Can High-Volume Exercise Be Bad For Your Heart? It Depends On Your Sex
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Endurance exercise has often been questioned for its potential to increase heart attack risk, a large (n=61,150) comprehensive (a meta-analysis of studies) research has shown, in a nutshell:
- In men, high-volume endurance exercise is associated with higher coronary artery calcium (CAC) scores (that’s bad) and higher calcified plaque volume (also bad) compared to non-athlete men.
- In women, however, no such increase was found (for CAC or plaque) regardless of exercise volume.
In fact, high-volume female athletes* had less calcified plaque than non-athlete women.
*as in, the exercise was high volume; the volume of the athletes themselves was not mentioned!
You may be wondering: does this mean that men should skip the exercise?
And the answer is: no, because moderate exercise was linked to lower calcified plaque volume in men and women.
As to what “high-volume”, “moderate”, and “non-athletes” mean, for the purposes of the study:
- High: >3,000 MET-minutes/week
- Moderate: 1,500–3,000 MET-minutes/week
- Non-athletes: <1,500 MET-minutes/week
MET = Metabolic Equivalent of Task, i.e. the number your phone exercise tracker app shows, whereby if you exercise for 1 minute with your heart above a certain percentage of its maximum, the tracker records it as 2 minutes, because it is the metabolic equivalent of 2 minutes at the lower heart rate.
Thus, in terms of practical advice: the researchers make clear that they don’t want to discourage exercise ,but to support comprehensive risk assessment, especially in men doing high-volume exercise.
You can read the paper in full here: Sex Differences in the Impact of Exercise Volume on Subclinical Coronary Atherosclerosis: A Meta-Analysis
“I’m a woman without a man in my life, so is this irrelevant to me?”
It might be, or it might not be! The question the researchers didn’t ask is: what’s the current state of your hormones?
Because, in this paper…
Let’s do a quick tally of how many times certain words are mentioned (bearing in mind that the paper is about sex differences, and is 8,301 words long):
- Hormone: 1
- Testosterone: 1
- Estrogen: 0
- Menopause: 0
- HRT: 0
Do you see the problem? An entire paper about sex differences, and we’re still getting medically sidelined.
And, this is likely important, because hormones make a huge difference to heart health; see for example:
- What Menopause Does To The Heart
- Hormones & Health, Beyond The Obvious
- His & Hers? The Hidden Complexities of Statins and Cardiovascular Disease (CVD)
What this means: it is likely, but not known for sure, that sex hormone differences are what affect the coronary artery calcium and calcified plaque scores so drastically as seen in the study.
In practical terms: if you are a woman who is post-menopause and not on hormone replacement therapy (HRT), you could well have higher risk factors in this case.
Want to learn more?
If you’re curious about the current state of your arteries, then please do book a professional test, but meanwhile:
Try This At Home: ABI Test For Clogged Arteries
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Fat’s Real Barriers To Health

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Fat Justice In Healthcare

This is Aubrey Gordon, an author, podcaster, and fat justice activist. What does that mean?
When it comes to healthcare, we previously covered some ideas very similar to her work, such as how…
There’s a lot of discrimination in healthcare settings
In this case, it often happens that a thin person goes in with a medical problem and gets treated for that, while a fat person can go in with the same medical problem and be told “you should try losing some weight”.
Top tip if this happens to you… Ask: “what would you advise/prescribe to a thin person with my same symptoms?”
Other things may be more systemic, for example:
When a thin person goes to get their blood pressure taken, and that goes smoothly, while a fat person goes to get their blood pressure taken, and there’s not a blood pressure cuff to fit them, is the problem the size of the person or the size of the cuff? It all depends on perspective, in a world built around thin people.
That’s a trivial-seeming example, but the same principle has far-reaching (and harmful) implications in healthcare in general, e.g:
- Surgeons being untrained (and/or unwilling) to operate on fat people
- Getting a one-size-fits-all dose that was calculated using average weight, and now doesn’t work
- MRI machines are famously claustrophobia-inducing for thin people; now try not fitting in it in the first place
…and so forth. So oftentimes, obesity will be correlated with a poor healthcare outcome, where the problem is not actually the obesity itself, but rather the system having been set up with thin people in mind.
It would be like saying “Having O- blood type results in higher risks when receiving blood transfusions”, while omitting to add “…because we didn’t stock O- blood”.
Read more on this topic: Shedding Some Obesity Myths
Does she have practical advice about this?
If she could have you understand one thing, it would be:
You deserve better.
Or if you are not fat: your fat friends deserve better.
How this becomes useful is: do not accept being treated as the problem!
Demand better!
If you meekly accept that you “just need to lose weight” and that thus you are the problem, you take away any responsibility from your healthcare provider(s) to actually do their jobs and provide healthcare.
See also Gordon’s book, which we’ve reviewed:
“You Just Need to Lose Weight”: And 19 Other Myths About Fat People – by Aubrey Gordon
Are you saying fat people don’t need to lose weight?
That’s a little like asking “would you say office workers don’t need to exercise more?”; there are implicit assumptions built into the question that are going unaddressed.
Rather: some people might benefit healthwise from losing weight, some might not.
In fact, over the age of 65, being what is nominally considered “overweight” reduces all-cause mortality risk.
For details of that and more, see: When BMI Doesn’t Measure Up
But what if I do want/need to lose weight?
Gordon’s not interested in helping with that, but we at 10almonds are, so…
Check out: Lose Weight, But Healthily
Where can I find more from Aubrey Gordon?
You might enjoy her blog:
Aubrey Gordon | Your Fat Friend
Or her other book:
What We Don’t Talk About When We Talk About Fat – by Aubrey Gordon
Enjoy!
Share This Post
-

Why You’re Tired & How To Fix It
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This is Sadia Badiei. A dietician by academic and professional background, she’s nowadays hung up her lab coat for a chef’s jacket, and is best known for her “Pick Up Limes” brand. Today, we’ll be taking her advice on managing energy levels with what’s on our plates!
Quick note: our usual medical/legal disclaimer applies, and this article cannot diagnose you from afar, and thus neither can it make any certain prescription; this is for educational purposes, and aimed at being applicable to most of our readers.
There are many possible things that can cause chronic fatigue, and not all of them can be fixed by diet. Your doctor will have access to tests and such that we, being a humble health science publication, do not.
You may recognize her; we’ve featured her videos occasionally, mostly recently:
Pick Up A Zest For Life: 10 Lessons For A Healthy Mind & Body
But, what does she want us to know about living life with more energy?
It starts with balance
Badiei makes the case that we should strive for a nutritionally-balanced diet; that may not come as much of a revelation, but what does that look like for a vegan (Badiei advocates for plant-based eating)?
She recommends that our diet consist of:
- About 50% fruits and vegetables
- About 25% grains and starches
- About 25% proteins
- Modest amounts of fats
- A little of well-chosen dairy substitutions
- Finally, a few judicious supplements to top it off
That does add up to more than 100%, but 1) we did say “About n%” and 2) this is not a bad thing to note, actually, since Badiei advocates (as we do) for focussing more on what we add into our diet, rather than what we take out.
Breaking it down a little further, she recommends making sure to get “the foundational seven”, which is a little like “Dr. Greger’s Daily Dozen”, but in this case it’s counted on a per-food-type basis.
Thus, she recommends:
- Dark green leafy vegetables
- Assorted other non-starchy vegetables (your choice what kind)
- Fruit, of any kinds (unlike Dr. Greger separating berries)
- Grains and starches (so for example, potatoes are lumped in with rice here, botanically very different, but often fulfil a similar culinary role)
- Nuts and seeds
- Legumes
- Fortified dairy alternatives
For full details including how much of each, and “what counts”, etc, see:
Pick Up Limes | The Nourish Method
Time your carbs
Slow-release carbohydrates, those with the most fiber, are best most of the time, giving us more sustained fuel, keeping us energized for longer after meals—even if we would rather sleep:
She cites: Fiber and Saturated Fat Are Associated with Sleep Arousals and Slow Wave Sleep
Quick-release carbohydrates, those with what’s generally considered a less favorable carb:fiber ratio, are best if we’re going to eat nearer to bedtime. We know, eating before bed is often considered a bit of a no-no, but Badiei bids us indulge if we so desire, as the quicker-absorbed carbohydrates support tryptophan reaching our brain more efficiently, and thus promote sleep onset.
See also: Should You Go Light Or Heavy On Carbs?
About that fat
We mentioned (or rather, Badiei’s citation mentioned) saturated fat. It is indeed linked with difficulty falling asleep, and/but omega-3 fatty acids, on the other hand, promote better sleep.
She cites: The relationship between sleep duration, sleep quality and dietary intake in adults
While you’re enjoying those nuts and seeds (for the omega-3 fatty acids), you might also note that several also star in Badiei’s list of plant-based foods that are rich in tryptophan, such as soy, cashews, pumpkin seeds, sunflower seeds, beans, green vegetables, and mushrooms.
Micronutrients
Badiei’s focus here is on B-vitamins, iron, magnesium, selenium, and zinc. We imagine most of our readers here are taking steps to ensure to get a full daily coverage of vitamins and minerals anyway, but you might want to read what she has to say about iron on a plant-based diet, because the numbers may be different than you think.
The reason for this is that while animal products contain mostly heme iron, which is easier to absorb but associated with a risk increase in some diseases, plant-based foods usually* contain only non-heme iron, which is healthier but not as bioavailable, so if eating only plants, we need more of it:
Pick Up Limes | Iron on a Plant-Based Diet
*If you eat a carnivorous plant, guess what, it’ll have heme iron in it, tangling that food web.
“What if I know I have chronic fatigue for non-dietary reasons?”
Well, that sucks, and we’re not going to pretend the above will magically fix it. However, there are still things that can at least relatively improve your experience:
Eat To Beat Chronic Fatigue! Yes, Even When Fatigued Chronically
(it’s a good guide to being able to consistently eat healthily when your energy levels are consistently at minimal, meaning that a lot of common advice becomes unusable)
Take care!
Share This Post
-
Should I kick my diet soft-drink habit? Where do I start?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The average Australian drinks almost 60 litres of soft drink a year. Many people see diet soft drinks as a “healthier” choice than regular ones, and when it comes to sugar, that’s true.
For example, a 375 millilitre can of Coca-Cola contains about seven teaspoons of added sugar (almost to 40 grams). That’s close to the World Health Organization’s (WHO) daily recommended limit for added sugars of 50g.
In comparison, the Diet Coke version is sweetened with artificial sweeteners such as aspartame and does not contain sugar.
So if you reach for diet soft drinks, is that so bad? Or is it worth giving them up too?

Towfiqu barbhuiya/Pexels Are diet soft drinks really that bad?
Diet soft drinks provide few nutrients. They often contain artificial sweeteners and caffeine, and while they’re low in energy (kilojoules), they aren’t filling.
People who regularly drink diet soft drinks may have a higher risk of developing conditions such as heart disease and type 2 diabetes.
But this doesn’t necessarily mean the drinks cause these conditions. People who already have health concerns or are trying to manage their weight may be more likely to choose diet drinks, which might make this evidence a little misleading.
How about artificial sweeteners?
In 2023, the WHO classified aspartame (a common sweetener found in many diet soft drinks) as “possibly carcinogenic to humans”. This means the evidence linking aspartame to cancer is currently limited and not conclusive.
The WHO also emphasised that the public generally consumes safe levels of aspartame and only has evidence for concern if people drink the equivalent to 14 cans of soft drink a day.
There is also emerging evidence some artificial sweeteners might irritate the gut or alter the balance of gut bacteria. These effects are still being investigated. But they’ve added to concerns about the health impacts of drinking diet soft drinks over a long period of time.
Can I get used to the sweetness?
An occasional diet drink isn’t likely to fuel an addiction to sweet foods, but cutting back is still a good idea if this has become a daily habit.
After people cut back on very sweet foods or drinks, some research suggests they start noticing sweetness more easily and find very sweet things taste too sweet.
So if you’re trying to enjoy less-sweet drinks, give it time. Within a few weeks you might actually prefer the less-sweet taste.
Here are three evidence-based strategies to help you adjust.
1. Water it down
A gentle first step is to dilute your soft drink. Start by pouring less soft drink into a glass and topping it up with water or soda water, then gradually adjust the ratio over time.
It may taste less sweet at first, but your taste buds will adapt. This slow, steady approach can make change feel easier and more sustainable than quitting abruptly.
2. Make smarter swaps
Try replacing diet soft drink with a healthier alternative that still delivers flavour or fizz. Sparkling water or soda water with a squeeze of lime or lemon and a few mint leaves gives you the same bubbly refreshment with a natural and refreshing flavour. Add ice if it is a hot day, or to provide some crunch.
If you prefer plain water but it feels boring, infuse it with slices of fruit, cucumber, berries or herbs.
You could also try unsweetened iced tea, such as black, green or herbal tea. These offer a mild caffeine lift without the added sweeteners and can be served cold with ice and lemon.
Coconut water can also be a healthier alternative as it is low in sugar while providing some additional electrolytes, which help balance fluid in the body.
3. Know your triggers
If you often reach for a soft drink out of habit, boredom or an afternoon energy slump, paying attention to these moments can help. Once you spot your triggers, you can plan a different response. Take a short walk, call a friend or make a cup of tea instead.
Keeping a chilled, reusable water bottle nearby also helps. If your drink is always within reach, you’re less likely to grab a diet soft drink when you’re out and about.
If you drink diet soft drinks because you’re hungry, reach for something nourishing instead, such as a handful of nuts, a yoghurt or a piece of fruit. These foods will satisfy you for longer than a can of diet soft drink because they have nutrients, such as fibre, to keep you fuller for longer.
The bottom line
You don’t have to give up diet soft drinks altogether. But being mindful of how much soft drink you drink, and how often, can help you make choices that better support your long-term health.
Start small, be consistent and let your taste buds adjust. Over time, you might find what once tasted “flat” now feels refreshingly natural.
Lauren Ball, Professor of Community Health and Wellbeing, The University of Queensland; Emily Burch, Accredited Practising Dietitian and Lecturer, Southern Cross University, and Mackenzie Derry, Nutritionist, Dietitian & PhD Candidate, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post



Related Posts
-
Ozempic and other weight-loss drugs linked to rare but serious eye conditions
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Drugs such as Ozempic, Wegovy and Mounjaro (known as semaglutide and tirzepatide) have changed the way clinicians manage diabetes and obesity around the world.
Collectively known as GLP-1 agonists, these drugs mimic the hormone GLP-1. This limits both hunger and interest in food, helping users lose weight, and helps control blood sugar levels.
But two new studies published today show that people taking these drugs may have a small increased risk of serious eye conditions and vision loss.
Here’s what you need to know if you’re taking or considering these medications.
What damage can occur?
Non-arteritic anterior ischaemic optic neuropathy, or NAION, is a rare but devastating eye condition that occurs when blood flow to the optic nerve is suddenly reduced or blocked. It’s also called an “eye stroke”.
The exact cause of NAION remains unclear and there are no current treatments available. People with diabetes are at increased risk of developing NAION.
Unlike other eye conditions that develop gradually, NAION causes a sudden, painless loss of vision. Patients typically notice the condition when they wake up and discover they’ve lost vision in one eye.
Vision tends to worsen over a couple of weeks and slowly stabilises. Recovery of vision is variable, but around 70% of people do not experience improvement in their vision.
What has previous research shown?
A previous study from 2024 found participants prescribed semaglutide for diabetes were four times more likely to develop NAION. For those taking it for weight loss, the risk was almost eight times higher.
In June, the European Medicines Agency concluded NAION represented a “very rare” side effect of semaglutide medications: a one in 10,000 chance. In a first for medicines regulators, the agency now requires product labels to include NAION as a documented risk.
However the recent studies suggest the risks may be lower than we first thought.
In addition to NAION, there is also evidence to suggest GLP-1 drugs can worsen diabetic eye disease, also known as diabetic retinopathy. This occurs when high blood sugar levels damage the small blood vessels in the retina, which can lead to vision loss.
It may sound counter-intuitive, but rapid blood sugar reductions can also destabilise the fragile blood vessels in the retina and lead to bleeding.
What do the new studies say?
Two newly published studies investigated people with type 2 diabetes living in the United States over two years. The studies looked at the medical records of 159,000 to 185,000 people.
One study found semaglutide or tirzepatide was associated with a more modest risk of developing NAION than previously thought. Of 159,000 people with type 2 diabetes who were taking these drugs, 35 people (0.04%) developed NAION, compared with 19 patients (0.02%) in the comparison group.
The researchers also found an increased risk of developing “other optic nerve disorders”. However, it’s unclear what kind of optic nerve disorders this includes, as the medical record codes used didn’t specify.
Counter to this, the second study did not find an increased risk of NAION among those taking GLP-1 drugs.
However, the researchers found a small increase in the number of people developing diabetic retinopathy in those prescribed GLP-1 drugs.
But overall, participants on GLP-1 drugs experienced fewer sight-threatening complications related to their diabetic retinopathy and required less invasive eye treatments compared to the group taking other diabetes medications.
Further studies are still needed to understand how GLP-1 drugs can lead to eye complications. A current, five-year clinical trial is studying the long-term effects of semaglutides and diabetic eye disease in 1,500 people, which should tell us more about the ocular risks in the future.
What does this mean for people taking GLP-1 drugs?
NAION is a serious condition. But we need to strike a balance between these (and other) risks and the benefits of GLP-1 medications in diabetes care, obesity treatment, reducing heart attack risks and extending lives.
The key lies in informed decision-making and identifying different levels of risk.
People with multiple NAION risk factors – such as sleep apnoea, high blood pressure and diabetes – should undergo careful consideration with their treating doctor before starting these medications.
“Crowded” optic nerve heads are also a risk factor for NAION. This is an anatomical feature where blood vessels at the optic nerve head are tightly packed together. People with crowded optic nerve heads should also undergo careful consideration before starting GLP-1 medications.
Although NAION can strike without warning, regular comprehensive eye examinations with your optometrist or ophthalmologist still serve important purposes. They can detect other drug-related eye problems, including worsening diabetic retinopathy, and can identify patients with crowded optic nerve heads. It’s also important to tell them if you are taking GLP-1 medications so they can keep a close watch on your eye health.
Emerging research also suggests that improving your heart health might help reduce risks of developing NAION. This includes proper management of high blood pressure, diabetes and cholesterol – all conditions that compromise the small blood vessels feeding the optic nerve.
Studies also show patients with heart conditions who better adhere to their medication prescriptions have lower risks of NAION than those who don’t.
Doctors should discuss NAION risks during prescribing decisions and work with eye care providers to monitor regularly for diabetic eye disease. Patients need clear instructions to seek immediate medical attention for sudden vision loss and the need for regular eye examinations.
Aggressive treatment of sleep apnoea and other heart conditions may also help reduce NAION risks. But for now, there remains an ongoing need for more research to understand how GLP-1 medications can affect the eye.
Flora Hui, Research Fellow, Centre for Eye Research Australia and Honorary Fellow, Department of Surgery (Ophthalmology), The University of Melbourne and Pete A Williams, Ulla and Ingemar Dahlberg Professor in Vision Science, Research Group Leader, Karolinska Institutet
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Ayurveda’s Contributions To Science
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Ayurveda’s Contributions To Science (Without Being Itself Rooted in Scientific Method)

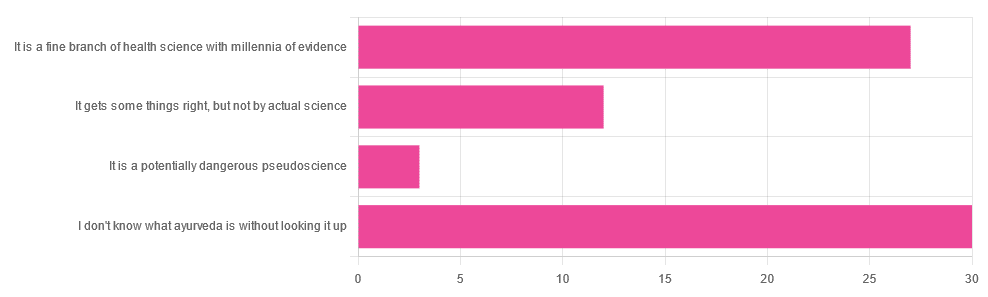
Yesterday, we asked you for your opinions on ayurveda, and got the above-depicted, below-described, set of responses. Of those who responded…
- A little over 41% said “I don’t know what ayurveda is without looking it up”
- A little over 37% said “It is a fine branch of health science with millennia of evidence”
- A little over 16% said “It gets some things right, but not by actual science”
- A little over 4% said “It is a potentially dangerous pseudoscience”
So, what does the science say?
Ayurveda is scientific: True or False?
False, simply. Let’s just rip the band-aid off in this case. That doesn’t mean it’s necessarily without merit, though!
Let’s put it this way:
- If you drink coffee to feel more awake because scientific method has discerned that caffeine has vasoconstrictive and adenosine-blocking effects while also promoting dopaminergic activity, then your consumption of coffee is evidence-based and scientific. Great!
- If you drink coffee to feel more awake because somebody told you that that somebody told them that it energizes you by balancing the elements fire (the heat of the coffee), air (the little bubbles on top), earth (the coffee grinds), water (the water), and ether (steam), then that is neither evidence-based nor scientific, but it will still work exactly the same.
Ayurveda is a little like that. It’s an ancient traditional Indian medicine, based on a combination of anecdotal evidence and supposition.
- The anecdotal evidence from ayurveda has often resulted in herbal remedies that, in modern scientific trials, have been found to have merit.
- Ayurvedic meditative practices also have a large overlap with modern mindfulness practices, and have also been found to have merit
- Ayurveda also promotes the practice of yoga, which is indeed a very healthful activity
- The supposition from ayurveda is based largely in those five elements we mentioned above, as well as a “balancing of humors” comparable to medieval European medicine, and from a scientific perspective, is simply a hypothesis with no evidence to support it.
Note: while ayurveda is commonly described as a science by its practitioners in the modern age, it did not originally claim to be scientific, but rather, wisdom handed down directly by the god Dhanvantari.
Ayurveda gets some things right: True or False?
True! Indeed, we covered some before in 10almonds; you may remember:
Bacopa Monnieri: A Well-Evidenced Cognitive Enhancer
(Bacopa monnieri is also known by its name in ayurveda, brahmi)
There are many other herbs that have made their way from ayurveda into modern science, but the above is a stand-out example. Others include:
- Ashwagandha: The Root of All Even-Mindedness?
- Boswellia serrata (Frankincense) Against Pain and Depression/Anxiety
Yoga and meditation are also great, and not only that, but great by science, for example:
- NCCIH | Yoga for Health: Clinical Guidelines, Scientific Literature, Info for Patients
- The Neuroscience of Mindfulness: How Mindfulness Alters the Brain and Facilitates Emotion Regulation
Ayurveda is a potentially dangerous pseudoscience: True or False?
Also True! We covered why it’s a pseudoscience above, but that doesn’t make it potentially dangerous, per se (you’ll remember our coffee example).
What does, however, make it potentially dangerous (dose-dependent) is its use of heavy metals such as lead, mercury, and arsenic:
Heavy Metal Content of Ayurvedic Herbal Medicine Products
Some final thoughts…
Want to learn more about the sometimes beneficial, sometimes uneasy relationship between ayurveda and modern science?
A lot of scholarly articles trying to bridge (or further separate) the two were very biased one way or the other.
Instead, here’s one that’s reasonably optimistic with regard to ayurveda’s potential for good, while being realistic about how it currently stands:
Development of Ayurveda—Tradition to trend
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

MSG vs. Salt: Sodium Comparison
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Q: Is MSG healthier than salt in terms of sodium content or is it the same or worse?
Great question, and for that matter, MSG itself is a great topic for another day. But your actual question, we can readily answer here and now:
- Firstly, by “salt” we’re assuming from context that you mean sodium chloride.
- Both salt and MSG do contain sodium. However…
- MSG contains only about a third of the sodium that salt does, gram-for-gram.
- It’s still wise to be mindful of it, though. Same with sodium in other ingredients!
- Baking soda contains about twice as much sodium, gram for gram, as MSG.
Wondering why this happens?
Salt (sodium chloride, NaCl) is equal parts sodium and chlorine, by atom count, but sodium’s atomic mass is lower than chlorine’s, so 100g of salt contains only 39.34g of sodium.
Baking soda (sodium bicarbonate, NaHCO₃) is one part sodium for one part hydrogen, one part carbon, and three parts oxygen. Taking each of their diverse atomic masses into account, we see that 100g of baking soda contains 27.4g sodium.
MSG (monosodium glutamate, C₅H₈NO₄Na) is only one part sodium for 5 parts carbon, 8 parts hydrogen, 1 part nitrogen, and 4 parts oxygen… And all those other atoms put together weigh a lot (comparatively), so 100g of MSG contains only 12.28g sodium.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: