Discipline is Destiny – by Ryan Holiday
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve previously reviewed another of Holiday’s books, The Daily Stoic, and here is another excellent work from the same author.
We’re not a philosophy newsletter, but there are some things that make a big difference to physical and mental health, the habits we build, and the path we take in life for better or for worse.
Self-discipline is one of those things. A lot of the time, we know what we need to do, but knowing isn’t the problem. We need to actually do it! This applies to diet, exercise, sleep, and more.
Holiday gives us, in a casual easy-reading style, timeless principles to lock in strong discipline and good habits for life.
The book’s many small chapters, by the way, are excellent for reading a chapter-per-day as a healthy dose of motivation each morning, if you’re so inclined.
Bottom line: if you’ve noticed that one of the biggest barriers between you and your goals is actually doing the necessary things in a disciplined fashion, then this book will help you become more efficient, and actually get there.
Click here to check out Discipline is Destiny, and upgrade yours!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Flexible Dieting – by Alan Aragon

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This is the book from which we were working, for the most part, in our recent Expert Insights feature with Alan Aragon. We’ll re-iterate here: despite not being a Dr. Aragon, he’s a well-published research scientist with decades in the field of nutritional science, as well as being a personal trainer and fitness educator.
As you may gather from our other article, there’s a lot more to this book than “eat what you like”. Specifically, as the title suggests, there’s a lot of science—decades of it, and while we had room to cite a few studies in our article, he cites many many more; several citations per page of a 288-page book.
So, that sets the book apart from a lot of its genre; instead of just “here’s what some gym-bro thinks”, it’s “here’s what decades of data says”.
Another strength of this book is how clearly he explains such a lot of science—he explains terms as they come up, as well as having a generous glossary. He also explains things clearly and simply without undue dumbing down—just clarity of communication.
The style is to-the-point and instructional; it’s neither full of fitness-enthusiast hype nor dry academia, and keeps a light and friendly conversational tone throughout.
Bottom line: if you’d like to get your diet in order and you want to do it right while also knowing which things still need attention (and why) and which you can relax about (and why), then this book will get you there.
Click here to check out Flexible Dieting, and take an easy, relaxed control of yours!
Share This Post
-

Syphilis Is Killing Babies. The U.S. Government Is Failing to Stop the Disease From Spreading.
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
ProPublica is a Pulitzer Prize-winning investigative newsroom. Sign up for The Big Story newsletter to receive stories like this one in your inbox.
Karmin Strohfus, the lead nurse at a South Dakota jail, punched numbers into a phone like lives depended on it. She had in her care a pregnant woman with syphilis, a highly contagious, potentially fatal infection that can pass into the womb. A treatment could cure the woman and protect her fetus, but she couldn’t find it in stock at any pharmacy she called — not in Hughes County, not even anywhere within an hour’s drive.
Most people held at the jail where Strohfus works are released within a few days. “What happens if she gets out before I’m able to treat her?” she worried. Exasperated, Strohfus reached out to the state health department, which came through with one dose. The treatment required three. Officials told Strohfus to contact the federal Centers for Disease Control and Prevention for help, she said. The risks of harm to a developing baby from syphilis are so high that experts urge not to delay treatment, even by a day.
Nearly three weeks passed from when Strohfus started calling pharmacies to when she had the full treatment in hand, she said, and it barely arrived in time. The woman was released just days after she got her last shot.
Last June, Pfizer, the lone U.S. manufacturer of the injections, notified the Food and Drug Administration of an “impending stock out” that it anticipated would last a year. The company blamed “an increase in syphilis infection rates as well as competitive shortages.”
Across the country, physicians, clinic staff and public health experts say that the shortage is preventing them from reining in a surge of syphilis and that the federal government is downplaying the crisis. State and local public health authorities, which by law are responsible for controlling the spread of infectious diseases, report delays getting medicine to pregnant people with syphilis. This emergency was predictable: There have been shortages of this drug in eight of the last 20 years.
Yet federal health authorities have not prevented the drug shortages in the past and aren’t doing much to prevent them in the future.
Syphilis, which is typically spread during sex, can be devastating if it goes untreated in pregnancy: About 40% of babies born to women with untreated syphilis can be stillborn or die as newborns, according to the CDC. Infants that survive can suffer from deformed bones, excruciating pain or brain damage, and some struggle to hear, see or breathe. Since this is entirely preventable, a baby born with syphilis is a shameful sign of a failing public health system.
In 2022, the most recent year for which the CDC has data available, more than 3,700 babies were infected with syphilis, including nearly 300 who were stillborn or died as infants. More than 50% of these cases occurred because, even though the pregnant parent was diagnosed with syphilis, they were never properly treated.
That year, there were 200,000 cases identified in the U.S., a 79% increase from five years before. Infection rates among pregnant people and babies increased by more than 250% in that time; South Dakota, where Strohfus works, had the highest rates — including a more than 400% increase among pregnant women. Statewide, the rate of babies born with the disease, a condition known as congenital syphilis, jumped more than 40-fold in just five years.
And that was before the current shortage of shots.
In Mississippi, the state with the second highest rate of syphilis in pregnant women, Dr. Caroline Weinberg started having trouble this summer finding treatments for her clinic’s patients, most of whom are uninsured, live in poverty or lack transportation. She began spending hours each month scouring medicine suppliers’ websites for available doses of the shots, a form of penicillin sold under the brand name Bicillin L-A.
“The way people do it for Taylor Swift, that’s how I’ve been with the Bicillin shortage,” Weinberg said. “Desperately checking the websites to see what I can snag.”
The shortage is driving up infection rates even further.
In a November survey by the National Coalition of STD Directors, 68% of health departments that responded said the drug shortage will cause syphilis rates in their area to increase, further crushing the nation’s most disadvantaged populations.
“This is the most basic medicine,” said Meghan O’Connell, chief public health officer for the Great Plains Tribal Leaders’ Health Board, which represents 18 tribal communities in South Dakota and three other states. “We allow ourselves to continue to not have enough, and it impacts so many people.”
ProPublica examined what the federal government has done to manage the crisis and the ways in which experts say it has fallen short.
The government could pressure Pfizer to be more transparent.
Twenty years ago, there were at least three manufacturers of the syphilis shot. Then Pfizer, one of the manufacturers, purchased the other two companies and became the lone U.S. supplier.
Pfizer’s supply has fallen short since then. In 2016, the company announced a shortage due to a manufacturing issue; it lasted two years. Even during times when Pfizer had not notified the FDA of an official shortage, clinics across the country told ProPublica, the shots were often hard to get.
Several health officials said they would like to see the government use its power as the largest purchaser of the drug to put pressure on Pfizer to produce adequate supplies and to be more transparent about how much of the drug they have on hand, when it will be widely available and how stable the supply will be going forward.
In response to questions, Pfizer said there are two reasons its supply is falling short. One, the company said, was a surge in use of the pediatric form of the drug after a shortage of a different antibiotic last winter. Pfizer also blamed a 70% increase in demand for the adult shots since last February, which it described as unexpected.
Public health experts say the increase in cases and subsequent rise in demand was easy to see coming. Officials have been raising the alarm about skyrocketing syphilis cases for years. “If Pfizer was truly caught completely off guard, it raises significant questions about the competency of the company to forecast obvious infectious disease trends,” a coalition of organizations wrote to the White House Drug Shortage Task Force in September.
Pfizer said it is consistently communicating with the CDC and FDA about its supply and that it has been transparent with public health groups and policymakers.
The FDA has a group dedicated to addressing drug shortages. But Valerie Jensen, associate director of that staff, said the FDA can’t force manufacturers to make more of a drug. “It is up to manufacturers to decide how to respond to that increased demand.” she said. “What we’re here to do is help with those plans.”
Pfizer said it had a target of increasing production by about 20% in 2023 but faced delays toward the end of the year. The company did not explain the reason for those delays.
The company said it has invested $38 million in the last five years in the Michigan facility where it makes the shots and that it is increasing production capacity. It also said it is adding evening shifts at the facility and actively recruiting and training new workers. Pfizer said it also reduced manufacturing time from 110 to 50 days. By the end of June, the company expects the supply to recover, which it described as having eight weeks of inventory based on its forecast demands with no disruptions in sight.
The government could manufacture the drug itself.
Having only one supplier for a drug, especially one of public health importance, makes the country vulnerable to shortages. With just one manufacturer, any disruption — contamination at a plant, a shortage of raw materials, a severe weather event or a flawed prediction of demand — can put lives at risk. What’s ultimately needed, public health experts say, is another manufacturer.
Congressional Democrats recently introduced a bill that would authorize the U.S. Department of Health and Human Services to manufacture generic drugs in exactly this scenario, when there are few manufacturers and regular shortages. Called the Affordable Drug Manufacturing Act, it would also establish an office of drug manufacturing.
This same bill was introduced in 2018, but it didn’t have bipartisan support and was never taken up for a vote. Sen. Elizabeth Warren, the Massachusetts Democrat who introduced the bill in the Senate, said she’s hopeful this time will be different. Lawmakers from both parties understand the risks created by drug shortages, and COVID-19 helped everyone understand the role the government can play to boost manufacturing.
Still, it’s unlikely to be passed with the current gridlock in Congress.
The government could reserve syphilis drugs for infected patients.
Responding to the shortage of shots to treat the disease, the CDC in July asked health care providers nationwide to preserve the scarce remaining doses for people who are pregnant. The shots are considered the gold standard treatment for anyone with syphilis, faster and with fewer side effects than an alternative pill regimen. And for people who are pregnant, the pills are not an option; the shots are the only safe treatment.
Despite that call, the military is giving shots to new recruits who don’t have syphilis, to prevent outbreaks of severe bacterial respiratory infections. The Army has long administered this treatment at boot camps held at Fort Leonard Wood, Fort Moore and Fort Sill. The Army has been unable to obtain the shots several times in the past few years, according to the U.S. Army Center for Initial Military Training. But the Defense Health Agency’s pharmacy operations center has been working with Pfizer to ensure military sites can get them, a spokesperson for the Defense Health Agency said.
“Until we think about public health the way we think about our military, we’re not going to see a difference,” said Dr. John Vanchiere, chief of pediatric infectious diseases at Louisiana State University Health Shreveport.
Some public health officials, including Alaska’s chief medical officer, Dr. Anne Zink, questioned whether the military should be using scarce shots for prevention.
“We should ask if that’s the best use,” she said.
Using antibiotics to prevent streptococcal outbreaks is a well-established, evidence-based public health practice that’s also used by other branches of the armed services, said Lt. Col. Randy Ready, a public affairs officer with the Army’s Initial Military Training center. “The Army continues to work with the CDC and the entire medical community in regards to public health while also taking into account the unique missions and training environments our Soldiers face,” including basic training, Ready said in a written statement.
The government isn’t stockpiling syphilis drugs.
In rare instances, the federal government has created stockpiles of drugs considered key to public health. In 2018, confronting shortages of various drugs to treat tuberculosis, the CDC created a small stockpile of them. And the federal Administration for Strategic Preparedness and Response keeps a national stockpile of supplies necessary for public health emergencies, including vaccines, medical supplies and antidotes needed in case of a chemical warfare attack.
In November, the Biden administration announced it was creating a new syphilis task force. When asked why the federal government doesn’t stockpile syphilis treatments, Adm. Rachel Levine, the HHS official who leads the task force, said officials don’t routinely stockpile drugs, because they have expiration dates.
In a written statement, an HHS spokesperson said that Bicillin has a shelf life of two years and that the Strategic National Stockpile “does not deploy products that are commercially available.” In general, the spokesperson wrote, stockpiles are most effective before a national shortage begins and can’t overcome the problems of limited suppliers or fragile supply chains. “There is also a risk that stockpiles can exacerbate shortages, particularly when supply is already low, by removing drugs from circulation that would have otherwise been available,” the spokesperson wrote.
Stephanie Pang, a senior director with the coalition of STD directors, said that given the critical role of this drug and the severe access concerns, she thinks a stockpile is necessary. “I don’t have another solution that actually gets drugs to patients,” Pang said.
The government could declare a federal emergency.
Some public health officials say the federal government needs to treat the syphilis crisis the way it did Ebola or monkeypox.
Declare a federal emergency, said Dr. Michael Dube, an infectious disease specialist for more than 30 years. That would free up money for more public health staff and fund more creative approaches that could lead to a long-term solution to the near-constant shortages, he said. “I’d hate to have to wait for some horrible anecdotes to get out there in order to get the public’s and the policymakers’ minds on it,” said Dube, who oversees medical care for AIDS Healthcare Foundation wellness clinics across the country.
Citing an alarming surge in syphilis cases, the Great Plains Tribes wrote to the HHS secretary last week asking that the agency declare a public health emergency in their areas. In the request, they asked HHS to work globally to find adequate syphilis treatment and send the needed medicine to the Great Plains region.
During the 2014 outbreak of Ebola in West Africa, Congress gave hundreds of millions of dollars to HHS to help develop new rapid tests and vaccines. Facing a global outbreak of monkeypox in 2022, a White House task force deployed more than a million vaccines, regularly briefed the public and sent extra resources to Pride parades and other places where people at risk were gathered.
Levine, leader of the federal syphilis task force, countered that declaring an emergency wouldn’t make much of a difference. The government, she said, already has a “dramatic and coordinated response” involving several agencies.
The FDA recently approved an emergency import of a similar syphilis treatment made by a French manufacturer that had plenty on hand. According to the company, Provepharm, the imported shots are enough to cover approximately one or two months of typical use by all people in the U.S. (The FDA would not say how many doses Provepharm sent, and the company said it was not allowed to reveal that number under the federal rules governing such emergency imports.)
Clinics applaud that development. But many of them can’t afford the imported shots.
The government could do more to rein in the cost.
Clinics and hospitals that primarily serve low-income patients often qualify for a federal program that allows them to purchase drugs at steeply discounted prices. Pharmaceutical companies that want Medicaid to cover their outpatient drugs must participate in the program.
One factor in determining the discount price is whether a pharmaceutical company has raised the price of a drug by more than the rate of inflation. Because Pfizer has hiked the price of its Bicillin shots significantly over the years, the government requires that it be sold to qualifying clinics for just pennies a dose. Otherwise, a single Pfizer shot can retail for upwards of $500. The French shots are comparable in retail price and not eligible for the discount program.
Several clinic directors also said they worried that drug distributors were reserving the limited supply of the Pfizer shot for organizations that could pay full price. For several days in January, for example, the website of Henry Schein, a medical supplier, showed doses of the shot available at full price, while doses at the penny pricing were out of stock, according to screenshots shared with ProPublica. When asked whether it was only selling shots at full price, a spokesperson for Henry Schein did not respond to the question.
Local health departments that qualify for the discount program told ProPublica they’ve had to pay full price at other distributors, because it was the only stock available.
The Health Resources and Services Administration, the federal agency that regulates the discount program, said that a drug manufacturer is ultimately responsible for ensuring that when supplies are available, they are available at the discounted price. When asked about this, Pfizer said that it has “one inventory that is distributed to our trade partners” and that hospitals and clinics that qualify for the discount program are “responsible for ensuring compliance with the program and orders through the wholesaler accordingly.” The company added, “Pfizer plays no part in this process.”
In October, on Weinberg’s regular search for shots for her Mississippi clinic, she found doses of Bicillin for sale at the discounted price and purchased 40. “The idea that we’re supposed to be hoarding treatment is a horrific compact,” she said. Word got out that the clinic, called Plan A, has some shots, and other clinics began sending pregnant patients there.
The clinic’s supply is dwindling. Weinberg is happy to get the shots to patients who need them. But she’s not sure how much longer her reserve will last — or if she’ll be able to find more when they’re gone.
Share This Post
-

Why Diets Make Us Fat – by Dr. Sandra Aamodt
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s well-known that crash-dieting doesn’t work. Restrictive diets will achieve short-term weight loss, but it’ll come back later. In the long term, weight creeps slowly upwards. Why?
Dr. Sandra Aamodt explores the science and sociology behind this phenomenon, and offers an evidence-based alternative.
A lot of the book is given over to explanations of what is typically going wrong—that is the title of the book, after all. From metabolic starvation responses to genetics to the negative feedback loop of poor body image, there’s a lot to address.
However, what alternative does she propose?
The book takes us on a shift away from focusing on the numbers on the scale, and more on building consistent healthy habits. It might not feel like it if you desperately want to lose weight, but it’s better to have healthy habits at any weight, than to have a wreck of physical and mental health for the sake of a lower body mass.
Dr. Aamodt lays out a plan for shifting perspectives, building health, and letting weight loss come by itself—as a side effect, not a goal.
In fact, as she argues (in agreement with the best current science, science that we’ve covered before at 10almonds, for that matter), that over a certain age, people in the “overweight” category of BMI have a reduced mortality risk compared to those in the “healthy weight” category. It really underlines how there’s no point in making oneself miserably unhealthy with the end goal of having a lighter coffin—and getting it sooner.
Bottom line: will this book make you hit those glossy-magazine weight goals by your next vacation? Quite possibly not, but it will set you up for actually healthier living, for life, at any weight.
Click here to check out Why Diets Make Us Fat, and live healthier and better!
Share This Post
Related Posts
-

How To Keep On Keeping On?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How To Keep On Keeping On… Long Term!
For many when it comes to health-related goals and practices, it’s easy to find ourselves in a bit of a motivational dip around this time of year. The enthusiasm of new year’s resolutions has been and gone, and there’s not yet much of a drive to “get a beach body” or “be summer-ready”.
A word to the wise on those before moving on, though:
- How to get a beach body: take your body to a beach. Voilà. Beach body.
- Remember: the beach is there for your pleasure and entertainment, not the other way around!
- How to be summer-ready: the real question is, will summer be ready for you?
But what is this, demotivational rhetoric to discourage you from getting fit and healthy?
Not at all, but rather, to be sure that you’re pursuing your own goals and not just what you feel might be expected of you.
All that in mind, let’s get to the tips…
Focus on adding health
It can be tempting (and even, good) to cut down on unhealthy things. But when it comes to motivation, it’s harder to stay motivated for deprivation, than it is for some healthy addition to life.
So for example, this philosophy would advocate for:
- Instead of counting calories, count steps! Or even…
- Instead of counting calories, count colors! Eat the rainbow and all that. No, skittles do not count, but eating a variety of naturally different-colored foods will tend to result in adding different nutrients to your diet.
- Instead of cutting out sugar, add fruit! How many per day will you go for? If you don’t eat much fruit as it is, consider making it a goal to have even just one piece of fruit a day, then build up from there. Find fruit you like! If you pick the fruit you want instead of the fruit you think you “should” have, it’s basically a dessert snack.
We’ve recommended it before, and we’ll recommend it again, but if you’re interested in “adding health”, you should definitely check out:
Dr. Greger’s Daily Dozen (checklist, plus app if you want it)
More details: it’s a checklist of 12 things you should try to include in your diet, with a free streak-tracking app, if you want it, all based on the same scientific research as the best-selling book “How Not To Die”.
“Minimum effort!”
Did you see the movie “Deadpool”? The protagonist has a catch-phrase as he goes into battle, saying to himself “Maximum effort!”.
And, that’s all very well and good if your superpower is immediate recovery from pretty much anything, but for the rest of us, sometimes it’s good to hold ourselves to “minimum effort!”.
Sometimes, something worth doing is worth doing just a little a bit. It’s always better than nothing! Even if feels like you gained nothing from it, it’s the foundation of a habit, and the habit will grow and add up. Sometimes it may even take you by surprise…
Don’t feel like doing 20 bodyweight squats? Do literally just one. Make a deal with yourself: do just one, then you can stop if you like. Then after you’ve done one, you might think to yourself “huh, that wasn’t so bad”, and you try out a few more. Maybe after 5 you can feel your blood pumping a bit and you think “you know what, that’s enough for now”, and great, you did 5x as much exercise as you planned! Wonder what you’ll do tomorrow!
(personal note from your writer here: I’ve managed to “just extend this exercise a little bit more than last time” my way into hour-long exercise sessions before now; I started with “just 10 squats” or “just one sun salutation” etc, to get myself out of a no-exercise period that I’d slipped into, and it’s amazing how quickly adding just a little bit to the previous day’s “minimum effort!” adds up to a very respectable daily exercise session)
Wondering what a good, easy, respectable short term goal could be?
Check Out, For Example: The Seven-Minute Workout
(You might have heard of this one before; it’s an incredibly efficient well-optimized short complete workout that requires no special equipment, just a bit of floorspace and a wall—the above app allows for customizations of it per your preferences, but the basic routine is an excellent starting point for most people)
Commit to yourself (and do any self-negotiation up-front)
Really commit, though. No “or I will look silly because I told people I’d do it”, no “or I will donate x amount to charity” etc, just “I will do it and that’s that”. If you find yourself second-guessing yourself or renegotiating with yourself, just shut that down immediately and refuse to consider it.
Note: you should have break-clauses in this contract with yourself, though. For example, “unless I am ill or injured” is a sensible rule to have in advance for most exercise regimes that weren’t undertaken with your illness or injury in mind.
Make a “To-Don’t” list
Much like how addicts are often advised to not try to quit more than one thing at once, we must also be mindful of not taking on too much at once. It can be very tempting to think:
“I will turn my life around, now! I’ll quit alcohol and animal products and sugar and refined grains, and I’ll go for a run each morning, and I’ll do this and that and there, I’ve got it, here is the blueprint for my healthy perfect life from this day forth!”
And, it’s great to have any and all of that as your end goal if you want, but please, pick one or two things at most to start with, focus on those, and when those have become second nature to you and just a normal part of your life, then choose the next thing to work on.
(You can plan out the whole thing in advance if you want! i.e., I’ll do this, then this, then this, but just… make sure that you’ve really got each one down to a matter of comfort and ease before you take up the next one)
In summary:
- Focus on adding health, whatever that looks like to you
- Figure out what “minimum effort!” is for you, and let that be your baseline
- Commit to yourself (and do any self-negotiation up-front, not later)
- Decide what you’re not going to do yet, and stick to that, too.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
- How to get a beach body: take your body to a beach. Voilà. Beach body.
-

Artichoke vs Cabbage – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
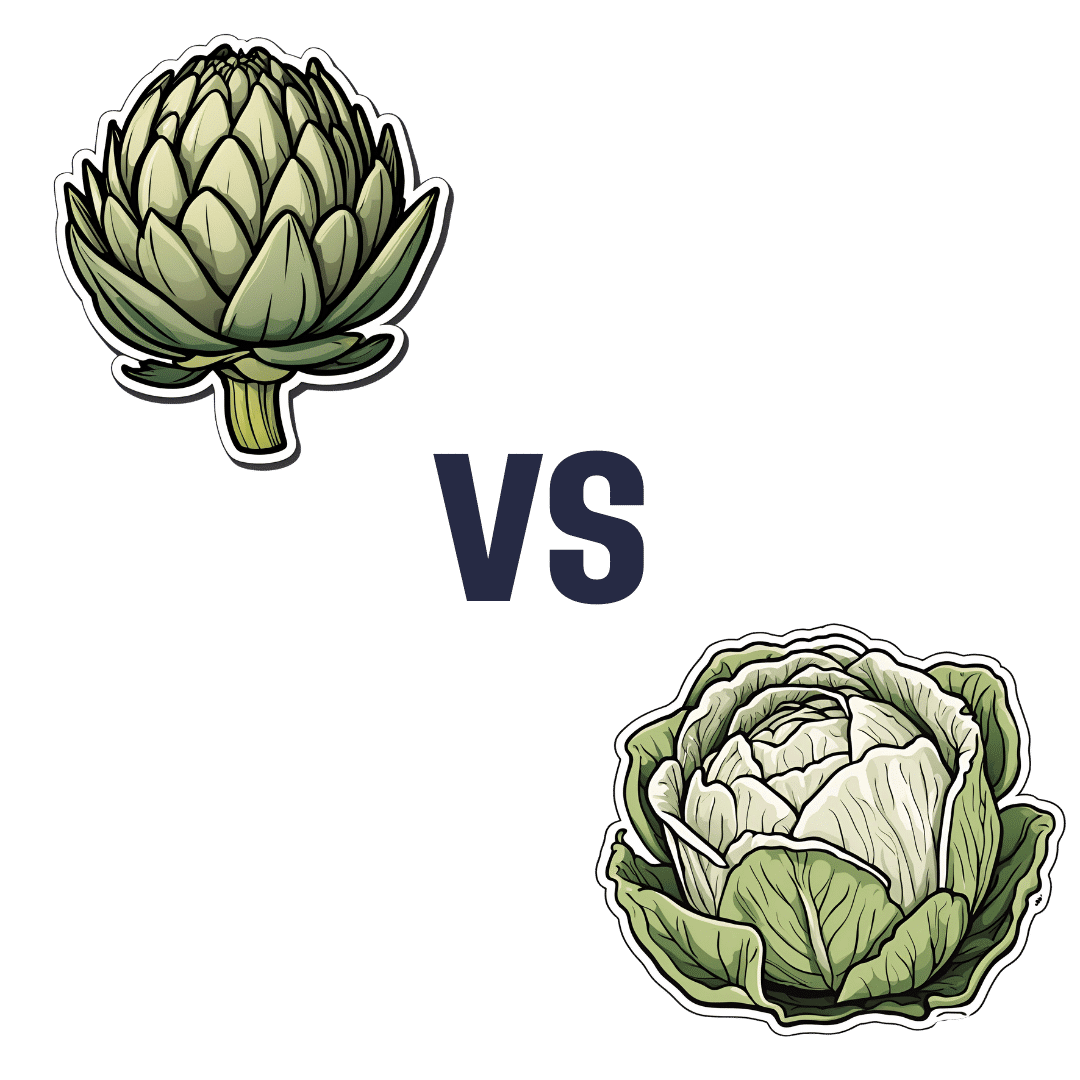
When comparing artichoke to cabbage, we picked the artichoke.
Why?
Looking at the macros first of all, artichoke has more than 2x the protein; it also has nearly 2x the carbs, but to more than counterbalance that, it has more than 2x the fiber. An easy win for artichoke in the macros category.
In the category of vitamins, both are very respectable; artichoke has more of vitamins B1, B2, B3, B5, B9, E, and choline, while cabbage has more of vitamins A, C, and K. Superficially, that’s a 7:3 win for artichoke, but the margins of difference for artichoke’s vitamins are very small (meaning cabbage is hot on its heels for those vitamins), whereas cabbage’s A, C, and K are with big margins of difference (3–7x more), and arguably those vitamins are higher priority in the sense that B-vitamins of various kinds are found in most foods, whereas A, C, and K aren’t, and while E isn’t either, artichoke had a tiny margin of difference for that. All in all, we’re calling this category a tie, as an equally fair argument could be made for either vegetable here.
When it comes to minerals, there’s a much clearer winner: artichoke has a lot more copper, iron, magnesium, manganese, phosphorus, potassium, and zinc, while cabbage has a tiny bit more selenium. The two vegetables are equal on calcium.
Adding up two clear artichoke wins and a tie, makes for an overall clear win for artichoke. Of course, enjoy both though; diversity is almost always best of all!
Want to learn more?
You might like to read:
What’s Your Plant Diversity Score?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Fluoride Toothpaste vs Non-Fluoride Toothpaste – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
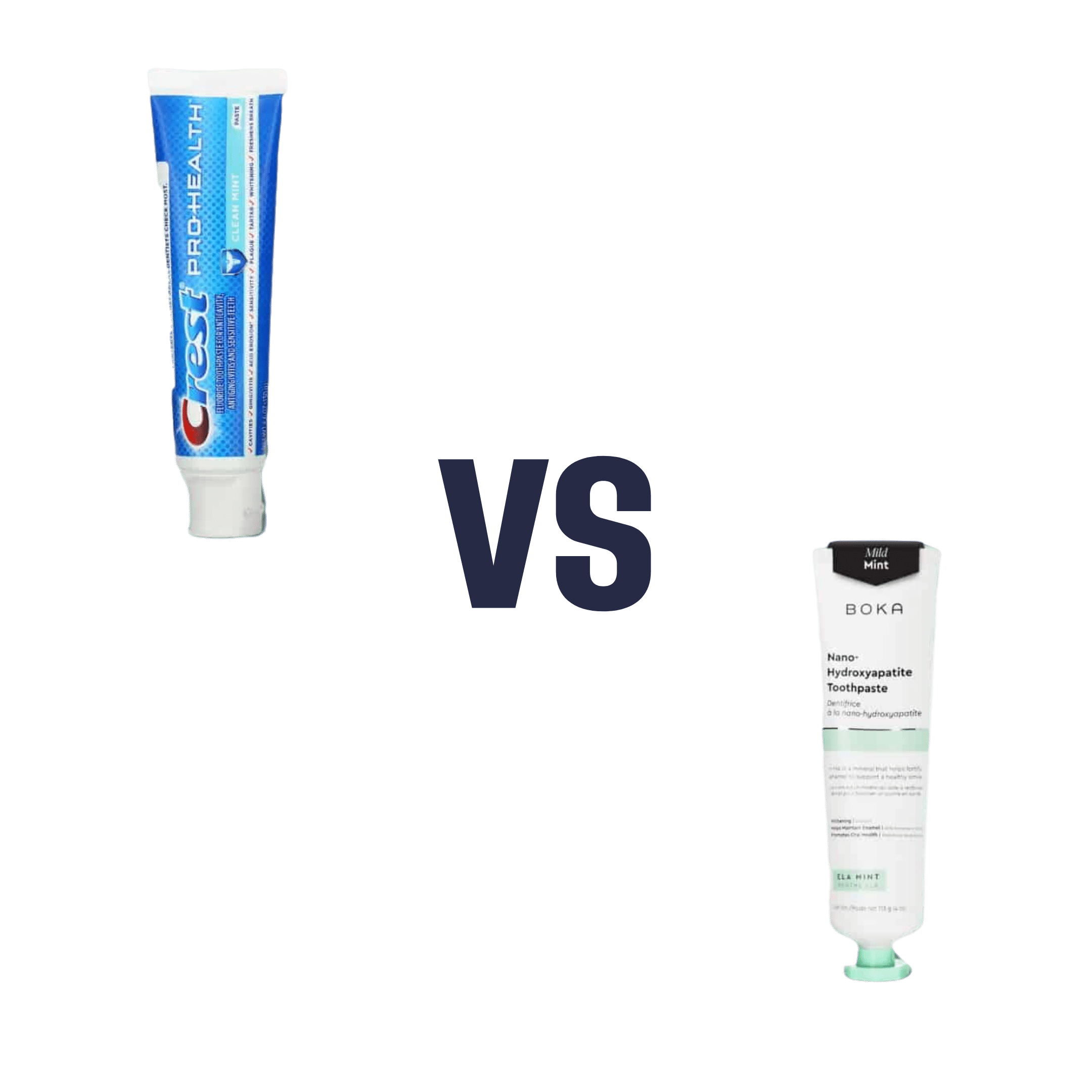
When comparing fluoride toothpaste to non-fluoride toothpaste, we picked the fluoride.
Why?
Fluoride is indeed toxic; that’s why it’s in toothpaste (to kill things; namely, bacteria whose waste products would harm our teeth). However, we are much bigger than those bacteria.
Given the amount of fluoride in toothpaste (usually under 1mg per strip of toothpaste to cover a toothbrush head), the amount that people swallow unintentionally (about 1/20th of that, so about 0.1mg daily if brushing teeth twice daily), and the toxicity level of fluoride (32–64mg/kg), then even if we take the most dangerous ends of all those numbers (and an average body size), to suffer ill effects from fluoride due to brushing your teeth, would require that you brush your teeth more than 23,000 times per day.
Alternatively, if you were to ravenously eat the toothpaste instead of spitting it out, you’d only need to brush your teeth a little over 1,000 times per day.
All the same, please don’t eat toothpaste; that’s not the message here.
However! In head-to-head tests, fluoride toothpaste has almost always beaten non-fluoride toothpaste.
Almost? Yes, almost: hydroxyapatite performed equally in one study, but that’s not usually an option on as many supermarket shelves.
We found some on Amazon, though, which is the one we used for today’s head-to-head. Here it is:
However, before you rush to buy it, do be aware that the toxicity of hydroxyapatite appears to be about twice that of fluoride:
Scientific Committee on Consumer Safety Opinion On Hydroxyapatite (Nano)
…which is still very safe (you’d need to brush your teeth, and eat all the toothpaste, about 500 times per day, to get to toxic levels, if we run with the same numbers we discussed before. Again, please do not do that, though).
But, since the science so far suggests it’s about twice as toxic as fluoride, then regardless of that still being very safe, the fluoride is obviously (by the same metric) twice as safe, hence picking the fluoride.
Want more options?
Check out our previous main feature:
Less Common Oral Hygiene Options
(the above article also links back to our discussion of different toothpastes and mouthwashes, by the way)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: