Moving Through Cancer – by Dr. Kathryn Schmitz
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We all know exercise is good for most things, but cancer is complicated, so… What should we do? Should we take it easy? Exercise more? Conserve energy? Can speeding up our metabolism (generally considered good) commensurately speed up the cancer (bad)?
Dr. Kathryn Schmitz is an expert in sports medicine for cancer patients, with decades of experience in that field.
Then, when her wife was diagnosed with an aggressive stage 3 cancer, Dr. Schmitz (of course) applied everything she knew, and doubled-down going through all available research with a fine-toothed comb. What was already her career, became her reason for living.
Prior to her wife getting cancer, Dr. Schmitz had already overturned the medical convention of yesteryear; it was her own research that changed mainstream policies on exercise recommendation for breast cancer patients specifically (previous advice was: avoid upper body exercise). That was about six years before her wife’s cancer diagnosis, which is at time of writing, 9 years ago now (happily, she is doing fine now, and is officially cancer-free* in the sense of “no evidence of disease”), and she’s only continued to increase her research since, to share it with us.
*this term is often avoided due to the technically non-zero chance of cancer returning, but the author uses it in this case, so we’ll use it here too.
This book covers many different kinds of cancer, with exercise protocols tailored for each, and also covers exercise in the context of surgery, chemotherapy and other infusion therapies, radiation therapies, hormonal therapies, and more.
On that note, she makes the distinction between “prehabilitation” (getting into the best possible condition before treatment) and post-treatment recovery protocols, and how to balance getting adequate exercise with getting adequate rest, during treatments of the ongoing kind (i.e. pretty much anything apart from surgery—since during surgery, one will certainly not be exercising).
All of this is very evidence-based, as one might expect from someone with her background in both academia and practice, and as such she refers to many studies throughout.
This is mostly a practical book, with direct instructions on what to do and how to do it and how to tailor it to your specific cancer/situation, with day-by-day, week-by-week plans, coupled with frequent reminders of such things as “but this adds to your stress, don’t do it; managing your stress is more important”, and “if you are unable to do the exercise on any given day, or must do a modified version, or cut your exercise short, just log that in your exercise journal and try again tomorrow”, and so forth.
That side of things is not limited to just disclaimers, either—she’s very aware, from her own experience with her wife, that fighting cancer is an emotional battle as much as a physical one, and she gives genuine attention to that too.
Bottom line: if you or a loved one has or has had cancer, this book can help survivorship and recovery, with highly specialised advice from someone who is not only a world-class expert in her field, but also very clearly cares very deeply.
Click here to check out Moving Through Cancer, and move through cancer!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

News of a ‘giant’ baby boy is all over TikTok. Here’s what women really need to know

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Baby boy Cassian is an internet sensation. He was born earlier this year in the United States weighing 5.8 kilograms. But after his mum and the hospital shared the news recently, it wasn’t long before headlines about the “giant” baby spread around the world. These included:
‘Are you OK’?: Woman breaks record with giant newborn baby
Record-breaking baby tips the scales at almost double the average size of a newborn
While baby Cassian was born heavier than average, he’s not unique. There have been other examples in the news of babies born heavier. That includes a baby boy born in Brazil in 2023 who weighed 7.3kg.
These stories might make women all over the world cross their legs. But how common are big babies, and does their birth always lead to complications?
What are big babies?
Macrosomia describes babies born over 4kg or 4.5kg, depending on the definition.
A big baby can also be defined as having a birth weight over the 90th percentile at a particular gestational age. In other words, more than 90% of babies have a lower birth weight at this particular stage of the pregnancy. The term “large for gestational age” is probably a more accurate term as the weeks of gestation is used alongside the weight.
There has been little change overall in the percentage of large babies in the past decade in Australia. While stories of such births hit the media, their proportion hovers around 9–10% of births.
What are the problems for big babies and their mums?
We don’t know the specific circumstances of Cassian’s birth, his health or that of his mother. And we don’t know whether common reasons for larger babies are relevant in this situation.
But, generally speaking, birth complications can be higher for mothers and babies when the baby is big, especially if more than 4.5kg. This is certainly not always the case, however.
There is an increased need for interventions during the birth, such as forceps or vacuum delivery, or a caesarean section the bigger the baby is. Having these interventions can impact a women’s recovery after the birth, and options for the next birth.
For the baby there are higher risks of the shoulders getting stuck in the birth canal during the birth (known as shoulder dystocia).
Midwives and obstetricians also may need to make extra manoeuvres for the baby to be safely delivered. For instance, they may need to try and bring down one shoulder if it’s stuck behind the mother’s pubic bone.
These manoeuvres can damage the baby or lead to oxygen restrictions, with the baby needing to be resuscitated. However, these complications are rare and can occur when a big baby was not expected.
What leads to a big baby?
Big babies are most often healthy babies, and there are a number of reasons for them.
Genetic factors mean babies are always big in some families.
Babies that go over their due dates tend to be a bit bigger as they have more time to grow inside their mothers.
Having diabetes, especially if this is poorly controlled, can lead to larger babies. This is because the mother’s higher blood sugar leads to the baby receiving more energy than it needs, so it stores this extra energy as fat.
Babies of mothers with diabetes diagnosed for the first time in pregnancy (gestational diabetes) are at increased risk of being obese and developing diabetes in the future.
Mothers who are larger before pregnancy, or when pregnant, may also be more likely to have big babies. This is mostly due to the increased likelihood of developing diabetes in pregnancy, and perhaps poorer nutrition choices.
Can you predict a big baby?
Estimations of babies’ weights before they are born are imprecise. That’s why so many women are told they are going to have a big baby and don’t, and others are surprised by a big baby when it arrives.
Midwives and obstetricians routinely feel a woman’s growing uterus when they provide antenatal check-ups. They are looking at the position the baby is lying in the uterus as well as where the top of the uterus is compared to the woman’s belly button. This gives an idea of whether the baby is growing as you would expect at that time.
They also measure from the top of a woman’s belly to the top of her pubic bone with a tape measure. The weeks of pregnancy usually correspond to the measurement within a couple of centimetres.
For example, at 36 weeks of pregnancy the tape measurement would be somewhere between 34cm and 38cm. If there is more or less than a 3cm difference between the measurement and the numbers of weeks of pregnancy then an ultrasound would be offered to look at how the baby’s growing and to estimate the size.
But ultrasounds are poor predictors of actual birth weight. The Big Baby Trial was published earlier this year. It randomised nearly 3,000 women in the United Kingdom to being induced at 39 weeks if suspected to be having a big baby (according to an ultrasound) or waiting for labour to start.
There was little difference in birth weight or poor outcomes, such as shoulder dystocia for the baby, leading to the trial being stopped early. Around 60% of babies screened as being big babies were not actually big at birth, showing the inaccuracy of ultrasounds in predicting birth weight.
What can women do?
The best health advice for women is to try to be a healthy weight (under a BMI of 30) before getting pregnant.
Eat a balanced diet and limit your intake of foods and drinks high in saturated fats and sugar. Try not to put too much weight on during pregnancy and exercise regularly. Talk to your midwife or obstetrician for advice and support about this.
If you have diabetes, or if this has been diagnosed during the pregnancy, close monitoring of your blood sugar and baby’s growth is important.
Hannah Dahlen, Professor of Midwifery, Associate Dean Research and HDR, Midwifery Discipline Leader, Western Sydney University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Air Purifiers & Sleep
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝I’ve read that air pollution has a negative effect on sleep quality and duration. Since I live next to a busy road, I was wondering whether I should invest in an air purifier. What are 10Almonds’s views?❞
Going straight to the science, there are two questions here:
- Does air pollution negatively affect sleep quality and duration?
- Does the use of an air purify actually improve the air quality in the way(s) necessary to make a difference?
We thought we’d have to tackle these questions separately, but we did find one study that addressed your question directly. It was a small study (n=30 if you believe the abstract; n=29 if you read the paper itself—one person dropped out); the results were modest but clear:
❝The purifier filter was associated with increased total sleep time for an average of 12 min per night, and increased total time in bed for an average of 19 min per night relative to the placebo.
There were several sleep and mood outcomes for which no changes were observed, and time awake after sleep onset was higher for the purifier filter. Air quality was better during the high-efficiency particulate air filter condition.
These findings offer positive indications that environmental interventions that improve air quality can have benefits for sleep outcomes in healthy populations who are not exhibiting clinical sleep disturbances.❞
In the above-linked paper’s introduction, it does establish the deleterious effect of air pollution on a wide variety of health metrics, including sleep, this latter evidenced per Caddick et al. (2018): A review of the environmental parameters necessary for an optimal sleep environment
Now, you may be wondering: is an extra 12 minutes per night worth it?
That’s your choice to make, but we would argue that it is. We can make many choices in our lives that affect our health slightly for the better or the worse. If we make a stack of choices in a particular direction, the effects will also stack, if not outright compound.
So in the case of sleep, it might be (arbitrary numbers for the sake of illustration):
- Get good exercise earlier in the day (+3%)
- Get good food earlier in the day (+2.5%)
- Practice mindfulness/meditation before bed (+2.5%)
- Have a nice dark room (+5%)
- Have fresh bedding (+2.5%)
- Have an air purifier running (+3%)
Now, those numbers are, as we said, arbitrary*, but remember that percentages don’t add up; they compound. So that “+3%” starts being a lot more meaningful than if it were just by itself.
*Confession: the figure of 3% for the air purifier wasn’t entirely arbitrary; it was based on 100(12/405) = 80/27 ≈ 3, wherein the 405 figure was an approximation of the average total time (in minutes) spent sleeping with placebo, based on a peep at their results graph. There are several ways the average could be reasonably calculated, but 6h45 (i.e., 405 minutes) was an approximate average of those reasonable approximate averages.
So, 12 minutes is a 3% improvement on that.
Don’t have an air purifier and want one?
We don’t sell them, but here’s an example on Amazon, for your convenience
Take care!
Share This Post
-
America’s Health System Isn’t Ready for the Surge of Seniors With Disabilities
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The number of older adults with disabilities — difficulty with walking, seeing, hearing, memory, cognition, or performing daily tasks such as bathing or using the bathroom — will soar in the decades ahead, as baby boomers enter their 70s, 80s, and 90s.
But the health care system isn’t ready to address their needs.
That became painfully obvious during the covid-19 pandemic, when older adults with disabilities had trouble getting treatments and hundreds of thousands died. Now, the Department of Health and Human Services and the National Institutes of Health are targeting some failures that led to those problems.
One initiative strengthens access to medical treatments, equipment, and web-based programs for people with disabilities. The other recognizes that people with disabilities, including older adults, are a separate population with special health concerns that need more research and attention.
Lisa Iezzoni, 69, a professor at Harvard Medical School who has lived with multiple sclerosis since her early 20s and is widely considered the godmother of research on disability, called the developments “an important attempt to make health care more equitable for people with disabilities.”
“For too long, medical providers have failed to address change in society, changes in technology, and changes in the kind of assistance that people need,” she said.
Among Iezzoni’s notable findings published in recent years:
Most doctors are biased. In survey results published in 2021, 82% of physicians admitted they believed people with significant disabilities have a worse quality of life than those without impairments. Only 57% said they welcomed disabled patients.
“It’s shocking that so many physicians say they don’t want to care for these patients,” said Eric Campbell, a co-author of the study and professor of medicine at the University of Colorado.
While the findings apply to disabled people of all ages, a larger proportion of older adults live with disabilities than younger age groups. About one-third of people 65 and older — nearly 19 million seniors — have a disability, according to the Institute on Disability at the University of New Hampshire.
Doctors don’t understand their responsibilities. In 2022, Iezzoni, Campbell, and colleagues reported that 36% of physicians had little to no knowledge of their responsibilities under the 1990 Americans With Disabilities Act, indicating a concerning lack of training. The ADA requires medical practices to provide equal access to people with disabilities and accommodate disability-related needs.
Among the practical consequences: Few clinics have height-adjustable tables or mechanical lifts that enable people who are frail or use wheelchairs to receive thorough medical examinations. Only a small number have scales to weigh patients in wheelchairs. And most diagnostic imaging equipment can’t be used by people with serious mobility limitations.
Iezzoni has experienced these issues directly. She relies on a wheelchair and can’t transfer to a fixed-height exam table. She told me she hasn’t been weighed in years.
Among the medical consequences: People with disabilities receive less preventive care and suffer from poorer health than other people, as well as more coexisting medical conditions. Physicians too often rely on incomplete information in making recommendations. There are more barriers to treatment and patients are less satisfied with the care they do get.
Egregiously, during the pandemic, when crisis standards of care were developed, people with disabilities and older adults were deemed low priorities. These standards were meant to ration care, when necessary, given shortages of respirators and other potentially lifesaving interventions.
There’s no starker example of the deleterious confluence of bias against seniors and people with disabilities. Unfortunately, older adults with disabilities routinely encounter these twinned types of discrimination when seeking medical care.
Such discrimination would be explicitly banned under a rule proposed by HHS in September. For the first time in 50 years, it would update Section 504 of the Rehabilitation Act of 1973, a landmark statute that helped establish civil rights for people with disabilities.
The new rule sets specific, enforceable standards for accessible equipment, including exam tables, scales, and diagnostic equipment. And it requires that electronic medical records, medical apps, and websites be made usable for people with various impairments and prohibits treatment policies based on stereotypes about people with disabilities, such as covid-era crisis standards of care.
“This will make a really big difference to disabled people of all ages, especially older adults,” said Alison Barkoff, who heads the HHS Administration for Community Living. She expects the rule to be finalized this year, with provisions related to medical equipment going into effect in 2026. Medical providers will bear extra costs associated with compliance.
Also in September, NIH designated people with disabilities as a population with health disparities that deserves further attention. This makes a new funding stream available and “should spur data collection that allows us to look with greater precision at the barriers and structural issues that have held people with disabilities back,” said Bonnielin Swenor, director of the Johns Hopkins University Disability Health Research Center.
One important barrier for older adults: Unlike younger adults with disabilities, many seniors with impairments don’t identify themselves as disabled.
“Before my mom died in October 2019, she became blind from macular degeneration and deaf from hereditary hearing loss. But she would never say she was disabled,” Iezzoni said.
Similarly, older adults who can’t walk after a stroke or because of severe osteoarthritis generally think of themselves as having a medical condition, not a disability.
Meanwhile, seniors haven’t been well integrated into the disability rights movement, which has been led by young and middle-aged adults. They typically don’t join disability-oriented communities that offer support from people with similar experiences. And they don’t ask for accommodations they might be entitled to under the ADA or the 1973 Rehabilitation Act.
Many seniors don’t even realize they have rights under these laws, Swenor said. “We need to think more inclusively about people with disabilities and ensure that older adults are fully included at this really important moment of change.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Share This Post


Related Posts
-

The Little-Known Truth…
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Myth-Buster, Myth-Buster, Bust Us A Myth (or three!)
Let’s can this myth for good
People think of “canned foods” as meaning “processed foods” and therefore bad. But the reality is it’s all dependent on what’s in the can (check the ingredients!). And as for nutrients?
Many canned fruits and vegetables contain more nutrients than fresh ones! This is because the way they’ve been stored preserves them better. For example:
- Canned tomatoes contain more bioavailable lycopene than fresh
- Canned spinach contains more bioavailable carotene than fresh
- Canned corn contains more bioavailable lutein than fresh
- The list goes on, but you get the idea!
Don’t Want To Take Our Word For It? Read The Scientific Paper Here!
Gaslight, Gymkeep, Girl-loss?
Many women and girls avoid doing weight-training as part of their exercise—or use only the smallest weights—to avoid “bulking up” and “looking like a man”.
Many men, meanwhile, wish it were that easy to bulk up!
The reality is that nobody, unless you have very rare genes, packs on a lot of muscle by accident. Even with the genes for it, it won’t happen unless you’re also eating for it!
Resistance-based strength training (such as lifting weights), is a great way for most people to look after an important part of their long-term health: bone density!
You can’t have strong muscles on weak bones, so strengthening the muscles cues the body to strengthen the bones. In short, your strength-training at age 45 or 55 (or earlier) could be what helps you avoid a broken hip at 65 or 75.
We’re Not Kidding, It Really Is That Important (Read The Study Here)!
Something doesn’t smell right about this
There’s been a big backlash against anti-perspirants and deodorants. The popular argument is that the aluminium in them causes cancer.
This led to many people buying “deodo-rocks”, crystal rocks that can be run under water and then rubbed on the armpits to deodorize “naturally”. But, those crystal rocks are actually alum crystals (guess what they contain…).
The belief that deodorants cause cancer came from studies done by applying deodorant to cells (like the canine kidney cells in this study) in petri dishes. So, assuming you don’t cut out your kidney and then spray it directly with the deodorant, the jury is still out!
A more recent systematic review sorted out quite clearly the ways in which aluminium was, or was not, harmful, and said:
❝Neither is there clear evidence to show use of Al-containing underarm antiperspirants or cosmetics increases the risk of Alzheimer’s Disease or breast cancer. Metallic Al, its oxides, and common Al salts have not been shown to be either genotoxic or carcinogenic.❞
Critical Reviews in Toxicology
…but also says that you should avoid eating aluminium while pregnant or breastfeeding. We hope you can resist the urge.
See The Summary For Yourself Here!
(actually the whole article is there, but we know you value condensed knowledge, so: the abstract at the top will probably tell you all you want to know!)
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Do you have knee pain from osteoarthritis? You might not need surgery. Here’s what to try instead
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Most people with knee osteoarthritis can control their pain and improve their mobility without surgery, according to updated treatment guidelines from the Australian Commission on Safety and Quality in Health Care.
So what is knee osteoarthritis and what are the best ways to manage it?

Pexels/Kindelmedia More than 2 million Australians have osteoarthritis
Osteoarthritis is the most common joint disease, affecting 2.1 million Australians. It costs the economy A$4.3 billion each year.
Osteoarthritis commonly affects the knees, but can also affect the hips, spine, hands and feet. It impacts the whole joint including bone, cartilage, ligaments and muscles.
Most people with osteoarthritis have persistent pain and find it difficult to perform simple daily tasks, such as walking and climbing stairs.
Is it caused by ‘wear and tear’?
Knee osteoarthritis is most likely to affect older people, those who are overweight or obese, and those with previous knee injuries. But contrary to popular belief, knee osteoarthritis is not caused by “wear and tear”.
Research shows the degree of structural wear and tear visible in the knee joint on an X-ray does not correlate with the level of pain or disability a person experiences. Some people have a low degree of structural wear and tear and very bad symptoms, while others have a high degree of structural wear and tear and minimal symptoms. So X-rays are not required to diagnose knee osteoarthritis or guide treatment decisions.
Telling people they have wear and tear can make them worried about their condition and afraid of damaging their joint. It can also encourage them to try invasive and potentially unnecessary treatments such as surgery. We have shown this in people with osteoarthritis, and other common pain conditions such as back and shoulder pain.
This has led to a global call for a change in the way we think and communicate about osteoarthritis.
What’s the best way to manage osteoarthritis?
Non-surgical treatments work well for most people with osteoarthritis, regardless of their age or the severity of their symptoms. These include education and self-management, exercise and physical activity, weight management and nutrition, and certain pain medicines.
Education is important to dispel misconceptions about knee osteoarthritis. This includes information about what osteoarthritis is, how it is diagnosed, its prognosis, and the most effective ways to self-manage symptoms.
Health professionals who use positive and reassuring language can improve people’s knowledge and beliefs about osteoarthritis and its management.
Many people believe that exercise and physical activity will cause further damage to their joint. But it’s safe and can reduce pain and disability. Exercise has fewer side effects than commonly used pain medicines such as paracetamol and anti-inflammatories and can prevent or delay the need for joint replacement surgery in the future.
Many types of exercise are effective for knee osteoarthritis, such as strength training, aerobic exercises like walking or cycling, Yoga and Tai chi. So you can do whatever type of exercise best suits you.
Increasing general physical activity is also important, such as taking more steps throughout the day and reducing sedentary time.
Weight management is important for those who are overweight or obese. Weight loss can reduce knee pain and disability, particularly when combined with exercise. Losing as little as 5–10% of your body weight can be beneficial.
Pain medicines should not replace treatments such as exercise and weight management but can be used alongside these treatments to help manage pain. Recommended medicines include paracetamol and non-steroidal anti-inflammatory drugs.
Opioids are not recommended. The risk of harm outweighs any potential benefits.
What about surgery?
People with knee osteoarthritis commonly undergo two types of surgery: knee arthroscopy and knee replacement.
Knee arthroscopy is a type of keyhole surgery used to remove or repair damaged pieces of bone or cartilage that are thought to cause pain.
However, high-quality research has shown arthroscopy is not effective. Arthroscopy should therefore not be used in the management of knee osteoarthritis.
Joint replacement involves replacing the joint surfaces with artificial parts. In 2021–22, 53,500 Australians had a knee replacement for their osteoarthritis.
Joint replacement is often seen as being inevitable and “necessary”. But most people can effectively manage their symptoms through exercise, physical activity and weight management.
The new guidelines (known as “care standard”) recommend joint replacement surgery only be considered for those with severe symptoms who have already tried non-surgical treatments.
I have knee osteoarthritis. What should I do?
The care standard links to free evidence-based resources to support people with osteoarthritis. These include:
- education, such as a decision aid and four-week online course
- self-directed online exercise and yoga programs
- weight management support
- pain management strategies, such as MyJointPain and painTRAINER.
If you have osteoarthritis, you can use the care standard to inform discussions with your health-care provider, and to make informed decisions about your care.
Belinda Lawford, Postdoctoral research fellow in physiotherapy, The University of Melbourne; Giovanni E. Ferreira, NHMRC Emerging Leader Research Fellow, Institute of Musculoskeletal Health, University of Sydney; Joshua Zadro, NHMRC Emerging Leader Research Fellow, Sydney Musculoskeletal Health, University of Sydney, and Rana Hinman, Professor in Physiotherapy, The University of Melbourne
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Some women’s breasts can’t make enough milk, and the effects can be devastating
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Many new mothers worry about their milk supply. For some, support from a breastfeeding counsellor or lactation consultant helps.
Others cannot make enough milk no matter how hard they try. These are women whose breasts are not physically capable of producing enough milk.
Our recently published research gives us clues about breast features that might make it difficult for some women to produce enough milk. Another of our studies shows the devastating consequences for women who dream of breastfeeding but find they cannot.
Some breasts just don’t develop
Unlike other organs, breasts are not fully developed at birth. There are key developmental stages as an embryo, then again during puberty and pregnancy.
At birth, the breast consists of a simple network of ducts. Usually during puberty, the glandular (milk-making) tissue part of the breast begins to develop and the ductal network expands. Then typically, further growth of the ductal network and glandular tissue during pregnancy prepares the breast for lactation.
But our online survey of women who report low milk supply gives us clues to anomalies in how some women’s breasts develop.
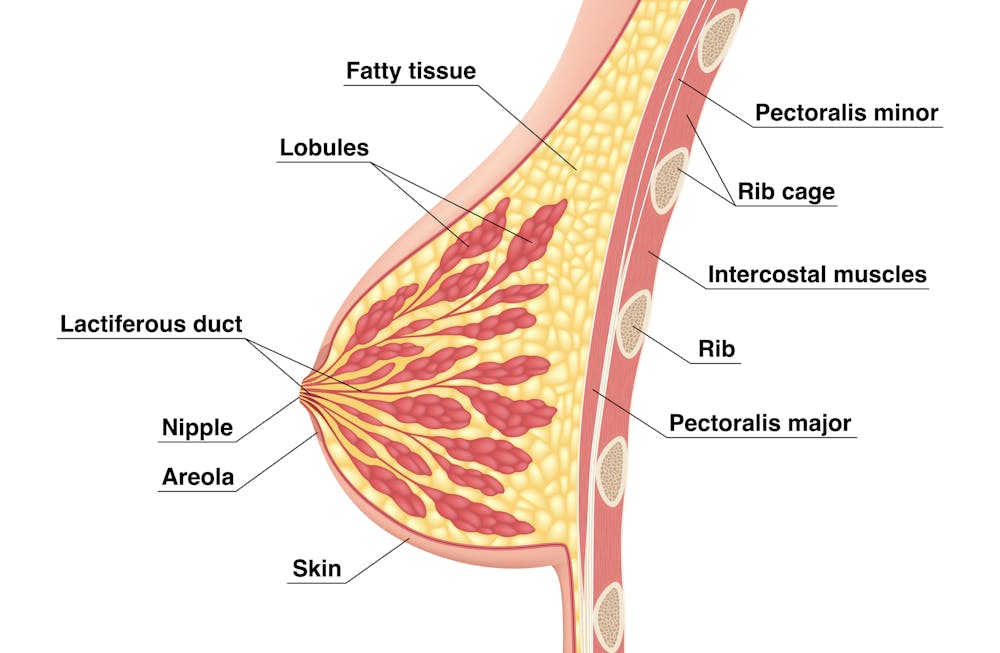
We’re not talking about women with small breasts, but women whose glandular tissue (shown in this diagram as “lobules”) is underdeveloped and have a condition called breast hypoplasia.
Sometimes not enough glandular tissue, shown here as lobules, develop.
Tsuyna/ShutterstockWe don’t know how common this is. But it has been linked with lower rates of exclusive breastfeeding.
We also don’t know what causes it, with much of the research conducted in animals and not humans.
However, certain health conditions have been associated with it, including polycystic ovary syndrome and other endocrine (hormonal) conditions. A high body-mass index around the time of puberty may be another indicator.
Could I have breast hypoplasia?
Our survey and other research give clues about who may have breast hypoplasia.
But it’s important to note these characteristics are indicators and do not mean women exhibiting them will definitely be unable to exclusively breastfeed.
Indicators include:
- a wider than usual gap between the breasts
- tubular-shaped (rather than round) breasts
- asymmetric breasts (where the breasts are different sizes or shapes)
- lack of breast growth in pregnancy
- a delay in or absence of breast fullness in the days after giving birth
In our survey, 72% of women with low milk supply had breasts that did not change appearance during pregnancy, and about 70% reported at least one irregular-shaped breast.
The effects
Mothers with low milk supply – whether or not they have breast hyoplasia or some other condition that limits their ability to produce enough milk – report a range of emotions.
Research, including our own, shows this ranges from frustration, confusion and surprise to intense or profound feelings of failure, guilt, grief and despair.
Some mothers describe “breastfeeding grief” – a prolonged sense of loss or failure, due to being unable to connect with and nourish their baby through breastfeeding in the way they had hoped.
These feelings of failure, guilt, grief and despair can trigger symptoms of anxiety and depression for some women.
Feelings of failure, guilt, grief and despair were common.
Bricolage/ShutterstockOne woman told us:
[I became] so angry and upset with my body for not being able to produce enough milk.
Many women’s emotions intensified when they discovered that despite all their hard work, they were still unable to breastfeed their babies as planned. A few women described reaching their “breaking point”, and their experience felt “like death”, “the worst day of [my] life” or “hell”.
One participant told us:
I finally learned that ‘all women make enough milk’ was a lie. No amount of education or determination would make my breasts work. I felt deceived and let down by all my medical providers. How dare they have no answers for me when I desperately just wanted to feed my child naturally.
Others told us how they learned to accept their situation. Some women said they were relieved their infant was “finally satisfied” when they began supplementing with formula. One resolved to:
prioritise time with [my] baby over pumping for such little amounts.
Where to go for help
If you are struggling with low milk supply, it can help to see a lactation consultant for support and to determine the possible cause.
This will involve helping you try different strategies, such as optimising positioning and attachment during breastfeeding, or breastfeeding/expressing more frequently. You may need to consider taking a medication, such as domperidone, to see if your supply increases.
If these strategies do not help, there may be an underlying reason why you can’t make enough milk, such as insufficient glandular tissue (a confirmed inability to make a full supply due to breast hypoplasia).
Even if you have breast hypoplasia, you can still breastfeed by giving your baby extra milk (donor milk or formula) via a bottle or using a supplementer (which involves delivering milk at the breast via a tube linked to a bottle).
More resources
The following websites offer further information and support:
- Australian Breastfeeding Association
- Lactation Consultants of Australia and New Zealand
- Royal Women’s Hospital, Melbourne
- Supply Line Breastfeeders Support Group of Australia Facebook support group
- IGT And Low Milk Supply Support Group Facebook support group
- Breastfeeding Medicine Network Australia/New Zealand
- Supporting breastfeeding grief (a collection of resources).
Shannon Bennetts, a research fellow at La Trobe University, contributed to this article.

Renee Kam, PhD candidate and research officer, La Trobe University and Lisa Amir, Professor in Breastfeeding Research, La Trobe University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: