Medicare and MyGov (62%), long wait times for appointments (60%) and transport difficulties (58%). These were much higher rates than for refugees generally in our previous research.
Refugees appreciated the range of disability supports available in Australia. At the same time, they reported challenges navigating these services. Even when they accessed them successfully, some faced challenges such as inadequate hours of support from the National Disability Insurance Scheme (NDIS).
Adnan, from Afghanistan, described what would have helped him and his brother, Yazan, who has cerebral palsy:
NDIS should have a team of people [to work with refugee] families with […] a person with disability […] they should have a team that meets this person and sees the needs of this person directly, and to help […] the family to find the proper provider. Because we don’t know […] as a refugee we came with no knowledge, no experience.
Refugees with disability we spoke to described a range of challenges. Eden Connell Our respondents shared similar difficulties finding housing as other refugees. However, they were less satisfied with various aspects of their homes (for example, the number, size and accessibility of rooms).
Refugees with disability appeared strongly motivated to learn English, yet reported barriers accessing adult learning programs such as the Adult Migrant English Program. These barriers included unsuitable delivery options (for example, online-only classes), being unable to sit for long periods, and trouble with memory and learning.
Breaking down barriers
The disability royal commission highlighted that refugees with disability face a range of challenges when trying to access disability and mainstream services. As the review from the commission notes:
many organisations have policies or programs to support inclusion of people with disability and also people from CALD [culturally and linguistically diverse] backgrounds, but these policies often do not intersect, nor do they intersect with other initiatives around inclusion.
The NDIS has developed a CALD strategy for 2024–28 which outlines a series of actions to improve access by migrants and refugees with disability. This will be a positive step if implemented in full.
Although our sample size was small, our research underscores the intersecting barriers that hinder inclusion for refugees with disability. Challenges around social connections, engagement with services and other domains may be magnified by experiences of disability.
Australia has obligations under international conventions and domestic laws and policies to protect the rights of refugees and people with disability.
We urgently need policy frameworks and systems that explicitly respond to the intersecting opportunities and challenges experienced by refugees with disability.
Tadgh McMahon, Adjunct Senior Lecturer, College of Medicine and Public Health, Flinders University and Gerard Goggin, Distinguished Professor, Institute for Culture and Society, Western Sydney University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: