Breast Milk’s Benefits That Are (So Far) Not Replicable
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Simply The Breast 🎶
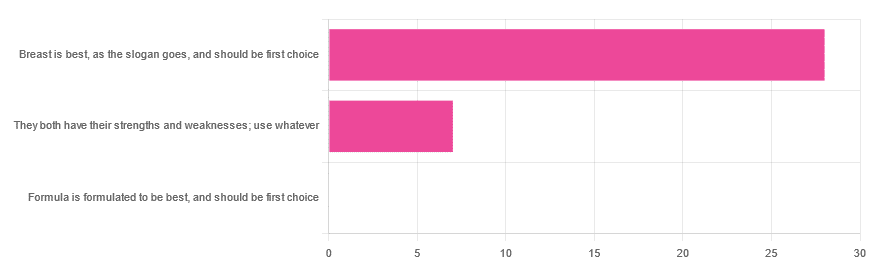
In Wednesday’s newsletter, we asked you for your opinion on breast vs formula milk (for babies!), and got the above-depicted, below-described, set of responses:
- 80% said “Breast is best, as the slogan goes, and should be first choice”
- 20% said “They both have their strengths and weaknesses; use whatever”
- 0% said “Formula is formulated to be best, and should be first choice”
That’s the first time we’ve ever had a possible poll option come back with zero votes whatsoever! It seems this topic is relatively uncontentious amongst our readership, so we’ll keep things brief today, but there is still a little mythbusting to be done.
So, what does the science say?
[Breast milk should be the first choice] at least for the few few weeks and months for the benefit of baby’s health as breast milk has protective factors formula does not: True or False?
True! The wording here was taken from one of our readers’ responses, by the way (thank you, Robin). There are a good number of those protective factors, the most well-known of which is passing on immune cells and cell-like things; in other words, immune-related information being passed from parent* to child.
*usually the mother, though in principle it could be someone else and in practice sometimes it is; the only real requirements are that the other person be healthy, lactating, and willing.
As for immune benefits, see for example:
Perspectives on Immunoglobulins in Colostrum and Milk
And for that matter, also:
(Colostrum is simply the milk that is produced for a short period after giving birth; the composition of milk will tend to change later)
In any case, immunoglobulin A is a very important component in breast milk (colostrum and later), as well as lactoferrin (has an important antimicrobial effect and is good for the newborn’s gut), and a plethora of cytokines:
As for that about the gut, lactoferrin isn’t the only breast milk component that benefits this, by far, and there’s a lot that can’t be replicated yet:
Human Breast Milk and the Gastrointestinal Innate Immune System
As long as your infant/child is nutritiously fed, it shouldn’t matter if it comes from breast or formula: True or False?
False! Formula milk will not convey those immune benefits.
This doesn’t mean that formula-feeding is neglectful; as several people who commented mentioned*, there are many reasons a person may not be able to breastfeed, and they certainly should not be shamed for that.
*(including the reader whose words we borrowed for this True/False item; the words we quoted above were prefaced with: “Not everyone is able to breastfeed for many different reasons”)
But, while formula milk is a very good second choice, and absolutely a respectable choice if breast milk isn’t an option (or an acceptable option) for whatever reason, it still does not convey all the health benefits of breast milk—yet! The day may come when they’ll find a way to replicate the immune benefits, but today is not that day.
They both have their strengths and weaknesses: True or False?
True! But formula’s strengths are only in the category of convenience and sometimes necessity—formula conveys no health benefits that breast milk could not do better, if available.
For many babies, formula means they get to eat, when without it they would starve due to non-availability of breast milk. That’s a pretty important role!
Note also: this is a health science publication, not a philosophical publication, but we’d be remiss not to mention one thing; let’s bring it in under the umbrella of sociology:
The right to bodily autonomy continues to be the right to bodily autonomy even if somebody else wants/needs something from your body.
Therefore, while there are indeed many good reasons for not being able to breastfeed, or even just not being safely* able to breastfeed, it is at the very least this writer’s opinion that nobody should be pressed to give their reason for not breastfeeding; “no” is already a sufficient answer.
*Writer’s example re safety: when I was born, my mother was on such drugs that it would have been a very bad idea for her to breastfeed me. There are plenty of other possible reasons why it might be unsafe for someone one way or another, but “on drugs that have a clear ‘do not take while pregnant or nursing’ warning” is a relatively common one.
All that said, for those who are willing and safely able, the science is clear: breast is best.
Want to read more?
The World Health Organization has a wealth of information (including explanations of its recommendations of, where possible, exclusive breastfeeding for the first 6 months, ideally continuing some breastfeeding for the first 2 years), here:
World Health Organization | Breastfeeding
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Mango vs Pear – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing mango to pear, we picked the mango.
Why?
In terms of macros, pear starts out strong with 2x the fiber for similar carbs and near-equally minimal protein, winning in this category.
In the category of vitamins, however, mango has a lot more of vitamins A, B1, B2, B3, B5, B6, B7, B9, C, and E, while pears are not higher in any vitamin (although they are equal in vitamin K), meaning a 10:0 win for mango here.
Looking at minerals, mango has more calcium, copper, magnesium, manganese, phosphorus, potassium, and selenium, while pears have more iron and zinc, yielding a 7:2 win for mango this time.
Adding up the sections makes for an overall win for mango, but by all means enjoy either or both, as diversity is good!
Want to learn more?
You might like:
What’s Your Plant Diversity Score?
Enjoy!
Share This Post
-

Simple, 10-Minute Hip Opening Routine
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Hips Feeling Stiff?
If so, Flow with Adee’s video (below) has just the solution with a quick 10-minute hip-opening routine. Designed for intermediates but open to all, we love Adee’s work and recommend that you reach out to her to tell her what you’d like to see next.
Other Methods
If you’re a book lover, we’ve reviewed a fantastic book on reducing hip pain. Alternatively, learn stretching from a ballerina with Jasmine McDonald’s ballet stretching routine.
Otherwise, enjoy today’s video:
How was the video? If you’ve discovered any great videos yourself that you’d like to share with fellow 10almonds readers, then please do email them to us!
Share This Post
-

Younger Next Year: The Exercise Program – by Chris Crowley & Dr. Henry Lodge
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We previously reviewed the same authors’ original “Younger Next Year”, and now here’s the more specific book about exercise for increasing healthspan and reversing markers of biological aging, going into much more detail in that regard.
How much more? Well, it’s a very hand-holding book in the sense that it walks the reader through everything step-by-step, tells not only what kind of exercise and how much, but also how to do, what things to do to prepare, how to avoid not erring in various ways, what metrics to keep an eye on to ensure you are making progress, and more.
There are also whole sections on specific common age-related issues including osteoporosis and arthritis, as well as how to train around injuries (especially of the kind that basically aren’t likely to ever fully go away).
As with the previous book, there’s a blend of motivational pep talk and science—this book is heavily weighted towards the former. It has, however, enough science to keep it on the right track throughout. Hence the two authors! Crowley for motivational pep and training tips, and Dr. Lodge for the science.
Bottom line: if you’d like to be biologically younger next year, that exercise will be an important component of that, and this book is really quite comprehensive for its relative brevity (weighing in at 176 pages).
Click here to check out Younger Next Year: The Exercise Program, and make that progress!
Share This Post

Related Posts
-
Peanuts vs Hazelnuts – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing peanuts to hazelnuts, we picked the hazelnuts.
Why?
It was close!
In terms of macros, peanuts have more protein while hazelnuts have more fiber and fat; the fat is healthy (mostly monounsaturated, some polyunsaturated, and very little saturated; less saturated fat than peanuts), so all in all, we’ll call this category a modest, subjective win for hazelnuts (since it depends on what we consider most important).
In the category of vitamins, peanuts have more of vitamins B2, B3, B5, B9, and choline, while hazelnuts have more of vitamins A, B1, B6, C, E, and K, making this one a marginal win for hazelnuts.
When it comes to minerals, peanuts have more magnesium, phosphorus, selenium, and zinc, while hazelnuts have more calcium, copper, iron, and manganese, so we’re calling it a tie on minerals.
Adding up the sections makes for a very close win for hazelnuts, but by all means enjoy both (unless you are allergic, of course)!
Want to learn more?
You might like to read:
Why You Should Diversify Your Nuts!
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
10 Skin Warning Signs You Should Never Ignore
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Do you have armpits? Don’t ignore them!
Heed the signs:
Without further ado, they are:
- Acanthosis nigricans: dark, velvety brown skin thickening on the neck, underarms, backs of the hands, or sides of the face can signal insulin resistance, prediabetes, or PMOS. The good news, however, is that despite common concerns of such, sudden widespread onset is rarely associated with cancer.
- Unexplained bruising: bruises appearing without remembered injury may be linked to platelet disorders, clotting disorders, vitamin deficiencies, liver disease, certain cancers, or medications such as blood thinners and corticosteroids; bruising accompanied by nosebleeds, bleeding gums, or large purple patches is especially concerning and merits medical attention.
- Yellowing of the skin or eyes: jaundice can indicate liver disease, bile duct obstruction, or increased breakdown of red blood cells; yellowing often appears under the tongue and inside the mouth before becoming obvious elsewhere. It’s worth knowing that unlike harmless carotene-related skin discoloration (i.e. you drank a lot of carrot juice and turned orange), jaundice also affects the eyes and mouth.
- Severe itching without a rash: persistent whole-body itching lasting more than six weeks with no visible rash can be associated with liver disease, kidney disease, thyroid disorders, iron deficiency, or cancers such as Hodgkin lymphoma. Itching triggered by showering is another warning sign.
- Thick, waxy, or tight skin: swollen, shiny, waxy skin on the shins may occur with Graves’ disease, while skin tightening on the fingers may suggest diabetes or Scleroderma, particularly when hand mobility becomes restricted.
- Butterfly rash on the face: a rash across the cheeks and nose that spares the folds beside the nose famously may indicate systemic lupus erythematosus, especially if it worsens with sun exposure and is accompanied by fatigue or joint pain.
- Dark streaks under the nails: a new dark band in a single nail, particularly one that widens, contains multiple colors, or extends onto the surrounding skin, can be a warning sign of melanoma and should be evaluated for such.
- Sudden hair shedding: rapid diffuse hair loss, known as telogen effluvium, often occurs about three months after a physical stressor and may be associated with thyroid disease, iron deficiency, infection, surgery, trauma, nutritional deficiencies, pregnancy, or rapid weight loss.
- Non-healing wounds or recurrent infections: cuts, scrapes, or ulcers that remain open for more than four weeks generally suggest poor circulation, vascular disease, diabetes, or impaired immune function.
- Yellow, thick, or crumbly nails: commonly caused by a fungal infection, but when accompanied by respiratory symptoms and leg swelling, they may indicate bigger problems and should be checked out.
For more on all of this plus visual illustrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
What Your Skin Texture Says About Your Health
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Pasteurization: What It Does And Doesn’t Do
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Pasteurization’s Effect On Risks & Nutrients

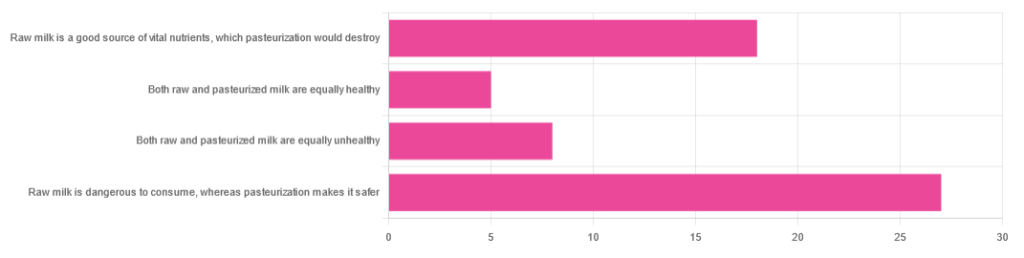
In Wednesday’s newsletter, we asked you for your health-related opinions of raw (cow’s) milk, and got the above-depicted, below-described, set of responses:
- About 47% said “raw milk is dangerous to consume, whereas pasteurization makes it safer”
- About 31% said “raw milk is a good source of vital nutrients which pasteurization would destroy”
- About 14% said “both raw milk and pasteurized milk are equally unhealthy”
- About 9% said “both raw milk and pasteurized milk are equally healthy”
Quite polarizing! So, what does the science say?
“Raw milk is dangerous to consume, whereas pasteurization makes it safer: True or False?”
True! Coincidentally, the 47% who voted for this are mirrored by the 47% of the general US population in a similar poll, deciding between the options of whether raw milk is less safe to drink (47%), just as safe to drink (15%), safer to drink (9%), or not sure (30%):
Public Fails to Appreciate Risk of Consuming Raw Milk, Survey Finds
As for what those risks are, by the way, unpasteurized dairy products are estimated to cause 840x more illness and 45x more hospitalizations than pasteurized products.
This is because unpasteurized milk can (and often does) contain E. coli, Listeria, Salmonella, Cryptosporidium, and other such unpleasantries, which pasteurization kills.
Source for both of the above claims:
(we know the title sounds vague, but all this information is easily visible in the abstract, specifically, the first two paragraphs)
Raw milk is a good source of vital nutrients which pasteurization would destroy: True or False?
False! Whether it’s a “good” source can be debated depending on other factors (e.g., if we considered milk’s inflammatory qualities against its positive nutritional content), but it’s undeniably a rich source. However, pasteurization doesn’t destroy or damage those nutrients.
Incidentally, in the same survey we linked up top, 16% of the general US public believed that pasteurization destroys nutrients, while 41% were not sure (and 43% knew that it doesn’t).
Note: for our confidence here, we are skipping over studies published by, for example, dairy farming lobbies and so forth. Those do agree, by the way, but nevertheless we like sources to be as unbiased as possible. The FDA, which is not completely unbiased, has produced a good list of references for this, about half of which we would consider biased, and half unbiased; the clue is generally in the journal names. For example, Food Chemistry and the Journal of Food Science and Journal of Nutrition are probably less biased than the International Dairy Association and the Journal of Dairy Science:
FDA | Raw Milk Misconceptions and the Danger of Raw Milk Consumption
this page covers a lot of other myths too, more than we have room to “bust” here, but it’s very interesting reading and we recommend to check it out!
Notably, we also weren’t able to find any refutation by counterexample on PubMed, with the very slight exception that some studies sometimes found that in the case of milks that were of low quality, pasteurization can reduce the vitamin E content while increasing the vitamin A content. For most milks however, no significant change was found, and in all cases we looked at, B-vitamins were comparable and vitamin D, popularly touted as a benefit of cow’s milk, is actually added later in any case. And, importantly, because this is a common argument, no change in lipid profiles appears to be findable either.
In science, when something has been well-studied and there aren’t clear refutations by counterexample, and the weight of evidence is clearly very much tipped into one camp, that usually means that camp has it right.
Milk generally is good/bad for the health: True or False?
True or False, depending on what we want to look at. It’s definitely not good for inflammation, but the whole it seems to be cancer-neutral and only increases heart disease risk very slightly:
- Keep Inflammation At Bay ← short version is milk is bad, fermented milk products are fine in moderation
- Is Dairy Scary? ← short version is that milk is neither good nor terrible; fermented dairy products however are health-positive in numerous ways when consumed in moderation
You may be wondering…
…how this goes for the safety of dairy products when it comes to the bird flu currently affecting dairy cows, so:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: