Carrots vs Red Cabbage – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing carrots to red cabbage, we picked the red cabbage.
Why?
It’s very close!
In terms of macros, these two vegetables are pretty much equal on all metrics. By official numbers, carrots have a tiny bit more fiber and red cabbage has a tiny bit more protein, but realistically, the difference are so small that they’re within the margin of variation (i.e. while we look at official average values, in reality one plant’s figures will differ very slightly from another’s; it could depend on what the soil was like or which plant got more sun, etc). So, a tie here.
In the category of vitamins, carrots have more of vitamins A, B3, B5, and E, while red cabbage has more of vitamins B2, B6, C, K, and choline. So, both have their merits, but red cabbage enjoys a measurable marginal victory here.
Looking at minerals, carrots have more copper, phosphorus, and potassium, while red cabbage has more calcium, iron, magnesium, manganese, and selenium. So, another marginal win for red cabbage here.
When it comes to phytochemicals, they’re about equal on polyphenols and other relevant phytonutrients not otherwise mentioned above.
Adding up the sections makes for a win for red cabbage, but it was close, and carrots are certainly great too. Enjoy either or both; diversity is good!
Want to learn more?
You might like:
What’s Your Plant Diversity Score?
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Navigating the health-care system is not easy, but you’re not alone.

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.

Hello, dear reader!
This is my first column for Healthy Debate as a Patient Navigator. This column will be devoted to providing patients with information to help them through their journey with the health-care system and answering your questions.
Here’s a bit about me: I have been a patient partner at The Ottawa Hospital and Ottawa Hospital Research Institute since 2017, and have joined a variety of governance boards that work on patient and caregiver engagement such as the Patient Advisors Network, the Ontario Health East Region Patient and Family Advisory Council and the Equity in Health Systems Lab.
My journey as a patient partner started much before 2017 though. When I was a teenager, I was diagnosed with a cholesteatoma, a rare and chronic disease that causes the development of fatty tumors in the middle ear. I have had multiple surgeries to try to fix it but will need regular follow-ups to monitor whether the tumor returns. Because of this, I also live with an invisible disability since I have essentially become functionally deaf in one ear and often rely on a hearing aid when I navigate the world.
Having undergone three surgeries in my adolescent years, it was my experience undergoing surgery for an acute hand and wrist injury following a jet ski accident as an adult that was the catalyst for my decision to become a patient partner. There was an intriguing contrast between how I was cared for at two different health-care institutions, my age being the deciding factor at which hospital I went to (a children’s hospital or an adult one).
The most memorable example was how, as a teenager or child, you were never left alone before surgery, and nurses and staff took all the time necessary to comfort me and answer my (and my family’s) questions. I also remember how right before putting me to sleep, the whole staff initiated a surgical pause and introduced themselves and explained to me what their role was during my surgery.
None of that happened as an adult. I was left in a hallway while the operating theater was prepared, anxious and alone with staff walking by not even batting an eye. My questions felt like an annoyance to the care team; as soon as I was wheeled onto the operating room table, the anesthetist quickly put me to sleep. I didn’t even have the time to see who else was there.
Now don’t get me wrong: I am incredibly appreciative with the quality of care I received, but it was the everyday interactions with the care teams that I felt could be improved. And so, while I was recovering from that surgery, I looked for a way to help other patients and the hospital improve its care. I discovered the hospital’s patient engagement program, applied, and the rest is history!
Since then, I have worked on a host of patient-centered policy and research projects and fervently advocate that surgical teams adopt a more compassionate approach with patients before and after surgery.
I’d be happy to talk a bit more about my journey if you ask, but with that out of the way … Welcome to our first patient navigator column about patient engagement.
Conceptualizing the continuum of Patient Engagement
In the context of Canadian health care, patient engagement is a multifaceted concept that involves active collaboration between patients, caregivers, health-care providers and researchers. It involves patients and caregivers as active contributors in decision-making processes, health-care services and medical research. Though the concept is not new, the paradigm shift toward patient engagement in Canada started around 2010.
I like to conceptualize the different levels of patient engagement as a measure of the strength of the relationship between patients and their interlocutors – whether it’s a healthcare provider, administrator or researcher – charted against the duration of the engagement or the scope of input required from the patient.
Defining different levels of Patient Engagement
Following the continuum, let’s begin by defining different levels of patient engagement. Bear in mind that these definitions can vary from one organization to another but are useful in generally labelling the level of patient engagement a project has achieved (or wishes to achieve).
Patient involvement: If the strength of the relationship between patients and their interlocutors is minimal and not time consuming or too onerous, then perhaps it can be categorized as patient involvement. This applies to many instances of transactional engagement.
Patient advisory/consulting: Right in the middle of our continuum, patients can find themselves engaging in patient advisory or consulting work, where projects are limited in scope and duration or complexity, and the relationship is not as profound as a partnership.
Patient partnership: The stronger the relationship is between the patient and their interlocutor, and the longer the engagement activity lasts or how much input the patient is providing, the more this situation can be categorized as patient partnership. It is the inverse of patient involvement.
Examples of the different levels of Patient Engagement
Let’s pretend you are accompanying a loved one to an appointment to manage a kidney disease, requiring them to undergo dialysis treatment. We’ll use this scenario to exemplify what label could be used to describe the level of engagement.
Patient involvement: In our case, if your loved one – or you – fills out a satisfaction or feedback survey about your experience in the waiting room and all that needed to be done was to hand it back to the clerk or care team, then, at a basic level, you could likely label this interaction as a form of patient involvement. It can also involve open consultations around a design of a new look and feel for a hospital, or the understandability of a survey or communications product. Interactions with the care team, administrators or researchers are minimal and often transactional.
Patient advisory/consulting: If your loved one was asked for more detailed information about survey results over the course of a few meetings, this could represent patient advisory/consulting. This could mean that patients meet with program administrators and care providers and share their insights on how things can be improved. It essentially involves patients providing advice to health-care institutions from the perspective of patients, their family members and caregivers.
Patient advisors or consultants are often appointed by hospitals or academic institutions to offer insights at multiple stages of health-care delivery and research. They can help pilot an initiative based on that feedback or evaluate whether the new solutions are working. Often patient advisors are engaged in smaller-term individual projects and meet with the project team as regularly as required.
Patient partnership: Going above and beyond patient advisory, if patients have built a trusting relationship with their care team or administrators, they could feel comfortable enough to partner with them and initiate a project of their own. This could be for a project in which they study a different form of treatment to improve patient-centered outcomes (like the time it takes to feel “normal” following a session); it could be working together to identify and remove barriers for other patients that need to access that type of care. These projects are not fulfilled overnight, but require a collaborative, longstanding and trusting relationship between patients and health-care providers, administrators or researchers. It ensures that patients, regardless of severity or chronicity of their illness, can meaningfully contribute their experiences to aid in improving patient care, or develop or implement policies, pilots or research projects from start to finish.
It is leveraging that lived and living experience to its full extent and having the patient partner involved as an equal voice in the decision-making process for a project – over many months, usually – that the engagement could be labeled a partnership.
Last words
The point of this column will be to answer or explore issues or questions related to patient engagement, health communications or even provide some thoughts on how to handle a particular situation.
I would be happy to collect your questions and feedback at any time, which will help inform future columns. Just email me at [email protected] or connect with me on social media (Linked In, X / Twitter).
It’s not easy to navigate our health-care systems, but you are not alone.
This article is republished from healthydebate under a Creative Commons license. Read the original article.
Share This Post
-

Hormones & Health, Beyond The Obvious
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Wholesome Health
This is Dr. Sara Gottfried, who some decades ago got her MD from Harvard and specialized as an OB/GYN at MIT. She’s since then spent the more recent part of her career educating people (mostly: women) about hormonal health, precision, functional, & integrative medicine, and the importance of lifestyle medicine in general.
What does she want us to know?
Beyond “bikini zone health”
Dr. Gottfried urges us to pay attention to our whole health, in context.
“Women’s health” is often thought of as what lies beneath a bikini, and if it’s not in those places, then we can basically treat a woman like a man.
And that’s often not actually true—because hormones affect every living cell in our body, and as a result, while prepubescent girls and postmenopausal women (specifically, those who are not on HRT) may share a few more similarities with boys and men of similar respective ages, for most people at most ages, men and women are by default quite different metabolically—which is what counts for a lot of diseases! And note, that difference is not just “faster” or “slower””, but is often very different in manner also.
That’s why, even in cases where incidence of disease is approximately similar in men and women when other factors are controlled for (age, lifestyle, medical history, etc), the disease course and response to treatment may vary considerable. For a strong example of this, see for example:
- The well-known: Heart Attack: His & Hers ← most people know these differences exist, but it’s always good to brush up on what they actually are
- The less-known: Statins: His & Hers ← most people don’t know these differences exist, and it pays to know, especially if you are a woman or care about one
Nor are brains exempt from his…
The female brain (kinda)
While the notion of an anatomically different brain for men and women has long since been thrown out as unscientific phrenology, and the idea of a genetically different brain is… Well, it’s an unreliable indicator, because technically the cells will have DNA and that DNA will usually (but not always; there are other options) have XX or XY chromosomes, which will usually (but again, not always) match apparent sex (in about 1/2000 cases there’s a mismatch, which is more common than, say, red hair; sometimes people find out about a chromosomal mismatch only later in life when getting a DNA test for some unrelated reason), and in any case, even for most of us, the chromosomal differences don’t count for much outside of antenatal development (telling the default genital materials which genitals to develop into, though this too can get diverted, per many intersex possibilities, which is also a lot more common than people think) or chromosome-specific conditions like colorblindness…
The notion of a hormonally different brain is, in contrast to all of the above, a reliable and easily verifiable thing.
See for example:
Alzheimer’s Sex Differences May Not Be What They Appear
Dr. Gottfried urges us to take the above seriously!
Because, if women get Alzheimer’s much more commonly than men, and the disease progresses much more quickly in women than men, but that’s based on postmenopausal women not on HRT, then that’s saying “Women, without women’s usual hormones, don’t do so well as men with men’s usual hormones”.
She does, by the way, advocate for bioidentical HRT for menopausal women, unless contraindicated for some important reason that your doctor/endocrinologist knows about. See also:
Menopausal HRT: A Tale Of Two Approaches (Bioidentical vs Animal)
The other very relevant hormone
…that Dr. Gottfried wants us to pay attention to is insulin.
Or rather, its scrubbing enzyme, the prosaically-named “insulin-degrading enzyme”, but it doesn’t only scrub insulin. It also scrubs amyloid beta—yes, the same that produces the amyloid beta plaques in the brain associated with Alzheimer’s. And, there’s only so much insulin-degrading enzyme to go around, and if it’s all busy breaking down excess insulin, there’s not enough left to do the other job too, and thus can’t break down amyloid beta.
In other words: to fight neurodegeneration, keep your blood sugars healthy.
This may actually work by multiple mechanisms besides the amyloid hypothesis, by the way:
The Surprising Link Between Type 2 Diabetes & Alzheimer’s
Want more from Dr. Gottfried?
You might like this interview with Dr. Gottfried by Dr. Benson at the IMCJ:
Integrative Medicine: A Clinician’s Journal | Conversations with Sara Gottfried, MD
…in which she discusses some of the things we talked about today, and also about her shift from a pharmaceutical-heavy approach to a predominantly lifestyle medicine approach.
Enjoy!
Share This Post
-

Dr. Stacy Sims’ Guide to Fitness and Nutrition after 40
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s worth noting that Dr. Sims has directed research programs at Stanford University focusing on female athlete health and performance, and she also has 94 peer-reviewed papers on the topic to her name.
Here’s what she has to say for those of us in the “women over 40” bracket:
What most people miss
Some notes on daily rhythm: Dr. Sims recommends to eat within an hour of waking, because cortisol spikes about 30 minutes afterwards, so, we can counter it with breakfast. She also advises we bookend our workouts with food, especially 30–40g of protein afterwards. Eat regularly through the day, have an adequate dinner, and avoid eating after dinner, to work with normal hormonal fluctuations.
You may be thinking “but I have long since menopaused; I do not have hormonal fluctuations”; in such a case, then do remember that “hormonal” doesn’t just mean sex hormones, it also means cortisol, serotonin, dopamine, leptin, ghrelin, insulin, and many others!
About heavy lifting after 40: declining estrogen changes muscle signalling, so women must rely more on central-nervous-system stimulation. Heavy loads create this stimulus, improving strength, power, lean mass, and nerve firing when hormonal signalling is reduced. So, lift heavy! But, also safely, please.
Some specific notes on high-intensity interval training (HIIT) of various kinds:
- SIT (sprint interval training): very short maximal bursts of 30 seconds or less at perceived exertion 9–10, followed by long recovery. effective for metabolic control and for signalling between skeletal muscle, the liver, and visceral fat. two intervals are usually the maximum for beginners if the effort is truly maximal.
- High-intensity training in general: true high intensity (e.g. 1–4 minute efforts at 80–90% of maximum heartrate with equal recovery) generates hormones that help lower cortisol afterwards. Moderate intensity does not create the same adaptive hormonal response.
On bone density, she recommends:
- Don’t bother with weighted vests for walking: wearing a weighted vest while walking can maintain existing bone but does not stimulate new growth. Basically, it doesn’t improve bone density because it lacks multi-directional stress, which is what’s needed per Wolff’s Law.
- Do use multi-directional jumps: for example, flat-footed pogo stick jumps or jumping rope, for about 10 minutes, three times per week. The “bone jump” app (developed from a 5-year study in 35–45-year-old women with low-normal bone density) provides structured jump progressions.
Two biggest things she wants us all to take into account, if we remember nothing else:
- Address sleep before fine-tuning training. Better sleep improves cravings, gut health, training response, and stress regulation.
- Ignore diet fads and instead focus on meal timing, consistent intake, and sufficient protein. Match your nutrition to your stress levels and training.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Next Level – by Dr. Stacy Sims ← this is her book specifically about going from strength to strength through menopause and beyond 😎
Take care!
Share This Post



Related Posts
-

Quit Drinking – by Rebecca Dolton
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Many “quit drinking” books focus on tips you’ve heard already—cut down like this, rearrange your habits like that, make yourself accountable like so, add a reward element this way, etc.
Dolton takes a different approach.
She focuses instead on the underlying processes of addiction, so as to not merely understand them to fight them, but also to use them against the addiction itself.
This is not just a social or behavioral analysis, by the way, and goes into some detail into the physiological factors of the addiction—including such things as the little-talked about relationship between addiction and gut flora. Candida albans, found in most if not all humans to some extent, gets really out of control when given certain kinds of sugars (including those from alcohol); it grows, eventually puts roots through the intestinal walls (ouch!) and the more it grows, the more it demands the sugars it craves, so the more you feed it.
Quite a motivator to not listen to such cravings! It’s not even you that wants it, it’s the Candida!
Anyway, that’s just one example; there are many. The point here is that this is a well-researched, well-written book that sets itself apart from many of its genre.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

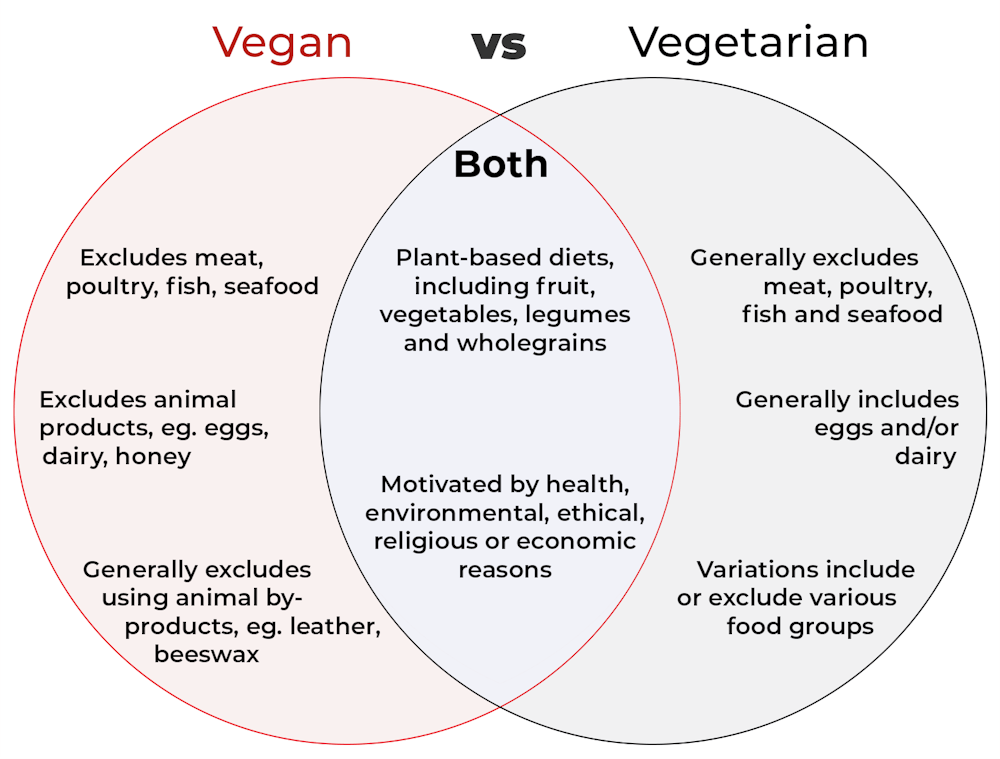
What’s the difference between vegan and vegetarian?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What’s the difference? is a new editorial product that explains the similarities and differences between commonly confused health and medical terms, and why they matter.
Vegan and vegetarian diets are plant-based diets. Both include plant foods, such as fruits, vegetables, legumes and whole grains.
But there are important differences, and knowing what you can and can’t eat when it comes to a vegan and vegetarian diet can be confusing.
So, what’s the main difference?
Creative Cat Studio/Shutterstock What’s a vegan diet?
A vegan diet is an entirely plant-based diet. It doesn’t include any meat and animal products. So, no meat, poultry, fish, seafood, eggs, dairy or honey.
What’s a vegetarian diet?
A vegetarian diet is a plant-based diet that generally excludes meat, poultry, fish and seafood, but can include animal products. So, unlike a vegan diet, a vegetarian diet can include eggs, dairy and honey.
But you may be wondering why you’ve heard of vegetarians who eat fish, vegetarians who don’t eat eggs, vegetarians who don’t eat dairy, and even vegetarians who eat some meat. Well, it’s because there are variations on a vegetarian diet:
- a lacto-ovo vegetarian diet excludes meat, poultry, fish and seafood, but includes eggs, dairy and honey
- an ovo-vegetarian diet excludes meat, poultry, fish, seafood and dairy, but includes eggs and honey
- a lacto-vegetarian diet excludes meat, poultry, fish, seafood and eggs, but includes dairy and honey
- a pescatarian diet excludes meat and poultry, but includes eggs, dairy, honey, fish and seafood
- a flexitarian, or semi-vegetarian diet, includes eggs, dairy and honey and may include small amounts of meat, poultry, fish and seafood.
Are these diets healthy?
A 2023 review looked at the health effects of vegetarian and vegan diets from two types of study.
Observational studies followed people over the years to see how their diets were linked to their health. In these studies, eating a vegetarian diet was associated with a lower risk of developing cardiovascular disease (such as heart disease or a stroke), diabetes, hypertension (high blood pressure), dementia and cancer.
For example, in a study of 44,561 participants, the risk of heart disease was 32% lower in vegetarians than non-vegetarians after an average follow-up of nearly 12 years.
Further evidence came from randomised controlled trials. These instruct study participants to eat a specific diet for a specific period of time and monitor their health throughout. These studies showed eating a vegetarian or vegan diet led to reductions in weight, blood pressure, and levels of unhealthy cholesterol.
For example, one analysis combined data from seven randomised controlled trials. This so-called meta-analysis included data from 311 participants. It showed eating a vegetarian diet was associated with a systolic blood pressure (the first number in your blood pressure reading) an average 5 mmHg lower compared with non-vegetarian diets.
It seems vegetarian diets are more likely to be healthier, across a number of measures.
For example, a 2022 meta-analysis combined the results of several observational studies. It concluded a vegetarian diet, rather than vegan diet, was recommended to prevent heart disease.
There is also evidence vegans are more likely to have bone fractures than vegetarians. This could be partly due to a lower body-mass index and a lower intake of nutrients such as calcium, vitamin D and protein.
But it can be about more than just food
Many vegans, where possible, do not use products that directly or indirectly involve using animals.
So vegans would not wear leather, wool or silk clothing, for example. And they would not use soaps or candles made from beeswax, or use products tested on animals.
The motivation for following a vegan or vegetarian diet can vary from person to person. Common motivations include health, environmental, ethical, religious or economic reasons.
And for many people who follow a vegan or vegetarian diet, this forms a central part of their identity.
More than a diet: veganism can form part of someone’s identity. Shutterstock So, should I adopt a vegan or vegetarian diet?
If you are thinking about a vegan or vegetarian diet, here are some things to consider:
- eating more plant foods does not automatically mean you are eating a healthier diet. Hot chips, biscuits and soft drinks can all be vegan or vegetarian foods. And many plant-based alternatives, such as plant-based sausages, can be high in added salt
- meeting the nutrient intake targets for vitamin B12, iron, calcium, and iodine requires more careful planning while on a vegan or vegetarian diet. This is because meat, seafood and animal products are good sources of these vitamins and minerals
- eating a plant-based diet doesn’t necessarily mean excluding all meat and animal products. A healthy flexitarian diet prioritises eating more whole plant-foods, such as vegetables and beans, and less processed meat, such as bacon and sausages
- the Australian Dietary Guidelines recommend eating a wide variety of foods from the five food groups (fruit, vegetables, cereals, lean meat and/or their alternatives and reduced-fat dairy products and/or their alternatives). So if you are eating animal products, choose lean, reduced-fat meats and dairy products and limit processed meats.
Katherine Livingstone, NHMRC Emerging Leadership Fellow and Senior Research Fellow at the Institute for Physical Activity and Nutrition, Deakin University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Kombucha vs Kimchi – Which is Healthier
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing kombucha to kimchi, we picked the kombucha.
Why?
While both are very respectable gut-healthy fermented products,
• the kombucha contains fermented tea, a little apple cider vinegar, and a little fiber
• the kimchi contains (after the vegetables) 810 mg sodium in that little tin, and despite the vegetables, no fiber.You may reasonably be surprised that they managed to take something that is made of mostly vegetables and ended up with no fiber without juicing it, but they did. Fermented vegetables are great for the healthy bacteria benefits (and are tasty too!), but the osmotic pressure due to the salt destroys the cell walls and thus the fiber.
Thus, we chose the kombucha that does the same job without delivering all that salt.
However! If you are comparing kombucha and kimchi out in the wilds of your local supermarket, do still check individual labels. It’s not uncommon, for example, for stores to sell pre-made kombucha that’s loaded with sugar.
About sugar and kombucha…
Sugar is required to make kombucha, to feed the yeast and helpful bacteria. However, there should be none of that sugar left (or only the tiniest trace amount) in the final product, because the yeast (and friends) consumed and metabolized it.
What some store brands do, however, is add in sugar afterwards, as they believe it improves the taste. This writer cannot imagine how, but that is their rationale in any case. Needless to say, it is not a healthy addition, and specifically, it’s bad for your gut, which (healthwise) is the whole point of drinking kombucha in the first place.
Want some? Here is an example product on Amazon, but feel free to shop around as there are many flavors available!
Read more about gut health: Gut Health 101
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: