How to keep your teeth young
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How to keep your teeth young
The association between aging and teeth is so well-established that it’s entered popular idiom, “too long in the tooth”, and when it comes to visual representations, false teeth are well-associated with old age.
And yet, avoiding such outcomes does not get anywhere near so much attention as, say, avoiding wrinkles or hair loss.
At 10almonds, we’ve covered general dental health before, in a three-part series:
- Toothpastes & Mouthwashes: Which Help And Which Harm?
- Flossing, Better (And Easier!)
- Less Common Oral Hygiene Options
Today, we’re going to be looking specifically at keeping our teeth young. What if you have lost your teeth already? Well, gum health remains important, and it’s foundational for everyone, so…
Look after your gums first and last
Hollywood’s most “perfect” whites would be nothing without the gums holding them in place. So, set aside the cosmetic whitening products that often harm gums (anything containing bleach / hydrogen peroxide, is generally a bad idea), andinstead focus on your gums.
As for avoiding gum disease (periodontitis)?
❝In conclusion, periodontitis might enhance the association of biological aging with all-cause mortality in middle-aged and older adults.
Hence, maintaining and enhancing periodontal health is expected to become an intervention to slow aging and extend life span.❞
Source: Does Periodontitis Affect the Association of Biological Aging with Mortality?
Ways to look after gum health include the obvious “floss” and “brush often” and “use fluoride toothpaste”, along with other options we covered in our “Less Common Oral Hygiene Options” article above.
Also important: don’t smoke. It is bad for everything, and this is no exception.
We expect we probably don’t have many subscribers who smoke, but if you do, please consider making quitting a priority.
See also: Smoking, Gum Disease, and Tooth Loss
Consider supplementing with collagen
Everyone’s all about the calcium and vitamin D for bones (and teeth), but a large part of the mass of both is actually collagen. And unlike calcium, which most people not living in a food desert get plenty of, or vitamin D, which is one of the most popular supplements around, collagen is something that gets depleted as we get older. We’ve written about its importance for bones:
We Are Such Stuff As Fish Are Made Of—Collagen’s benefits are more than skin deep
And as for its role in combatting gum disease and tooth loss:
Nanoscale Dynamics of Streptococcal Adhesion to AGE-Modified Collagen
By the way, that “AGE” there isn’t about chronological age; it’s about advanced glycation end-products. Those are also something you can and should avoid:
A different kind of “spit and polish”
We imagine you have the “polishing” part in hand; that’s tooth-brushing, of course. But spit?
Saliva is hugely important for our oral health, but it’s not something most of us think about a lot. For example, you might not have known (or might have known but not thought much about) that many common medications affect our saliva, including many blood pressure medications and antidepressants:
Impact of ageing and drug consumption on oral health
Because there are so many possibilities, this is the kind of thing to check with your pharmacist or doctor about. But as a rule, if you take a medication whose side-effects include “dry mouth”, this might be you.
Here’s a really useful (academic) article that covers what drugs cause this, how to diagnose it, and what can be done about it:
Hyposalivation in Elderly Patients
If something’s difficult, find a way to make it easier
Sometimes, as we get older, some things that used to be easy, aren’t. We can lose strength, coordination, manual dexterity, memory, attention, and more. Obviously, we try not to, and do what we can to keep ourselves in good health.
But, if you do have some disability that makes for example brushing and/or flossing difficult to do consistently and/or well, consider talking to your doctor to see if there are assistive devices that can help, or some other kind of support that could allow you to do what you need to.
There’s never any shame in getting help if we need it.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Which Diet? Top Diets Ranked By Experts

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A panel of 69 doctors and nutritionists examined the evidence for 38 diets, and scored them in 21 categories (e.g. best for weight loss, best for heart, best against diabetes, etc).
We’ll not keep it a mystery: the Mediterranean diet has been ranked as “best overall” for the 8th year in a row.
The Mediterranean (And Its Close Friends & Relations)
We’ve written before about the Mediterranean diet, here:
The Mediterranean Diet: What Is It Good For? ← What isn’t it good for?
👆 the above article also delineates what does and doesn’t go in a Mediterranean diet—hint, it’s not just any food from the Mediterranean region!
The Mediterranean diet’s strengths come from various factors including its good plant:animal ratio (leaning heavily on the plants), colorful fruit and veg minimally processed, and the fact that olive oil is the main source of fat:
All About Olive Oil ← pretty much one of the healthiest fats we can consume, if not healthiest all-rounder fat
The Mediterranean diet also won 1st place in various more specific categories, including:
- Best against arthritis (followed by Dr. Weil’s Anti-inflammatory, MIND, DASH)
- Best for mental health (followed by MIND, Flexitarian, DASH)
- Best against diabetes (followed by Flexitarian, DASH, MIND)
- best for liver regeneration (followed by Flexitarian, Vegan, DASH, MIND)
- Best for gut heath (followed by Vegan, DASH, Flexitarian, MIND)
If you’re not familiar with DASH and MIND, there are clues in their full names: Dietary Approaches to Stop Hypertension and Mediterranean-DASH Intervention for Neurodegenerative Delay, and as you might well suspect, they are simply tweaked variations of the Mediterranean diet:
Four Ways To Upgrade The Mediterranean ← DASH and MIND are the heart-healthiest and brain-healthiest versions of the Mediterranean; this article also includes a gut-healthiest version and a most anti-inflammatory version
What aren’t those best for?
The Mediterranean diet scored 1st or 2nd in most of the 21 categories, and usually had the other above-named diets keeping it company in the top few.
When it comes to weight loss, the Mediterranean scored 2nd place and wasn’t flanked by its usual friends and relations; instead in first place was commercial diet WeightWatchers (likely helped a lot by being also a peer support group), and in third place was the Volumetrics diet, which we wrote about here:
Some Surprising Truths About Hunger And Satiety
And when it comes to rapid weight loss specifically, the Mediterranean didn’t even feature in the top spots at all, because it’s simply not an extreme diet and it prioritizes health over shedding the pounds at any cost. The top in that category were mostly commercial diets:
- Jenny Craig
- Slimfast
- Keto
- Nutrisystem
- WeightWatchers
We’ve not as yet written about any of those commercial diets, but we have written about keto here:
Ketogenic Diet: Burning Fat Or Burning Out?
Want to know more?
You can click around, exploring by diet or by health category, here 😎
Enjoy!
Share This Post
-

What’s the difference between miscarriage and stillbirth?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What’s the difference? is a new editorial product that explains the similarities and differences between commonly confused health and medical terms, and why they matter.
Former US First Lady Michelle Obama revealed in her memoir she had a miscarriage. UK singer-songwriter and actor Lily Allen has gone on the record about her stillbirth.
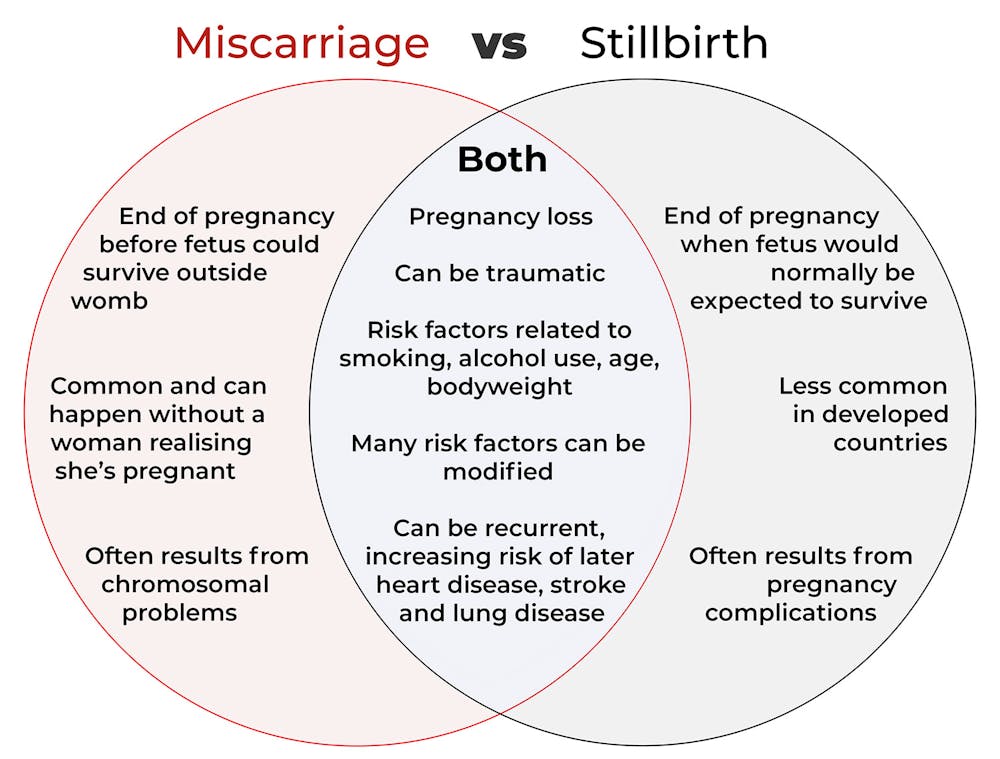
Both miscarriage and stillbirth are sadly familiar terms for pregnancy loss. They can be traumatic life events for the prospective parents and family, and their impacts can be long-lasting. But the terms can be confused.
Here are some similarities and differences between miscarriage and stillbirth, and why they matter.

christinarosepix/Shutterstock Let’s start with some definitions
In broad terms, a miscarriage is when a pregnancy ends while the fetus is not yet viable (before it could survive outside the womb).
This is the loss of an “intra-uterine” pregnancy, when an embryo is implanted in the womb to then develop into a fetus. The term miscarriage excludes ectopic pregnancies, where the embryo is implanted outside the womb.
However, stillbirth refers to the end of a pregnancy when the fetus is normally viable. There may have been sufficient time into the pregnancy. Alternatively, the fetus may have grown large enough to be normally expected to survive, but it dies in the womb or during delivery.
The Australian Institute of Health and Welfare defines stillbirth as a fetal death of at least 20 completed weeks of gestation or with a birthweight of at least 400 grams.
Internationally, definitions of stillbirth vary depending on the jurisdiction.
How common are they?
It is difficult to know how common miscarriages are as they can happen when a woman doesn’t know she is pregnant. There may be no obvious symptoms or something that looks like a heavier-than-normal period. So miscarriages are likely to be more common than reported.
Studies from Europe and North America suggest a miscarriage occurs in about one in seven pregnancies (15%). More than one in eight women (13%) will have a miscarriage at some time in her life.
Around 1–2% of women have recurrent miscarriages. In Australia this is when someone has three or more miscarriages with no pregnancy in between.
Australia has one of the lowest rates of stillbirth in the world. The rate has been relatively steady over the past 20 years at 0.7% or around seven per 1,000 pregnancies.
Who’s at risk?
Someone who has already had a miscarriage or stillbirth has an increased risk of that outcome again in a subsequent pregnancy.
Compared with women who have had a live birth, those who have had a stillbirth have double the risk of another. For those who have had recurrent miscarriages, the risk of another miscarriage is four-fold higher.
Some factors have a u-shaped relationship, with the risk of miscarriage and stillbirth lowest in the middle.
For instance, maternal age is a risk factor for both miscarriage and stillbirth, especially if under 20 years old or older than 35. Increasing age of the male is only a risk factor for stillbirth, especially for fathers over 40.
An older dad can be a risk factor for stillbirth, but not miscarriage. Elizaveta Galitckaia/Shutterstock Similarly for maternal bodyweight, women with a body mass index or BMI in the normal range have the lowest risk of miscarriage and stillbirth compared with those in the obese or underweight categories.
Lifestyle factors such as smoking and heavy alcohol drinking while pregnant are also risk factors for both miscarriage and stillbirth.
So it’s important to not only avoid smoking and alcohol while pregnant, but before getting pregnant. This is because early in the pregnancy, women may not know they have conceived and could unwittingly expose the developing fetus.
Why do they happen?
Miscarriage often results from chromosomal problems in the developing fetus. However, genetic conditions or birth defects account for only 7-14% of stillbirths.
Instead, stillbirths often relate directly to pregnancy complications, such as a prolonged pregnancy or problems with the umbilical cord.
Maternal health at the time of pregnancy is another contributing factor in the risk of both miscarriage and stillbirths.
Chronic diseases, such as high blood pressure, diabetes, hypothyroidism (underactive thyroid), polycystic ovary syndrome, problems with the immune system (such as an autoimmune disorder), and some bacterial and viral infections are among factors that can increase the risk of miscarriage.
Similarly mothers with diabetes, high blood pressure, and untreated infections, such as malaria or syphilis, face an increased risk of stillbirth.
In many cases, however, the specific cause of pregnancy loss is not known.
How about the long-term health risks?
Miscarriage and stillbirth can be early indicators of health issues later in life.
For instance, women who have had recurrent miscarriages or recurrent stillbirths are at higher risk of cardiovascular disease (such as heart disease or stroke).
Our research has also looked at the increased risk of stroke. Compared with women who had never miscarried, we found women with a history of three or more miscarriages had a 35% higher risk of non-fatal stroke and 82% higher risk of fatal stroke.
Women who had a stillbirth had a 31% higher risk of a non-fatal stroke, and those who had had two or more stillbirths were at a 26% higher risk of a fatal stroke.
We saw similar patterns in chronic obstructive pulmonary disease or COPD, a progressive lung disease with respiratory symptoms such as breathlessness and coughing.
Our data showed women with a history of recurrent miscarriages or stillbirths were at a 36% or 67% higher risk of COPD, respectively, even after accounting for a history of asthma.
Long-term health risks of recurrent miscarriages or stillbirths include developing lung disease later in life. PRPicturesProduction/Shutterstock Why is all this important?
Being well-informed about the similarities and differences between these two traumatic life events may help explain what has happened to you or a loved one.
Where risk factors can be modified, such as smoking and obesity, this information can be empowering for individuals who wish to reduce their risk of miscarriage and stillbirth and make lifestyle changes before they become pregnant.
More information and support about miscarriage and stillbirth is available from SANDS and Pink Elephants.
Gita Mishra, Professor of Life Course Epidemiology, Faculty of Medicine, The University of Queensland; Chen Liang, PhD student, reproductive history and non-communicable diseases in women, The University of Queensland, and Jenny Doust, Clinical Professorial Research Fellow, School of Public Health, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Peaceful Kitchen – by Catherine Perez
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The author, a keen cook and Registered Dietician with a Master’s in same, covers the basics of the science of nutrition as relevant to her recipes, but first and foremost this is not a science textbook—it’s a cookbook, and its pages contain more love for the art than citations for the (perfectly respectable) science.
Mexican and Dominican cuisine are the main influences in this book, but there are dishes from around the world too.
The recipes themselves are… Comparable in difficulty to the things we often feature in our recipes section here at 10almonds. They’re probably not winning any restaurants Michelin stars, but they’re not exactly student survival recipes either. They’re made from mostly non-obscure whole foods, nutritionally-dense ingredients at that, with minimal processed foods involved.
That said, she does take a “add, don’t subtract” approach to nutrition, i.e. focussing more on adding in diversity of plants than on “don’t eat this; don’t eat that” mandates.
If there’s any criticism to be levelled at the book, it’s that in most cases we’d multiply the spices severalfold, but that’s not a big problem as readers can always judge that individually; she’s given the basic information of which spices in which proportions, which is the key knowledge.
Bottom line: if you’re looking to expand your plant-based cooking repertoire, this one is a fine choice.
Click here to check out Peaceful Kitchen, and try some new things!
Share This Post



-
How extreme heat can affect you—and how you can protect yourself
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Because of climate change, last summer was the hottest in the Northern Hemisphere in 2,000 years—and this summer is expected to be even hotter. The record may continue to be broken: Extreme heat is expected to become even more frequent.
The scorching heat has led to an increase in heat-related deaths in the United States, according to the Department of Health and Human Services, with approximately 2,300 deaths in the summer of 2023. Extreme heat, defined as a period of two to three days with high heat and humidity with temperatures above 90 degrees Fahrenheit, can have serious health consequences, including symptoms like headache, dizziness, loss of consciousness, nausea, and confusion.
As we face more extreme heat, you may be wondering how you can protect yourself and your loved ones. Read on to learn about heat-related illness, who’s most at risk, and more.
What happens when our bodies are exposed to extreme heat?
As our body temperature rises, our bodies attempt to cool down by opening up more blood vessels near the skin to begin sweating. The evaporation of our sweat regulates our body temperature, but it also leads to losing fluids and minerals.
When it’s too humid, sweating alone doesn’t do the trick. The heart must work harder to bring blood around the body. It starts beating faster, which can cause light-headedness, nausea, and headache.
This process can affect our health in different ways, including increasing our risk of hospitalization for heart disease, worsening asthma, and injuring kidneys due to dehydration. It can also result in heat-related illness. Below are some effects of heat on our bodies:
- Heat cramps: Occur when a person loses salt through sweating, which causes painful cramps. Symptoms begin as painful spasms after heavy sweating, usually in the legs or the stomach. Heat cramps can lead to heat exhaustion or heat stroke.
- Heat exhaustion: This occurs when the body loses an excessive amount of water and salt, usually during intense physical activity. Symptoms include irritability, heavy sweating, and weakness, including muscle cramps. Heat exhaustion can lead to heat stroke.
- Heat stroke: This is the most severe heat-related illness. It happens when the body can’t cool down and reaches a temperature of 106 Fahrenheit or higher within 10 to 15 minutes. If the person doesn’t receive emergency treatment, it can cause permanent disability or death. Symptoms include confusion, loss of consciousness, and seizures.
What should I do if someone experiences a heat-related illness?
If you or someone you’re with begins to show signs of heat illness, the Centers for Disease Control and Prevention recommends the following:
- Heat cramps: Stop all physical activity, drink water or a sports drink, move to a cool place, and wait for cramps to go away before resuming activity. If the cramps last more than an hour, you’re on a low-sodium diet, or you have heart problems, get medical help.
- Heat exhaustion: Move the person to a cool place, loosen their clothes, use a cool bath or cloths to try to lower their body temperature, and give them a sip of water. If the person throws up, or if their symptoms last longer than an hour or worsen, get medical help.
- Heat stroke: Call 911 immediately. Then, move the person to a cooler place, use cool cloths or a cool bath to help lower their temperature, and don’t give them anything to drink.
Read more about heat-related illness and what to do in each case.
Who’s more vulnerable to extreme heat?
While everyone can be affected by extreme heat, some people are more at risk, including people of color.
A 2023 KFF report outlined that because of historical residential segregation in the U.S. (known as “redlining”), people of color are more likely to live in areas that experience higher temperatures from rooftops, asphalt, and sidewalks that retain the sun’s heat (known as the “urban heat island effect”). Additionally, communities of color are more likely to live in areas with fewer trees, which act as a canopy and provide shade, making the heat worse and more direct.
Children under 5, adults 65 or over, and pregnant people are also more vulnerable to extreme heat. If you have a chronic health condition like diabetes, heart problems, or a mental health condition, you’re also at higher risk. (Some psychiatric medications, like antidepressants, can also make people more susceptible to heat).
Lastly, anyone exposed to the sun and extreme heat for long periods is also at higher risk. This includes athletes, people who work outdoors, and unhoused people.
What can I do to prevent heat-related illness during a heat wave?
During a heat wave, follow these tips to stay cool and protect yourself from heat-related illness:
- Never leave your pets or children inside a car.
- Wear loose, light-colored clothing (dark colors absorb more heat).
- Find shade if you’re outside.
- If you don’t have air conditioning in your home, go to a place where you can cool down, such as a local library, community center, local pool or splash pad, or mall. Check to see if your city has designated cooling centers. (Cities like New York have a list of places.)
- Wear a hat.
- Drink (non-alcoholic) fluids often to stay hydrated—and if you have pets, give them water frequently as well.
- Check on your family members or older neighbors who may be more sensitive to extreme heat.
- Avoid using your stove or oven too often or during the hottest parts of the day.
- Cover your windows with shades to keep the heat out.
What are some resources to prevent heat-related illness?
If you need financial assistance to cool down your home, such as to purchase an air conditioner, apply to the federal government’s Low Income Home Energy Assistance Program.
Before you head outside during a heat wave, use the CDC’s HeatRisk tool: Enter your zip code to find the current heat risk in your area and get tips on what to do to stay safe with each risk level.
During a heat wave, also look for a cooling center in your state using the National Center for Healthy Housing’s list.
Check out the National Weather Service’s for more tips and resources.
For more information, talk to your health care provider.
This article first appeared on Public Good News and is republished here under a Creative Commons license.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Policosanol: A Rival To Statins, Without The Side Effects?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Policosanol (which can be extracted from various sources, but is mostly made from sugar cane extract) is marketed as lipid-lowering agent for improving cholesterol levels, but its research history has not been without controversy:
2001: it works!
After a lot of research in the 1990s, it came out of the gate strong in 2001, with:
❝Policosanol (5 and 10 mg/day) significantly decreased LDL-cholesterol (17.3% and 26.7%, respectively), total cholesterol (12.9% and 19.5%), as well as the ratios of LDL-cholesterol to high-density lipoprotein (HDL)-cholesterol (17.2% and 26.5%) and total cholesterol to HDL-cholesterol (16.3% and 21.0%) compared with baseline and placebo❞
This, by the way, is comparable in efficacy to the most powerful statins, but without the adverse side effects.
Source: Efficacy and tolerability of policosanol in hypercholesterolemic postmenopausal women
Furthermore, its effects were not limited to postmenopausal women, and additionally, it was found that 20mg/day was sufficient for optimal effects; 40mg worked exactly the same as 20mg:
2006–2010: we do not trust the Cubans!
After it had been marketed and used in much of the world for some years, extra scrutiny was brought upon it, because the initial studies had been performed by the same lab in Cuba, a commercial lab that had tested them for a private interest (i.e., a company selling the supplement):
Heart Beat: Policosanol: A sweet nothing for high cholesterol
And furthermore, US-based labs were unable to replicate the results:
Policosanols as Nutraceuticals: Fact or Fiction
The Cuban researchers countered that the composition of policosanol as produced in their lab was different than the composition of the policosanol as produced in the US labs, because of the purity of the ingredients used in the Cuban lab.
Which, on the face of it, could be true or could just be the claim of a commercial lab with an association with a company selling a product.
Of course, importing Cuban ingredients to test them in the US was not a reasonably accessible option for the US-based labs, because of the US’s embargo of Cuba. In principle it could be done, but unless there is already a huge clear profit incentive, research scientists are usually on their hands and knees begging for grants already, so getting extra funding for specially-important Cuban ingredients was not going to be likely.
2012: never mind, it does work after all!
An American meta-analysis of 4596 patients from 52 eligible studies (from around the world, so many of them not affected by the US’s embargo; some were from within the US using non-Cuban ingredients, though), found:
❝policosanol is more effective than plant sterols and stanols for LDL level reduction and more favorably alters the lipid profile, approaching antilipemic drug efficacy❞
Those last words there, to be clear, mean “yes, the original claim of being on a par with statins is at least more or less true”.
Source: Meta-Analysis of Natural Therapies for Hyperlipidemia: Plant Sterols and Stanols versus Policosanol
2018: also yes, the Cuban kind does get those extra-effective results, even when tested outside of Cuba
A Korean research team verified this; it’s quite straightforward so for brevity we’ll just drop links:
- Consumption of Cuban Policosanol Improves Blood Pressure and Lipid Profile via Enhancement of HDL Functionality in Healthy Women Subjects: Randomized, Double-Blinded, and Placebo-Controlled Study
- Long-Term Consumption of Cuban Policosanol Lowers Central and Brachial Blood Pressure and Improves Lipid Profile With Enhancement of Lipoprotein Properties in Healthy Korean Participants
Mystery resolved!
Want to try some?
We don’t sell it, but here for your convenience is an example product on Amazon—it’s not the Cuban kind, because the US’s trade embargo makes it difficult for the US to import even things that are theoretically now exempt from the embargo such as food and medicines. In principle they can now be imported, but in practice, the extra regulations added to Cuban imports make it nearly impossible, especially for small sellers.
Still, it’s 40mg/tablet policosanol from sugar cane extract, and 3rd party lab tested, so it’s the next best thing 😎
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Alpha, beta, theta: what are brain states and brain waves? And can we control them?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There’s no shortage of apps and technology that claim to shift the brain into a “theta” state – said to help with relaxation, inward focus and sleep.
But what exactly does it mean to change one’s “mental state”? And is that even possible? For now, the evidence remains murky. But our understanding of the brain is growing exponentially as our methods of investigation improve.
Brain-measuring tech is evolving
Currently, no single approach to imaging or measuring brain activity gives us the whole picture. What we “see” in the brain depends on which tool we use to “look”. There are myriad ways to do this, but each one comes with trade-offs.
We learnt a lot about brain activity in the 1980s thanks to the advent of magnetic resonance imaging (MRI).
Eventually we invented “functional MRI”, which allows us to link brain activity with certain functions or behaviours in real time by measuring the brain’s use of oxygenated blood during a task.
We can also measure electrical activity using EEG (electroencephalography). This can accurately measure the timing of brain waves as they occur, but isn’t very accurate at identifying which specific areas of the brain they occur in.
Alternatively, we can measure the brain’s response to magnetic stimulation. This is very accurate in terms of area and timing, but only as long as it’s close to the surface.
What are brain states?
All of our simple and complex behaviours, as well as our cognition (thoughts) have a foundation in brain activity, or “neural activity”. Neurons – the brain’s nerve cells – communicate by a sequence of electrical impulses and chemical signals called “neurotransmitters”.
Neurons are very greedy for fuel from the blood and require a lot of support from companion cells. Hence, a lot of measurement of the site, amount and timing of brain activity is done via measuring electrical activity, neurotransmitter levels or blood flow.
We can consider this activity at three levels. The first is a single-cell level, wherein individual neurons communicate. But measurement at this level is difficult (laboratory-based) and provides a limited picture.
As such, we rely more on measurements done on a network level, where a series of neurons or networks are activated. Or, we measure whole-of-brain activity patterns which can incorporate one or more so-called “brain states”.
According to a recent definition, brain states are “recurring activity patterns distributed across the brain that emerge from physiological or cognitive processes”. These states are functionally relevant, which means they are related to behaviour.
Brain states involve the synchronisation of different brain regions, something that’s been most readily observed in animal models, usually rodents. Only now are we starting to see some evidence in human studies.
Various kinds of states
The most commonly-studied brain states in both rodents and humans are states of “arousal” and “resting”. You can picture these as various levels of alertness.
Studies show environmental factors and activity influence our brain states. Activities or environments with high cognitive demands drive “attentional” brain states (so-called task-induced brain states) with increased connectivity. Examples of task-induced brain states include complex behaviours such as reward anticipation, mood, hunger and so on.
In contrast, a brain state such as “mind-wandering” seems to be divorced from one’s environment and tasks. Dropping into daydreaming is, by definition, without connection to the real world.
We can’t currently disentangle multiple “states” that exist in the brain at any given time and place. As mentioned earlier, this is because of the trade-offs that come with recording spatial (brain region) versus temporal (timing) brain activity.
Brain states vs brain waves
Brain state work can be couched in terms such as alpha, delta and so forth. However, this is actually referring to brain waves which specifically come from measuring brain activity using EEG.
EEG picks up on changing electrical activity in the brain, which can be sorted into different frequencies (based on wavelength). Classically, these frequencies have had specific associations:
- gamma is linked with states or tasks that require more focused concentration
- beta is linked with higher anxiety and more active states, with attention often directed externally
- alpha is linked with being very relaxed, and passive attention (such as listening quietly but not engaging)
- theta is linked with deep relaxation and inward focus
- and delta is linked with deep sleep.
Brain wave patterns are used a lot to monitor sleep stages. When we fall asleep we go from drowsy, light attention that’s easily roused (alpha), to being relaxed and no longer alert (theta), to being deeply asleep (delta).
Can we control our brain states?
The question on many people’s minds is: can we judiciously and intentionally influence our brain states?
For now, it’s likely too simplistic to suggest we can do this, as the actual mechanisms that influence brain states remain hard to detangle. Nonetheless, researchers are investigating everything from the use of drugs, to environmental cues, to practising mindfulness, meditation and sensory manipulation.
Controversially, brain wave patterns are used in something called “neurofeedback” therapy. In these treatments, people are given feedback (such as visual or auditory) based on their brain wave activity and are then tasked with trying to maintain or change it. To stay in a required state they may be encouraged to control their thoughts, relax, or breathe in certain ways.
The applications of this work are predominantly around mental health, including for individuals who have experienced trauma, or who have difficulty self-regulating – which may manifest as poor attention or emotional turbulence.
However, although these techniques have intuitive appeal, they don’t account for the issue of multiple brain states being present at any given time. Overall, clinical studies have been largely inconclusive, and proponents of neurofeedback therapy remain frustrated by a lack of orthodox support.
Other forms of neurofeedback are delivered by MRI-generated data. Participants engaging in mental tasks are given signals based on their neural activity, which they use to try and “up-regulate” (activate) regions of the brain involved in positive emotions. This could, for instance, be useful for helping people with depression.
Another potential method claimed to purportedly change brain states involves different sensory inputs. Binaural beats are perhaps the most popular example, wherein two different wavelengths of sound are played in each ear. But the evidence for such techniques is similarly mixed.
Treatments such as neurofeedback therapy are often very costly, and their success likely relies as much on the therapeutic relationship than the actual therapy.
On the bright side, there’s no evidence these treatment do any harm – other than potentially delaying treatments which have been proven to be beneficial.

Susan Hillier, Professor: Neuroscience and Rehabilitation, University of South Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: