What’s the difference between miscarriage and stillbirth?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What’s the difference? is a new editorial product that explains the similarities and differences between commonly confused health and medical terms, and why they matter.
Former US First Lady Michelle Obama revealed in her memoir she had a miscarriage. UK singer-songwriter and actor Lily Allen has gone on the record about her stillbirth.
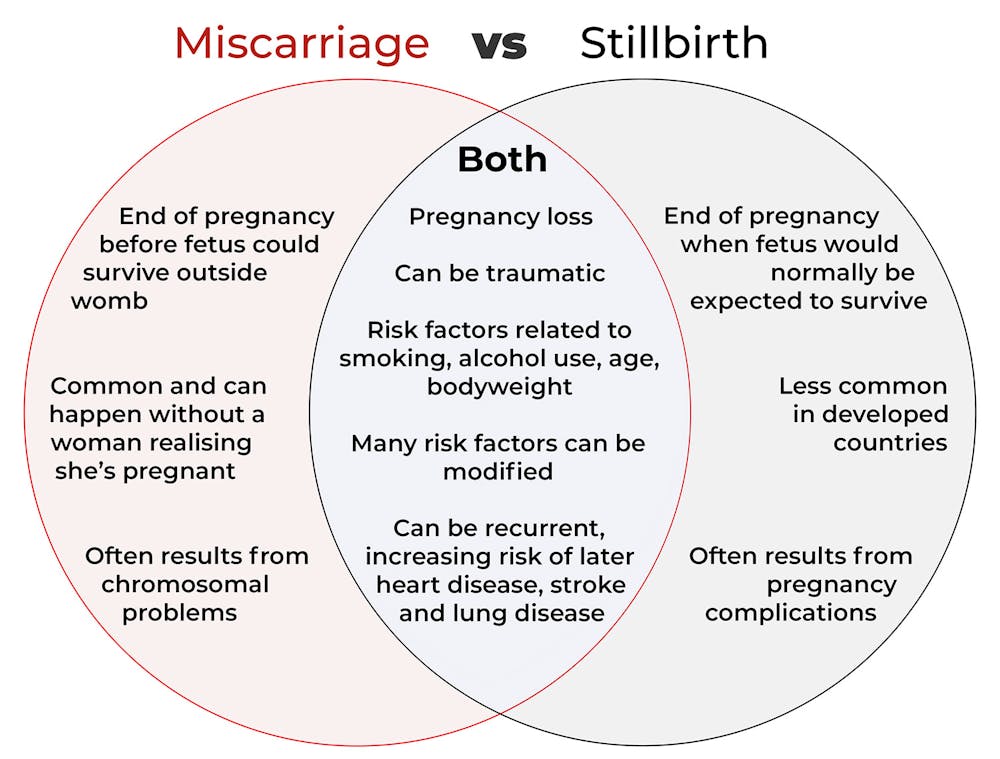
Both miscarriage and stillbirth are sadly familiar terms for pregnancy loss. They can be traumatic life events for the prospective parents and family, and their impacts can be long-lasting. But the terms can be confused.
Here are some similarities and differences between miscarriage and stillbirth, and why they matter.

Let’s start with some definitions
In broad terms, a miscarriage is when a pregnancy ends while the fetus is not yet viable (before it could survive outside the womb).
This is the loss of an “intra-uterine” pregnancy, when an embryo is implanted in the womb to then develop into a fetus. The term miscarriage excludes ectopic pregnancies, where the embryo is implanted outside the womb.
However, stillbirth refers to the end of a pregnancy when the fetus is normally viable. There may have been sufficient time into the pregnancy. Alternatively, the fetus may have grown large enough to be normally expected to survive, but it dies in the womb or during delivery.
The Australian Institute of Health and Welfare defines stillbirth as a fetal death of at least 20 completed weeks of gestation or with a birthweight of at least 400 grams.
Internationally, definitions of stillbirth vary depending on the jurisdiction.
How common are they?
It is difficult to know how common miscarriages are as they can happen when a woman doesn’t know she is pregnant. There may be no obvious symptoms or something that looks like a heavier-than-normal period. So miscarriages are likely to be more common than reported.
Studies from Europe and North America suggest a miscarriage occurs in about one in seven pregnancies (15%). More than one in eight women (13%) will have a miscarriage at some time in her life.
Around 1–2% of women have recurrent miscarriages. In Australia this is when someone has three or more miscarriages with no pregnancy in between.
Australia has one of the lowest rates of stillbirth in the world. The rate has been relatively steady over the past 20 years at 0.7% or around seven per 1,000 pregnancies.
Who’s at risk?
Someone who has already had a miscarriage or stillbirth has an increased risk of that outcome again in a subsequent pregnancy.
Compared with women who have had a live birth, those who have had a stillbirth have double the risk of another. For those who have had recurrent miscarriages, the risk of another miscarriage is four-fold higher.
Some factors have a u-shaped relationship, with the risk of miscarriage and stillbirth lowest in the middle.
For instance, maternal age is a risk factor for both miscarriage and stillbirth, especially if under 20 years old or older than 35. Increasing age of the male is only a risk factor for stillbirth, especially for fathers over 40.

Similarly for maternal bodyweight, women with a body mass index or BMI in the normal range have the lowest risk of miscarriage and stillbirth compared with those in the obese or underweight categories.
Lifestyle factors such as smoking and heavy alcohol drinking while pregnant are also risk factors for both miscarriage and stillbirth.
So it’s important to not only avoid smoking and alcohol while pregnant, but before getting pregnant. This is because early in the pregnancy, women may not know they have conceived and could unwittingly expose the developing fetus.
Why do they happen?
Miscarriage often results from chromosomal problems in the developing fetus. However, genetic conditions or birth defects account for only 7-14% of stillbirths.
Instead, stillbirths often relate directly to pregnancy complications, such as a prolonged pregnancy or problems with the umbilical cord.
Maternal health at the time of pregnancy is another contributing factor in the risk of both miscarriage and stillbirths.
Chronic diseases, such as high blood pressure, diabetes, hypothyroidism (underactive thyroid), polycystic ovary syndrome, problems with the immune system (such as an autoimmune disorder), and some bacterial and viral infections are among factors that can increase the risk of miscarriage.
Similarly mothers with diabetes, high blood pressure, and untreated infections, such as malaria or syphilis, face an increased risk of stillbirth.
In many cases, however, the specific cause of pregnancy loss is not known.
How about the long-term health risks?
Miscarriage and stillbirth can be early indicators of health issues later in life.
For instance, women who have had recurrent miscarriages or recurrent stillbirths are at higher risk of cardiovascular disease (such as heart disease or stroke).
Our research has also looked at the increased risk of stroke. Compared with women who had never miscarried, we found women with a history of three or more miscarriages had a 35% higher risk of non-fatal stroke and 82% higher risk of fatal stroke.
Women who had a stillbirth had a 31% higher risk of a non-fatal stroke, and those who had had two or more stillbirths were at a 26% higher risk of a fatal stroke.
We saw similar patterns in chronic obstructive pulmonary disease or COPD, a progressive lung disease with respiratory symptoms such as breathlessness and coughing.
Our data showed women with a history of recurrent miscarriages or stillbirths were at a 36% or 67% higher risk of COPD, respectively, even after accounting for a history of asthma.

Why is all this important?
Being well-informed about the similarities and differences between these two traumatic life events may help explain what has happened to you or a loved one.
Where risk factors can be modified, such as smoking and obesity, this information can be empowering for individuals who wish to reduce their risk of miscarriage and stillbirth and make lifestyle changes before they become pregnant.
More information and support about miscarriage and stillbirth is available from SANDS and Pink Elephants.
Gita Mishra, Professor of Life Course Epidemiology, Faculty of Medicine, The University of Queensland; Chen Liang, PhD student, reproductive history and non-communicable diseases in women, The University of Queensland, and Jenny Doust, Clinical Professorial Research Fellow, School of Public Health, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Real Way To Eat More Veg If You Don’t Like Veg

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Let us start by assuming you’re aware you can blend them into a soup. Juicing is also an option.
Turning vegetables into a liquid will keep most of their nutrients, but be aware that soup-ifying will lose some fiber, and juicing will lose all (or nearly all) of the fiber.
See also: Can you drink your fruit and vegetables? How does juice compare to the whole food?
If you do opt for juicing, please have it alongside something that’s not juice, because otherwise it will wreak havoc on your gut:
3 Day Juice Fasting? Not So Fast!
…not to mention your blood sugar levels:
Fruit Is Healthy; Juice Isn’t (Here’s Why)
For a deeper dive into the physiology of why that happens, check out: Which Sugars Are Healthier, And Which Are Just The Same?
Ask yourself one question
No, this isn’t about whether you feel lucky. Rather, the question is:
Why don’t you like veg?
To be clear, this is not challenging you to justify your dislike. Your likes and dislikes require no justification; they simply are.
But! It is important, to be able to proceed with this, for you to understand what it is about veg that you don’t like.
- For some people it’s the flavors (in which case cooking vigorously will kill most flavors)
- For some it’s the lack of flavors (in which case, time to go light on the cooking, heavy on the seasoning)
- For some, it’s the textures (needing them to not be soft)
- For some, it’s the textures (needing them to not be varied)
- For some, it’s about needing to do too much prep (needing something easier)
With regard to “too much flavor”, as we say, that’s easy; just cook it more and the flavor will go. Yes, you’ll probably lose some nutrients too, but you’ll still get some.
With regard to “not enough flavor”, then by all means cook them less, where safely possible (for example, potatoes are poisonous raw, so please still cook those). See also:
Make Your Vegetables Work Better Nutritionally ← this is about which veg you should cook more or less or differently, for optimal nutrients
And to add the healthiest extra flavors of all: Our Top 5 Spices: How Much Is Enough For Benefits?
With regard to needing them to not be soft, most are good raw, e.g. carrots, celery, bell peppers, cucumber, as some top items.
Remember also that salad doesn’t have to have soft leaves! You can make it out of anything you want; nobody can stop you!
See for example: Supergreen Superfood Salad Slaw ← so very crunchy!
If you are cooking, though, remember that you can choose vegetables will stay crunchy if cooked lightly (for example just quickly stir-frying), such as sugarsnap peas, cabbage, water chestnuts, Brussels sprouts (slice them!), bamboo shoots, etc.
With regard to needing the textures to not be varied, that usually means making them soft, and simply means cooking them generously. It’s possible that you might not like the smell of some vegetables while cooking (cruciferous vegetables are a common one for this complaint), so you might want to just skip those ones.
There are also ways of getting in things that are soft and homogenous without cooking, so such hummus, guacamole, and other similar dips!
With regard to needing it to require less prep, buy things ready-prepped as much as you can! Get in that frozen veg, or canned, it’s all good. Or even just ready-prepared stir-fry veg that you just need to toss into a wok.
We’ll tell you an extra secret: you can even literally just order take-out of your favorite vegetable dishes. Yes, there’ll probably be a bit more salt and maybe even sugar than you might use at home, but you’re getting vegetables in, and a positive attitude to diet (i.e., focusing on what to include, rather than what to exclude) will almost always result in the heathiest balance.
Also, getting things ready mixed (e.g. mixed frozen veg over separate) also cuts down on prep time and things you need to do. similarly, some of the things we mentioned earlier are zero-prep if bought ready-made, e.g. the hummus, guacamole, etc.
Still not a fan of veg?
All is not lost. As it turns out, fruit and vegetable extracts are still beneficial even in supplement form!
See: Are Fruit & Vegetable Extract Supplements Worth It?
Take care!
Share This Post
-

Your Future Self – by Dr. Hal Herschfield
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How do you want to be, one year from now? Five years from now? Ten years from now?
Now, how would you have answered that same question one, five, ten years ago?
The reality, according to Dr. Hal Herschfield, is that often we go blundering into the future blindly, because we lack empathy with our future self. Our past self, we can have strong feelings about. They could range from compassion to shame, pride to frustration, but we’ll have feelings. Our future self? A mystery.
What he proposes in this book, therefore, is not merely the obvious “start planning now, little habits that add up”, etc, but also to address the underlying behavioral science of why we don’t.
Starting with exercises of empathy for our tomorrow-self (literally tomorrow, i.e. the day after this one), and building a mindset of “paying it forward”—to ourself.
By treating our future self like a loved one, we can find ourselves a lot more motivated to actually do the things that future-us will thank us for.
The real value of this book is in the progressive exercises, because it’s a “muscle” that most people haven’t exercised much. But when we do? What a superpower it becomes!
Bottom line: if you know what you “should” do, but somehow just don’t do it, this book will help connect you to your future self and work as a better team to get there… the way you actually want.
Click here to check out Your Future Self, and start by gifting this book to future-you!
Share This Post
-

The Brain As A Work-In-Progress
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
And The Brain Goes Marching On!

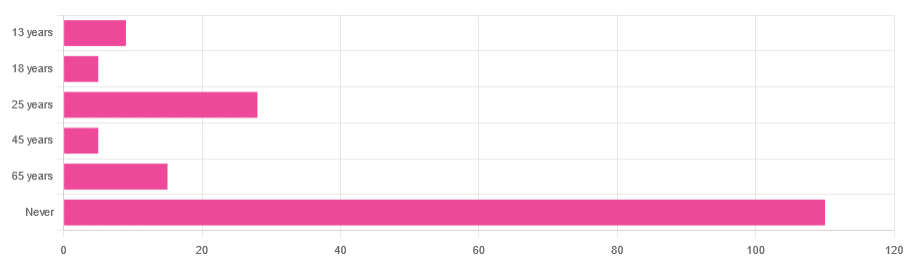
In Tuesday’s newsletter, we asked you “when does the human brain stop developing?” and got the above-depicted, below-described, set of responses:
- About 64% of people said “Never”
- About 16% of people said “25 years”
- About 9% of people said “65 years”
- About 5% of people said “13 years”
- About 3% of people said “18 years”
- About 3% of people said “45 years”
Some thoughts, before we get into the science:
An alternative wording for the original question was “when does the human brain finish developing”; the meaning is the same but the feeling is slightly different:
- “When does the human brain stop developing?” focuses attention on the idea of cessation, and will skew responses to later ages
- When does the human brain finish developing?” focuses on attention on a kind of “is it done yet?” and will skew responses to earlier ages
Ultimately, since we had to chose one word or another, we picked the shortest one, but it would have been interesting if we could have done an A/B test, and asked half one way, and half the other way!
Why we picked those ages
We picked those ages as poll options for reasons people might be drawn to them:
- 13 years: in English-speaking cultures, an important milestone of entering adolescence (note that the concept of a “teenager” is not precisely universal as most languages do not have “-teen” numbers in the same way; the concept of “adolescent” may thus be tied to other milestones)
- 18 years: age of legal majority in N. America and many other places
- 25 years: age popularly believed to be when the brain is finished developing, due to a study that we’ll talk about shortly (we guess that’s why there’s a spike in our results for this, too!)
- 45 years: age where many midlife hormonal changes occur, and many professionals are considered to have peaked in competence and start looking towards retirement
- 65 years: age considered “senior” in much of N. America and many other places, as well as the cut-off and/or starting point for a lot of medical research
Notice, therefore, how a lot of things are coming from places they really shouldn’t. For example, because there are many studies saying “n% of people over 65 get Alzheimer’s” or “n% of people over 65 get age-related cognitive decline”, etc, 65 becomes the age where we start expecting this—because of an arbitrary human choice of where to draw the cut-off for the study enrollment!
Similarly, we may look at common ages of legal majority, or retirement pensions, and assume “well it must be for a good reason”, and dear reader, those reasons are more often economically motivated than they are biologically reasoned.
So, what does the science say?
Our brains are never finished developing: True or False?
True! If we define “finished developing” as “we cease doing neurogenesis and neuroplasticity is no longer in effect”.
Glossary:
- Neurogenesis: the process of creating new brain cells
- Neuroplasticity: the process of the brain adapting to changes by essentially rebuilding itself to suit our perceived current needs
We say “perceived” because sometimes neuroplasticity can do very unhelpful things to us (e.g: psychological trauma, or even just bad habits), but on a biological level, it is always doing its best to serve our overall success as an organism.
For a long time it was thought that we don’t do neurogenesis at all as adults, but this was found to be untrue:
How To Grow New Brain Cells (At Any Age)
Summary of conclusions of the above: we’re all growing new brain cells at every age, even if we be in our 80s and with Alzheimer’s disease, but there are things we can do to enhance our neurogenic potential along the way.
Neuroplasticity will always be somewhat enhanced by neurogenesis (after all, new neurons get given jobs to do), and we reviewed a great book about the marvels of neuroplasticity including in older age:
Our brains are still developing up to the age of 25: True or False?
True! And then it keeps on developing after that, too. Now this is abundantly obvious considering what we just talked about, but see what a difference the phrasing makes? Now it makes it sound like it stops at 25, which this statement doesn’t claim at all—it only speaks for the time up to that age.
A lot of the popular press about “the brain isn’t fully mature until the age of 25” stems from a 2006 study that found:
❝For instance, frontal gray matter volume peaks at about age 11.0 years in girls and 12.1 years in boys, whereas temporal gray matter volume peaks at about age at 16.7 years in girls and 16.2 years in boys. The dorsal lateral prefrontal cortex, important for controlling impulses, is among the latest brain regions to mature without reaching adult dimensions until the early 20s.❞
Source: Structural Magnetic Resonance Imaging of the Adolescent Brain
There are several things to note here:
- The above statement is talking about the physical size of the brain growing
- Nowhere does he say “and stops developing at 25”
However… The study only looked at brains up to the age of 25. After that, they stopped looking, because the study was about “the adolescent brain” so there has to be a cut-off somewhere, and that was the cut-off they chose.
This is the equivalent of saying “it didn’t stop raining until four o’clock” when the reality is that four o’clock is simply when you gave up on checking.
The study didn’t misrepresent this, by the way, but the popular press did!
Another 2012 study looked at various metrics of brain development, and found:
- Synapse overproduction into the teens
- Cortex pruning into the late 20s
- Prefrontal pruning into middle age at least (they stopped looking)
- Myelination beyond middle age (they stopped looking)
Source: Experience and the developing prefrontal cortex ← check out figure 1, and make sure you’re looking at the human data not the rat data
So how’s the most recent research looking?
Here’s a 2022 study that looked at 123,984 brain scans spanning the age range from mid-gestation to 100 postnatal years, and as you can see from its own figure 1… Most (if not all) brain-things keep growing for life, even though most slow down at some point, they don’t stop:
Brain charts for the human lifespan ← check out figure 1; don’t get too excited about the ventricular volume column as that is basically “brain that isn’t being a brain”. Do get excited about the rest, though!
Want to know how not to get caught out by science being misrepresented by the popular press? Check out:
How Science News Outlets Can Lie To You (Yes, Even If They Cite Studies!)
Take care!
Share This Post

-

What Teas To Drink Before Bed (By Science!)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Which Sleepy Tea?
Herbal “tea” preparations (henceforth we will write it without the quotation marks, although these are not true teas) are popular for winding down at the end of a long day ready for a relaxing sleep.
Today we’ll look at the science for them! We’ll be brief for each, because we’ve selected five and have only so much room, but here goes:
Camomile
Simply put, it works and has plenty of good science for it. Here’s just one example:
❝Noteworthy, our meta-analysis showed a significant improvement in sleep quality after chamomile administration❞
Also this writer’s favourite relaxation drink!
(example on Amazon if you want some)
Lavender
We didn’t find robust science for its popularly-claimed sedative properties, but it does appear to be anxiolytic, and anxiety gets in the way of sleep, so while lavender may not be a sedative, it may calm a racing mind all the same, thus facilitating better sleep:
(example on Amazon if you want some)
Magnolia
Animal study for the mechanism:
Human study for “it is observed to help humans sleep better”:
As you can see from the title, its sedative properties weren’t the point of the study, but if you click through to read it, you can see that they found (and recorded) this benefit anyway
(example on Amazon if you want some)
Passionflower
There’s not a lot of evidence for this one, but there is some. Here’s a small study (n=41) that found:
❝Of six sleep-diary measures analysed, sleep quality showed a significantly better rating for passionflower compared with placebo (t(40) = 2.70, p < 0.01). These initial findings suggest that the consumption of a low dose of Passiflora incarnata, in the form of tea, yields short-term subjective sleep benefits for healthy adults with mild fluctuations in sleep quality.❞
So, that’s not exactly a huge body of evidence, but it is promising.
(example on Amazon if you want some)
Valerian
We’ll be honest, the science for this one is sloppy. It’s very rare to find Valerian tested by itself (or sold by itself; we had to dig a bit to find one for the Amazon link below), and that skews the results of science and renders any conclusions questionable.
And the studies that were done? Dubious methods, and inconclusive results:
Nevertheless, if you want to try it for yourself, you can do a case study (i.e., n=1 sample) if not a randomized controlled trial, and let us know how it goes 🙂
(example on Amazon if you want some)
Summary
- Valerian we really don’t have the science to say anything about it
- Passionflower has some nascent science for it, but not much
- Lavender is probably not soporific, but it is anxiolytic
- Magnolia almost certainly helps, but isn’t nearly so well-backed as…
- Camomile comes out on top, easily—by both sheer weight of evidence, and by clear conclusive uncontroversial results.
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Apricot vs Cantaloupe – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing apricots to cantaloupe, we picked the apricots.
Why?
In terms of macros, apricots have 2x the fiber, for slightly more carbs and protein, winning in this first category.
In the category of vitamins, apricots have more of vitamins B2, B5, B7, E, and K, while cantaloupe has more of vitamins A, B1, B6, B9, and C, which would be a 5:5 tie, but it’s worth noticing the outlier that is the huge margin of difference when it comes to apricots having nearly 17x more vitamin E, so we say apricots win this round.
Looking at minerals, apricots have more calcium, copper, iron, manganese, phosphorus, and zinc, while cantaloupe has more magnesium, potassium, and selenium yielding a tidy 6:3 win to apricots here.
In other considerations, apricots are much higher in polyphenols, and also have some specific anticancer properties that cantaloupe can’t boast, so that’s another round in apricots’ favor.
Adding up the sections makes for a clear overall win for apricots, but by all means do enjoy either or both, as diversity is best!
Want to learn more?
You might like:
Top 8 Fruits That Prevent & Kill Cancer
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Should I kick my diet soft-drink habit? Where do I start?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The average Australian drinks almost 60 litres of soft drink a year. Many people see diet soft drinks as a “healthier” choice than regular ones, and when it comes to sugar, that’s true.
For example, a 375 millilitre can of Coca-Cola contains about seven teaspoons of added sugar (almost to 40 grams). That’s close to the World Health Organization’s (WHO) daily recommended limit for added sugars of 50g.
In comparison, the Diet Coke version is sweetened with artificial sweeteners such as aspartame and does not contain sugar.
So if you reach for diet soft drinks, is that so bad? Or is it worth giving them up too?

Towfiqu barbhuiya/Pexels Are diet soft drinks really that bad?
Diet soft drinks provide few nutrients. They often contain artificial sweeteners and caffeine, and while they’re low in energy (kilojoules), they aren’t filling.
People who regularly drink diet soft drinks may have a higher risk of developing conditions such as heart disease and type 2 diabetes.
But this doesn’t necessarily mean the drinks cause these conditions. People who already have health concerns or are trying to manage their weight may be more likely to choose diet drinks, which might make this evidence a little misleading.
How about artificial sweeteners?
In 2023, the WHO classified aspartame (a common sweetener found in many diet soft drinks) as “possibly carcinogenic to humans”. This means the evidence linking aspartame to cancer is currently limited and not conclusive.
The WHO also emphasised that the public generally consumes safe levels of aspartame and only has evidence for concern if people drink the equivalent to 14 cans of soft drink a day.
There is also emerging evidence some artificial sweeteners might irritate the gut or alter the balance of gut bacteria. These effects are still being investigated. But they’ve added to concerns about the health impacts of drinking diet soft drinks over a long period of time.
Can I get used to the sweetness?
An occasional diet drink isn’t likely to fuel an addiction to sweet foods, but cutting back is still a good idea if this has become a daily habit.
After people cut back on very sweet foods or drinks, some research suggests they start noticing sweetness more easily and find very sweet things taste too sweet.
So if you’re trying to enjoy less-sweet drinks, give it time. Within a few weeks you might actually prefer the less-sweet taste.
Here are three evidence-based strategies to help you adjust.
1. Water it down
A gentle first step is to dilute your soft drink. Start by pouring less soft drink into a glass and topping it up with water or soda water, then gradually adjust the ratio over time.
It may taste less sweet at first, but your taste buds will adapt. This slow, steady approach can make change feel easier and more sustainable than quitting abruptly.
2. Make smarter swaps
Try replacing diet soft drink with a healthier alternative that still delivers flavour or fizz. Sparkling water or soda water with a squeeze of lime or lemon and a few mint leaves gives you the same bubbly refreshment with a natural and refreshing flavour. Add ice if it is a hot day, or to provide some crunch.
If you prefer plain water but it feels boring, infuse it with slices of fruit, cucumber, berries or herbs.
You could also try unsweetened iced tea, such as black, green or herbal tea. These offer a mild caffeine lift without the added sweeteners and can be served cold with ice and lemon.
Coconut water can also be a healthier alternative as it is low in sugar while providing some additional electrolytes, which help balance fluid in the body.
3. Know your triggers
If you often reach for a soft drink out of habit, boredom or an afternoon energy slump, paying attention to these moments can help. Once you spot your triggers, you can plan a different response. Take a short walk, call a friend or make a cup of tea instead.
Keeping a chilled, reusable water bottle nearby also helps. If your drink is always within reach, you’re less likely to grab a diet soft drink when you’re out and about.
If you drink diet soft drinks because you’re hungry, reach for something nourishing instead, such as a handful of nuts, a yoghurt or a piece of fruit. These foods will satisfy you for longer than a can of diet soft drink because they have nutrients, such as fibre, to keep you fuller for longer.
The bottom line
You don’t have to give up diet soft drinks altogether. But being mindful of how much soft drink you drink, and how often, can help you make choices that better support your long-term health.
Start small, be consistent and let your taste buds adjust. Over time, you might find what once tasted “flat” now feels refreshingly natural.
Lauren Ball, Professor of Community Health and Wellbeing, The University of Queensland; Emily Burch, Accredited Practising Dietitian and Lecturer, Southern Cross University, and Mackenzie Derry, Nutritionist, Dietitian & PhD Candidate, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: