5 Things You Can Change About Your Personality (But: Should You?)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There are many personality-typing systems that, with varying degrees of validity*, aim to describe a person’s personality.
*and often pseudoscience:
- sometimes obviously so like astrology
- sometimes dressed up in clinical words like the Meyers-Briggs
- sometimes openly, per “this is not science but you may find it useful to frame things this way”, like the Enneagram
There is currently one kind of personality-typing system (with some minor variations) that is used in the actual field of clinical psychology, specifically under the umbrella of “trait theory”, and that is…
The “Big Five” personality traits
Also called the OCEAN or CANOE model, based on its 5 components:
- openness to experience: inventive/curious rather than consistent/cautious
- conscientiousness: efficient/organized rather than extravagant/careless
- extroversion: outgoing/energetic rather than solitary/reserved
- agreeableness: friendly/compassionate rather than critical/judgmental
- neuroticism: sensitive/nervous rather than resilient/confident
The latter (neuroticism) is not to be confused with neurosis, which is very different and beyond the scope of today’s article.
Note that some of these seem more positive/negative than others at a glance, but really, any of these could be a virtue or a vice depending on specifics or extremity.
For scientific reference, here’s an example paper:
The Big Five Personality Factors and Personal Values
Quick self-assessment
There are of course many lengthy questionnaires for this, but in the interests of expediency:
Take a moment to rate yourself as honestly as you can, on a scale of 1–10, for each of those components, with 10 being highest for the named trait.
For example, this writer gives herself: O7, C6, E3, A8, N2 (in other words I’d say I’m fairly open, moderately conscientious, on the reserved side, quite agreeable, and quite resilient)
Now, put your rating aside (in your phone’s notes app is fine, if you hadn’t written it down already) and forget about it for the moment, because we want you to do the next exercise from scratch.
Who would you be, at your best?
Now imagine your perfect idealized self, the best you could ever be, with no constraints.
Take a moment to rate your idealized self’s personality, on a scale of 1–10, for each of those components, with 10 being highest for the named trait.
For example, this writer picks: O9, C10, E5, A8, N1.
Maybe this, or maybe your own idealized self’s personality, will surprise you. That some traits might already be perfect for you already; others might just be nudged a little here or there; maybe there’s some big change you’d like. Chances are you didn’t go for a string of 10s or 1s (though if you did, you do you; there are no wrong answers here as this one is about your preferences).
We become who we practice being
There are some aspects of personality that can naturally change with age. For example:
- confidence/resilience will usually gradually increase with age due to life experience (politely overlook teenagers’ bravado; they are usually a bundle of nerves inside, resulting in the overcompensatory displays of confidence)
- openness to experience may decrease with age, as we can get into a rut of thinking/acting a certain way, and/or simply consciously decide that our position on something is already complete and does not need revision.
But, we can decide for ourselves how to nudge our “Big Five” traits, for example:
- We can make a point of seeking out new experiences, and considering new ideas, or develop strategies for reining ourselves in
- We can use systems to improve our organization, or go out of our way to introduce a little well-placed chaos
- We can “put ourselves out there” socially, or make the decision to decline more social invitations because we simply don’t want to
- We can make a habit of thinking kindly of others and ourselves, or we can consciously detach ourselves and look on the cynical side more
- We can build on our strengths and eliminate our weaknesses, or lean into uncomfortable emotions
Some of those may provoke a “why would anyone want to…?” response, but the truth is we are all different. An artist and a police officer may have very different goals for who they want to be as a person, for example.
Interventions to change personality can and do work:
A systematic review of personality trait change through intervention
There are many ways to go about “being the change we want to see” in ourselves, and yes there can be a degree of “fake it until you make it” if that works for you, but it doesn’t have to be so. It can also simply be a matter of setting yourself reminders about the things that are most important to you.
Writer’s example: pinned above my digital workspace I have a note from my late beloved, written just under a week before death. The final line reads, “keep being the good person that you are” (on a human level, the whole note is uplifting and soothing to me and makes me smile and remember the love we shared; or to put it in clinical terms, it promotes high agreeableness, low neuroticism).
Other examples could be a daily practice of gratitude (promotes lower neuroticism), or going out of your way to speak to your neighbors (promotes higher extraversion), signing up for a new educational course (promotes higher openness) or downloading a budgeting app (promotes higher conscientiousness).
In short: be the person you want to be, and be that person deliberately, because you can.
Some resources that may help for each of the 5 traits:
- Curiosity Kills The Neurodegeneration
- How (And Why) To Train Your Pre-Frontal Cortex
- How To Beat Loneliness & Isolation
- Optimism Seriously Increases Longevity!
- Building Psychological Resilience (Without Undue Hardship)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

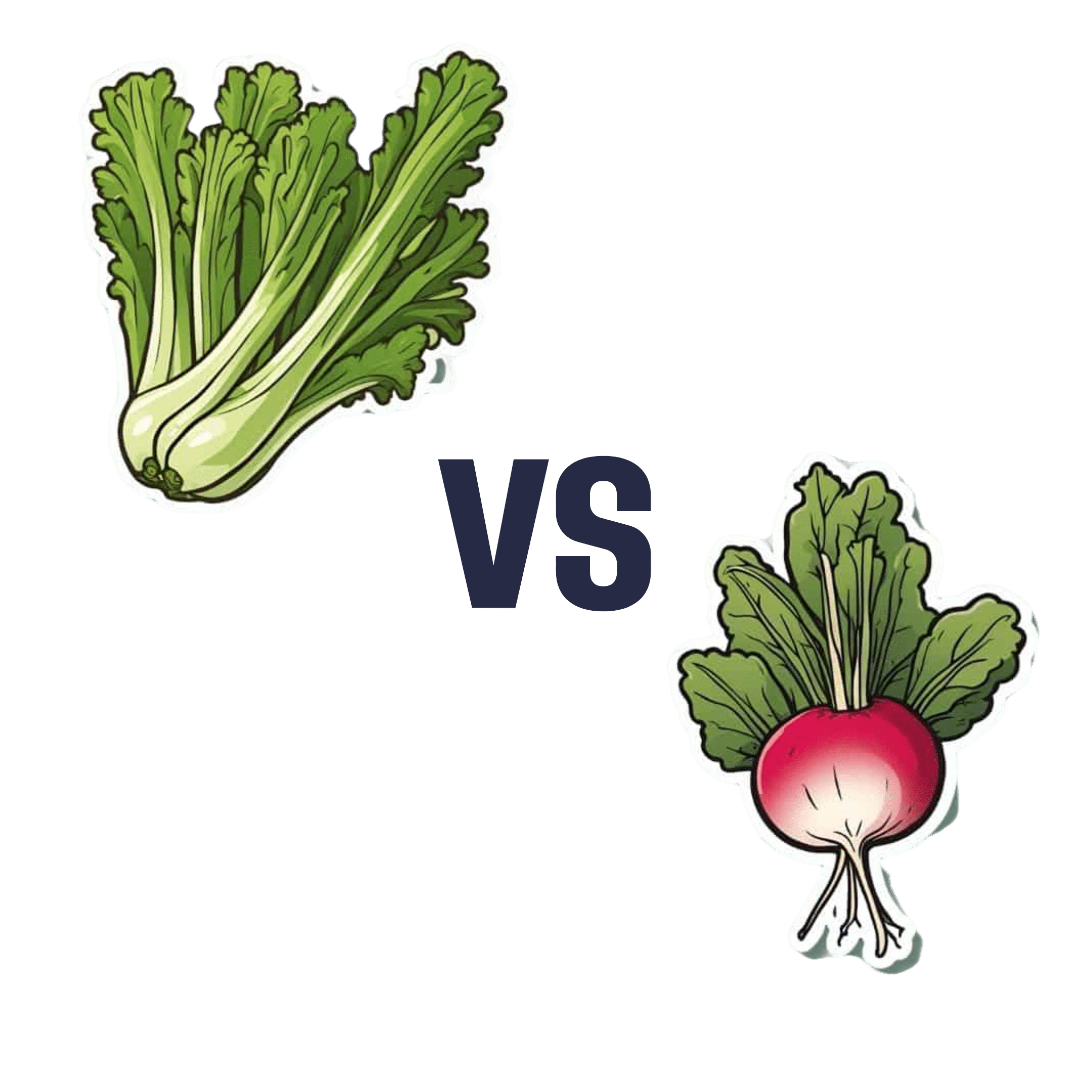
Celery vs Radish – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing celery to radish, we picked the celery.
Why?
It was very close! And yes, surprising, we know. Generally speaking, the more colorful/pigmented an edible plant is, the healthier it is. Celery is just one of those weird exceptions (as is cauliflower, by the way).
Macros-wise, these two are pretty much the same—95% water, with just enough other stuff to hold them together. The proportions of “other stuff” are also pretty much equal.
In the category of vitamins, celery has more vitamin K while radish has more vitamin C; the other vitamins are pretty close to equal. We’ll call this one a minor win for celery, as vitamin K is found in fewer foods than vitamin C.
When it comes to minerals, celery has more calcium, manganese, phosphorus, and potassium, while radish has more copper, iron, selenium, and zinc. We’ll call this a minor win for radish, as the margins are a little wider for its minerals.
So, that makes the score 1–1 so far.
Both plants have an assortment of polyphenols, of which, when we add up the averages, celery comes out on top by some way. Celery also comes out on top when we do a head-to-head of the top flavonoid of each; celery has 5.15mg/100g of apigenin to radish’s 0.63mg/100g kaempferol.
Which means, both are great healthy foods, but celery wins the day.
Want to learn more?
You might like to read:
Celery vs Cucumber – Which is Healthier?
Take care!
Share This Post
-

How To Prevent And Reverse Type 2 Diabetes
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Turn back the clock on insulin resistance

This is Dr. Jason Fung. He’s a world-leading expert on intermittent fasting and low carbohydrate approaches to diet. He also co-founded the Intensive Dietary Management Program, later rebranded to the snappier title: The Fasting Method, a program to help people lose weight and reverse type 2 diabetes. Dr. Fung is certified with the Institute for Functional Medicine, for providing functional medicine certification along with educational programs directly accredited by the Accreditation Council for Continuing Medical Education (ACCME).
Why Intermittent Fasting?
Intermittent fasting is a well-established, well-evidenced, healthful practice for most people. In the case of diabetes, it becomes complicated, because if one’s blood sugars are too low during a fasting period, it will need correcting, thus breaking the fast.
Note: this is about preventing and reversing type 2 diabetes. Type 1 is very different, and sadly cannot be prevented or reversed in this fashion.
However, these ideas may still be useful if you have T1D, as you have an even greater need to avoid developing insulin resistance; you obviously don’t want your exogenous insulin to stop working.
Nevertheless, please do confer with your endocrinologist before changing your dietary habits, as they will know your personal physiology and circumstances in ways that we (and Dr. Fung) don’t.
In the case of having type 2 diabetes, again, please still check with your doctor, but the stakes are a lot lower for you, and you will probably be able to fast without incident, depending on your diet itself (more on this later).
Intermittent Fasting can be extra helpful for the body in the case of type 2 diabetes, as it helps give the body a rest from high insulin levels, thus allowing the body to become gradually re-sensitised to insulin.
Why low carbohydrate?
Carbohydrates, especially sugars, especially fructose*, cause excess sugar to be quickly processed by the liver and stored there. When the body’s ability to store glycogen is exceeded, the liver stores energy as fat instead. The resultant fatty liver is a major contributor to insulin resistance, when the liver can’t keep up with the demand; the blood becomes spiked full of unprocessed sugars, and the pancreas must work overtime to produce more and more insulin to deal with that—until the body starts becoming desensitized to insulin. In other words, type 2 diabetes.
There are other factors that affect whether we get type 2 diabetes, for example a genetic predisposition. But, our carb intake is something we can control, so it’s something that Dr. Fung focuses on.
*A word on fructose: actual fruits are usually diabetes-neutral or a net positive due to their fiber and polyphenols.
Fructose as an added ingredient, however, not so much. That stuff zips straight into your veins with nothing to slow it down and nothing to mitigate it.
The advice from Dr. Fung is simple here: cut the carbs. If you are already diabetic and do this with no preparation, you will probably simply suffer hypoglycemia, so instead:
- Enjoy a fibrous starter (a salad, some fruit, or perhaps some nuts)
- Load up with protein first, during your main meal—this will start to trigger your feelings of satedness
- Eat carbs last (preferably whole, unprocessed carbohydrates), and stop eating when 80% full.
Adapting Intermittent Fasting to diabetes
Dr. Fung advocates for starting small, and gradually increasing your fasting period, until, ideally, fasting 16 hours per day. You probably won’t be able to do this immediately, and that’s fine.
You also probably won’t be able to do this, if you don’t also make the dietary adjustments that help to give your liver a break, and thus by knock-on-effect, give your pancreas a break too.
With the dietary adjustments too, however, your insulin production-and-response will start to return to its pre-diabetic state, and finally its healthy state, after which, it’s just a matter of maintenance.
Want to hear more from Dr. Fung?
You may enjoy his blog, and for those who like videos, here is his YouTube channel:
Share This Post
-

How Your Diet May Be Causing Chronic Tightness (& How To Fix It)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There is often more to hamstring flexibility than just stretching:
Three steps
The method focuses on three areas: diet, mindset, and movement.
Why diet? Poor gut health and inflammation, often caused by processed and fast foods, contribute to chronic hamstring tightness. The video suggests nutrient-dense meals like Greek yogurt with poached eggs. As for collagen, that is found most abundantly in the bones and skin of fish and other animals, but if you are vegan/vegetarian, fear not, you can just make sure to eat plenty of its constituent parts instead, and synthesize it yourself like any other animal. See also: The Best Foods For Collagen Production
Why mindset? Addressing pain and other somatic (bodily) concerns involves understanding the body as a single interconnected system. So, it’s necessary to also take care of any emotional stress or other underlying conditions, as well as ensuring your hormones are all in order.
Why movement? Machine-based training, which isolates muscles, can cause imbalances. Instead, consider functional movements like hanging and compound exercises such as Pilates or other calisthenics systems. These improve core strength, enhance flexibility, and prevent stiffness, ensuring better overall function.
Some example exercises:
- Bent knee hamstring stretch: hold for 2 seconds; do 10–12 reps (2 sets per leg).
- Straight leg active isolation: focus on quad engagement with assistance from a band; 10–12 reps (2 sets per leg).
- Active hip abductors: target IT band and glute medius; 1 set of 12 reps per leg.
- Active lunge stretch: incorporate a band to intensify the stretch; 2 seconds at the top range.
For more on all of this plus visual demonstrations of the exercises, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Fix Tight Hamstrings In Just 3 Steps
Take care!
Share This Post

Related Posts
-

Anti-Cholesterol Cardamom & Pistachio Porridge
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This tasty breakfast’s beta-glucan content binds to cholesterol and carries it out of the body; there are lots of other nutritional benefits too!
You will need
- 1 cup coconut milk
- ⅓ cup oats
- 4 tbsp crushed pistachios
- 6 cardamom pods, crushed
- 1 tsp rose water or 4 drops edible rose essential oil
- Optional sweetener: drizzle of honey or maple syrup
- Optional garnishes: rose petals, chopped nuts, dried fruit
Method
(we suggest you read everything at least once before doing anything)
1) Heat the coconut milk, adding the oats and crushed cardamom pods. Simmer for 5–10 minutes depending on how cooked you want the oats to be.
2) Stir in the crushed pistachio nuts, as well as the rose water.
3) Serve in a bowl, adding any optional toppings:

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- The Best Kind Of Fiber For Overall Health? ← it’s beta-glucan, which is fund abundantly in oats
- Pistachios vs Pecans – Which is Healthier? ← have a guess
- Can Saturated Fats Be Healthy? ← coconut can!
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Train For The Event Of Your Life!
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Mobility As A Sporting Pursuit
As we get older, it becomes increasingly important to treat life like a sporting event. By this we mean:
As an “athlete of life”, there are always events coming up for which we need to train. Many of these events will be surprise tests!
Such events/tests might include:
- Not slipping in the shower and breaking a hip (or worse)
- Reaching an item from a high shelf without tearing a ligament
- Getting out of the car at an awkward angle without popping a vertebra
- Climbing stairs without passing out light-headed at the top
- Descending stairs without making it a sled-ride-without-a-sled
…and many more.
Train for these athletic events now
Not necessarily this very second; we appreciate you finishing reading first. But, now generally in your life, not after the first time you fail such a test; it can (and if we’re not attentive: will) indeed happen to us all.
With regard to falling, you might like to revisit our…
…which covers how to not fall, and to not injure yourself if you do.
You’ll also want to be able to keep control of your legs (without them buckling) all the way between standing and being on the ground.
Slav squats or sitting squats (same exercise, different names, amongst others) are great for building and maintaining this kind of strength and suppleness:
(Click here for a refresher if you haven’t recently seen Zuzka’s excellent video explaining how to do this, especially if it’s initially difficult for you, “The Most Anti-Aging Exercise”)
this exercise is, by the way, great for pretty much everything below the waist!
You will also want to do resistance exercises to keep your body robust:
Resistance Is Useful! (Especially As We Get Older)
And as for those shoulders? If it is convenient for you to go swimming, then backstroke is awesome for increasing and maintaining shoulder mobility (and strength).
If swimming isn’t a viable option for you, then doing the same motion with your arms, while standing, will build the same flexibility. If you do it while holding a small weight (even just 1kg is fine, but feel free to increase if you so wish and safely can) in each hand will build the necessary strength as you go too.
As for why even just 1kg is fine: read on
About that “and strength”, by the way…
Stretching is not everything. Stretching is great, but mobility without strength (in that joint!) is just asking for dislocation.
You don’t have to be built like the Terminator, but you do need to have the structural integrity to move your body and then a little bit more weight than that (or else any extra physical work could be enough to tip you to breaking point) without incurring damage from the strain. So, it needs to not be a strain! See again, the aforementioned resistance exercises.
That said, even very gentle exercise helps too; see for example the impact of walking on osteoporosis:
Living near green spaces linked to higher bone density and lower osteoporosis risk
and…
So you don’t have to run marathons—although you can if you want:
Marathons in Mid- and Later-Life
…to keep your hips and more in good order.
Want to test yourself now?
Check out:
Building & Maintaining Mobility
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Healthy Heart, Healthy Brain – by Dr. Bradley Bale & Dr. Amy Doneen
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve often written that “what’s good for your heart is good for your brain”, because the former feeds the latter and takes away detritus. You cannot have a healthy brain without a healthy heart.
This book goes into that in more detail than we have ever had room to here! This follows from their previous book “Beat The Heart Attack Gene”, but we’re jumping in here because that book doesn’t really contain anything not also included in this one.
The idea is the same though: it is the authors’ opinion that far too many interventions are occurring far too late, and they want to “wake everyone up” (including their colleagues in the field) to encourage earlier (and broader!) testing.
Fun fact: that also reminded this reviewer that she had a pending invitation for blood tests to check these kinds of things—phlebotomy appointment now booked, yay!
True the spirit of such exhortation to early testing, this book does include diagnostic questionnaires, to help the reader know where we might be at. And, interestingly, while the in-book questionnaire format of “so many points for this answer, so many for that one”, etc is quite normal, what they do differently in the diagnostics is that in cases of having to answer “I don’t know”, it assigns the highest-risk point value, i.e. the test will err on the side of assume the worst, in the case of a reader not knowing, for example, what our triglycerides are like. Which, when one thinks about it, is probably a very sensible reasoning.
There’s a lot of advice about specific clinical diagnostic tools and things to ask for, and also things that may raise an alarm that most people might overlook (including doctors, especially if they are only looking for something else at the time).
You may be wondering: do they actually give advice on what to actually do to improve heart and brain health, or just how to be aware of potential problems? And the answer is that the latter is a route to the former, and yes they do offer comprehensive advice—well beyond “eat fiber and get some exercise”, and even down to the pros and cons of various supplements and medications. When it comes to treating a problem that has been identified, or warding off a risk that has been flagged, the advice is a personalized, tailored, approach. Obviously there’s a limit to how much they can do that in the book, but even so, we see a lot of “if this then that” pointers to optimize things along the way.
The style is… a little salesy for this reviewer’s tastes. That is to say, while it has a lot of information of serious value, it’s also quite padded with self-congratulatory anecdotes about the many occasions the authors have pulled a Dr. House and saved the day when everyone else was mystified or thought nothing was wrong, the wonders of their trademarked methodology, and a lot of hype for their own book, as in, the book that’s already in your hands. Without all this padding, the book could have been cut by perhaps a third, if not more. Still, none of that takes away from the valuable insights that are in the book too.
Bottom line: if you’d like to have a healthier heart and brain, and especially if you’d like to avoid diseases of those two rather important organs, then this book is a treasure trove of information.
Click here to check out Healthy Heart, Healthy Brain, and secure your good health now, for later!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: